
Abstract
The lung remains one of the most challenging organs to image using magnetic resonance imaging (MRI) due to intrinsic rapid signal decay. However, unlike conventional modalities such as computed tomography, MRI does not involve radiation and can provide functional and morphologic information on a regional basis. Here we demonstrate proof of concept for a new MRI approach to achieve substantial gains in a signal to noise ratio (SNR) in the lung parenchyma: contrast-enhanced ultrashort echo time (UTE) imaging following intravenous injection of a high-relaxivity blood-pool manganese porphyrin T1 contrast agent. The new contrast agent increased relative enhancement of the lung parenchyma by over 10-fold compared to gadolinium diethylene triamine pentaacetic acid (Gd-DTPA), and the use of UTE boosted the SNR by a factor of 4 over conventional T1-weighted gradient echo acquisitions. The new agent also maintains steady enhancement over at least 60 minutes, thus providing a long time window for obtaining high-resolution, high-quality images and the ability to measure a number of physiologic parameters.
LUNG DISEASES remain a devastating cause of morbidity and mortality worldwide, with no cure for many conditions, including emphysema and cystic fibrosis, and increasing prevalence of asthma and chronic obstructive pulmonary diseases. Managing lung diseases is challenging, due in part to the limitations of current diagnostic methods based on spirometry, high-resolution computed tomography (CT), and nuclear medicine. Spirometry measures global lung function and is insensitive to mild or regional changes occurring at the onset of disease. 1 CT provides only structural information and is associated with radiation exposure.2,3 Nuclear medicine measures function (ventilation, perfusion), but spatial resolution is coarse, and this technique cannot be frequently used as it involves radioactive tracers. 4 What is desired is a noninvasive method that can provide both structural and functional information at high resolution and on a regional basis.
Magnetic resonance imaging (MRI) has the potential to overcome these limitations of conventional methods for the assessment of pulmonary structure and function. Compared to other organs, however, MRI of the lung is especially difficult. Lung signal is generally very weak as a result of low tissue density and multiple air-tissue interfaces that give rise to susceptibility effects, and fast imaging techniques are required to compensate for respiratory and cardiac motion. 5 To overcome low signal in the parenchyma, contrast-enhanced imaging with the administration of gadolinium (Gd) chelates is commonly employed to assess perfusion and ventilation. Perfusion defects, abnormalities in the pulmonary vasculature, and the presence of nodules may be assessed, 5 and ventilation deficits are indirectly identified by hypoxic vasoconstriction. 6 More experimental approaches have also been proposed, such as hyperpolarized noble gases helium 3 7 and xenon 129, 8 to assess ventilation, but complexity, high costs, and access to laser-induced hyperpolarization at the imaging site have precluded broader clinical application. To date, contrast-enhanced imaging remains the most established method and an integral component of a lung MRI examination. 6 Nonetheless, considerably greater enhancement of the parenchyma remains an important goal and will truly differentiate MRI from other imaging modalities as a sensitive, high–spatial resolution technology for both morphologic and functional lung imaging.
Ultrashort echo time (UTE) imaging was first proposed to achieve a higher signal to noise ratio (SNR) in lung MRI by Bergin and colleagues, where a very short echo time (TE) (in microseconds) was used to further minimize signal decay caused by short T2* in the lung parenchyma relative to conventional acquisitions with an already short TE (1–2 ms). 9 More recently, there has been renewed interest in applying UTE to lung MRI, and a number of noncontrast studies clearly demonstrate improved SNR and visualization of otherwise unobservable structures.10,11 When contrast is administered, UTE continues to provide gains in signal.12,13 Nonetheless, it is clear that despite the improvements demonstrated in these studies, additional and substantial gains in lung parenchymal contrast are needed. For this, one must look beyond the acquisition sequence.
The contrast agent itself wields a significant influence on the enhancement that can be achieved. Thus, an alternative method to improve parenchymal enhancement is to administer a contrast agent with a higher relaxivity and/or longer retention. A higher relaxivity translates to greater signal enhancement, whereas longer retention enables a longer window for imaging, thus eliminating the stringent requirement of timing the acquisition precisely to capture the peak enhancement of the lung parenchyma. Recently, we described the synthesis of a new high-relaxivity T1 MRI contrast agent that behaves like a blood-pool agent.14-16 The compