
Abstract
The study of nasal ciliary beat frequency (CBF) and ultrastructure may contribute to the understanding of pathognomonic cases of male infertility associated with defects in sperm motility. This study was designed to report a particular case of male infertility, characterized by the association of two respiratory autosomal recessive genetic diseases (alpha-1-antitrypsin deficiency [AAT-D] and primary ciliary dyskinesia [PCD]). A 39-year-old patient with complete sperm immotility, AAT-D, and bronchiectasis was studied in the Laboratory of Male Fertility, the Department of Urology, the Respiratory Center of a Pediatric Hospital, and in the Department of Clinical Medicine of a Rehabilitation Respiratory Hospital. Family history, physical examination, hormonal analysis, microbial assays, semen analysis, nasal ciliary function, and structure study by digital high-speed video photography and transmission electron microscopy are described. A noninvasive nasal biopsy to retrieve ciliated epithelium lining the inferior surface of the inferior nasal turbinates was performed and CBF was determined. Beat pattern was slightly curved and rigid, not wide, and metacronic in all the observed fields analyzed. CBF was 8.2 Hz in average (reference value, 10–15 Hz) Ultrastructural assay revealed absence of the inner dynein arms in 97% of the cilia observed. The final infertility accurate diagnosis was achieved by the study of nasal CBF and ultrastructure contributing to the patient health management and genetic counseling while deciding fatherhood. Beyond this particular case, the present report may open a new field of studies in male infertility, mainly in cases of asthenozoospermia.
Complete sperm immotility is rarely described in the andrology laboratory (frequency 1 of 5000 males). 6 If necrozoospermia (high percentage of immotile spermatozoa in the ejaculate and low percentage of live, below the lower reference limit of 58% 4 ) is discarded and a very homogenous microscopic pattern is observed where the sperm structural defect is systematic, a genetic origin implying cilia distributed ubiquity should be suspected.
In the nodal cells there is always a 9 + 0 arrangement but the axoneme of sperm flagella as well as of motile cilia on respiratory, oviduct, and ependymal epithelial cells are comprised of a “9 + 2” microtubule arrangement, with 9 outer microtubule doublets surrounding a single central pair. Outer dynein arms associated with the outer microtubule doublets provide the motor force required for ciliary and flagellar beating. In addition, nexin links consist of the dynein regulatory complex and connect the neighboring outer microtubule doublets, and radial spokes link the outer doublets to the central pair.
Defects in motile ciliary and flagellar function commonly result in the primary ciliary dyskinesia (PCD) syndrome; patients commonly suffer from chronic sinusitis, bronchiectasis, neonatal respiratory distress, and male infertility. The Kartagener's syndrome is a subset of PCD where situs inversus is present. 7
Before the era of intracytoplasmic sperm injection, patients with this alteration were considered to be sterile but since the introduction of this technique they have the chance to procreate. Their decision should be based on an adequate genetic counseling and thus a correct and clear diagnosis of the cause of their infertility is necessary.
We have recorded three cases with normal sperm count but complete sperm immotility in our clinic during the last 3 years; one having 97% of dead sperm, the second with viable cells finally diagnosed as PCD (defects in both dynein arms) and the third one that motivated this publication.
The aim of this work was to describe the rare association of two autosomal recessive genetic diseases in a patient suffering from respiratory pathology and infertility. The final diagnosis was achieved indirectly by studying the dynamic and structure of nasal cilia by a novel method.
Materials and Methods
This study was approved by the Institutional Review Board of The Hospital de Clinicas “José de San Martin.”
Patient
An adult man with absence of sperm motility was the subject of this study. The patient (39 years old) came to our center for semen analysis after 6 years of sexual intercourse without conception. He was informed of and gave written consent for the procedures related to the study.
Medical History and Laboratory Data
The patient was a nonsmoker, by the age of 13 years had had dyspnea, and since then he had been treated for asthma. He has two sisters and nine brothers, all of them fertile except for one brother with the same respiratory failure and infertility that has not been examined yet.
The α-1-antitrypsin deficiency (AAT-D) dosage was performed at the very beginning, much before the ciliary function and structure were known. It is a simple test included in our algorithm to begin studying our patients, to understand the origin of bronchiectasis. Serum concentration of AAT-D was 122 mg/dL (reference value, >150 mg/dL); the genetic study showed up an MZ phenotype. Computed tomography of the chest revealed bronchiectasis localized mainly in the right upper and middle lobes and both bases. Spirometry showed ventilatory incapacity of moderate grade (forced expiratory volume in 1 second, 2.5 L. (71%); forced vital capacity, 5.09 L [118%]; forced expiratory volume in 1 second/forced vital capacity, 49%-obstructive pattern), 98% blood oxygen saturation, and class II functional dyspnea. The patient had frontal sinus agenesis. Haemophilus influenzae in sputum culture was developed. Maxillare bilateral sinusitis was diagnosed by tomography of paranasal sinuses.
Ultrasonography indicated normal testis size although in both epididymal caputs 1 cm cysts were observed. Varicocele and hydrocele were discarded as well as urine or sperm infections (negative for chlamydia, mycoplasma, and ureaplasma). Physical examination and reproductive endocrine evaluation were within standard ranges.
Semen Analysis
Semen sample was collected by masturbation after 3 days of sexual abstinence and examined after liquefaction for 30 minutes at 37°C. Volume, pH, concentration, and motility were evaluated according to World Health Organization guidelines. 4 The sample was stained with 0.5% eosin Y in 0.9% aqueous sodium chloride solution; bright red (dead) and uncolored (living) cells were scored by light microscope. Finally, semen smears were Papanicolaou stained and morphology was assessed.
Evaluation of Ciliary Structure and Function
Ciliated samples were obtained by brushing the inferior nasal turbinate with a 2-mm cytology brush (BC-15C; Keymed, Southend-on-Sea, U.K.; Fig. 1). 8 This has been found to be an ideal site for repeated sampling of ciliated epithelium. 9 Nasal brushings were placed in medium 199 (25 mM of hydroxyethyl piperazine ethane sulfonic acid, Earles salt, L-glutamine [pH 7.3]), which contained antibiotic solution (streptomycin at 50 mg/mL, penicillin at 50 mg/mL; GibcoBR Life Technologies, Paisley, U.K.). 10

Zeiss microscope mounted on an antivibration table (Wentworth Laboratories, Ltd., Sandy, Bedfordshire, U.K.). Specimens are examined using a ×100 interference contrast lens. Beating ciliated edges were recorded using a digital high-speed video camera (Prosilica Cam recorder; Allied Vision Technology) at a rate of 400 frames/s, using a shutter speed of 1 in 4000.
Transmission Electron Microscopy
Tissue obtained by nasal brushing was fixed in 2.5% glutaraldehyde in Sorenson's phosphate buffer for 48 hours and then postfixed in 1% osmium tetroxide. After rinsing in distilled water, the cells were embedded in a drop of 2% liquid agar at 45°C and allowed to solidify. This was processed through to resin by standard techniques. Ultrathin sections were cut at 70 nm. These were collected on 200 mesh thin-bar copper grids and stained in 1% uranyl acetate and counter-stained in Reynolds lead phosphate. The sections were then examined by transmission electron microscopy (Zeiss EM109; Carl Zeiss, Oberkochen, Germany). Ten cilia from five different cells were studied.
Ciliary Beat Frequency and Beat Pattern
Ciliated strips of epithelium were suspended in a chamber created by the separation of a coverslip and glass slide by two adjacent coverslips; its height was 0.5 mm to prevent squashing. The slide was placed on a heated stage (37°C) of a Zeiss microscope mounted on an antivibration table (Wentworth Laboratories, Ltd., Sandy, Bedfordshire, U.K.). Specimens were examined using a ×100 interference contrast lens. Only undisrupted ciliated strips of >50 nm in length were studied. Beating ciliated edges were recorded using a digital high-speed video camera (Prosilica Cam recorder; Allied Vision Technology, Stadtroda, Germany) at a rate of 400 frames/s, using a shutter speed of 1 in 4000. 10 Briefly, the camera allowed video sequences to be replayed at reduced frame rates or frame by frame. This allows the precise movement of individual cilia to be observed during their beat cycle. Ten readings of ciliary beat frequency (CBF) were taken from different areas along each ciliated edge (Fig. 1).
Results
Semen Analysis
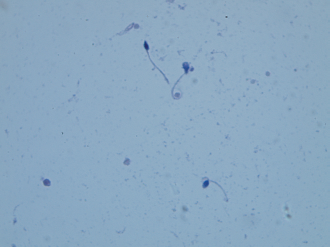
The analysis of the semen samples showed normal semen volume, pH, and high sperm concentration (135 10 6 sperm/mL; 8,775 10 6 sperm/ejaculate). A total absence of motility was observed. The supravital dye test revealed that 60% of the immotile sperm were viable (lower reference limit, 58% 4 ). No particular sperm defects were identified in Papanicolaou stained smears, and 13% of them were classified as normal (Fig. 2). Figure 3 shows the morphological sperm feature of the other PCD patients referred to previously, lacking both dynein arms; note the complete abnormally of the tails. No epididymal cysts were detected in the clinical examination of this patient.

Papanicolaou semen stained smear (1000× magnification) of the described patient.
Papanicolaou semen stained smear (1000× magnification) of the patient referred to lacking both dynein arms. Note that no normal sperm tails are present; they are coiled, shortened, or bad inserted.
Nasal Ciliary Study
A noninvasive nasal biopsy to retrieve ciliated epithelium lining the inferior surface of the inferior nasal turbinates was performed and CBF was determined. Beat pattern was slightly curved and rigid, not wide and metacronic in all of the observed fields analyzed. CBF was 8.2 Hz in average (reference value, 10–15 Hz). 11 Neither particles nor periciliary liquid mobilization was detected.
Ultrastructural assay revealed absence of the inner dynein arm in 97% of the cilia observed (Figs. 4 and 5).

Transmission electron micrograph of cross-section of cilia from nasal ciliary epithelium shows normal ultrastructure (90,000× magnification).

Transmission electron micrograph of cross-section of cilia from nasal ciliary epithelium shows absence of inner dynein arms (90,000× magnification).
Discussion
The patient arrived to our Andrology Laboratory misdiagnosed, in search of fertility after 6 years of failure. No history of genitourinary infections or previous testicular injury was given by the patient. Although sperm were all immotile, necrozoospermia was ruled out. Sperm count and morphology were normal, indicating that this man was a good candidate for intracytoplasmic sperm injection.
Although he was nonsmoker he suffered from respiratory disorders since childhood. The presence of bronchiectasis did not fit with the diagnosis of AAT-D, a disorder that causes pulmonary emphysema. 12 Sperm immotility guided the study to ciliary pathology. The final diagnosis was achieved by recording ciliary beat pattern, frequency, and ultrastructure, which revealed PCD, lacking inner dynein arms.
AAT-D and male infertility has been reported in an asthmatic patient. 13 It has been proved that AAT-D could favor the deterioration of spermatozoids. 14 The mechanisms involved could be associated with an increase in inflammatory activity, because it is known that there is a decrease in fertility in men with inflammatory diseases. 15 In our patient, probably the epididymal cysts observed in both caputs may be related to the AAT-D. Sperm are produced in the testis but mature in the epididymis, where they stay for at least 15 days; in this organ they acquire lineal motility and suffer some biochemical changes known as “decapacitation,” a phenomenon that enables them for their long trip to the ovum. The observed cysts may interfere with this procedure. In the literature there are old reports describing AAT-D in women in relation to both increase ovulation rate and enhancement of multiple pregnancies.16–18
Although PCD in clinical andrology has been extensively described, to our knowledge, this is the first time that the coexistence of AAT-D and PCD is reported in an infertile man.
Rare lung diseases, defined as a disease that affects <200,000 individuals, impact individuals across a wide swath of society, 19 like AAT-D (1/3500) 20 and PCD (1/34,000). 21
Investigations into the first disease showed that mutations in the gene for AAT protein were responsible for the destructive lung disease. This led to the discovery that AAT is a protein that inhibits elastases, enzymes that attack structural components of the lung, and launched an entire field of investigation into the role of these enzymes in the development of emphysema, even in patients who do not have genetic deficiency of AAT, and offer hope for future therapies to harness the destructive process.
PCD is an inherited disease affecting the organ system that rely on a ciliary defect caused by diverse alterations in axonemal structure and/or function. If the diagnosis is made at birth, individuals may benefit from a good life quality while a preventive medicine is installed based on physiotherapy, physical exercises, and treatment of incipient infections. Because of the genetics risks in the offspring, adequate medical counseling may be offered to the patient. Only homozygous children will suffer from the disease, because the heterozygous ones are completely healthy, because both diseases are autosomal and recessive.
Our aim was to describe a rare case of male infertility. The results from our study have direct impact in our patient but may contribute to clarify male infertility cases of unknown origin like it occurred with emphysema and AAT. Sperm motility is a subject of interest in andrology, although it has been thoroughly studied many aspects of the relationship between chemistry and mechanics in CBF remain obscure. Probably, the main tool referred in this article to evaluate nasal ciliary functionality may help us in this challenge.
In summary, the present article reports a rare case of sperm immotility associated with two autosomal recessive diseases implying respiratory disorders. This association may have been casual or could indicate that the gene or genes responsible can be linked as one female infertility case having AAT-D and PCD (defect in the outer dynein arm) was diagnosed in our clinic. Epidemiological and molecular biology studies should be conducted to confirm this hypothesis. An accurate diagnosis achieved by the study of nasal CBF and ultrastructure contributed to the patient's health management and genetic counseling while deciding fatherhood. Beyond this particular case, the present report may open a new field of studies in male infertility, mainly in cases of severe asthenozoospermia.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article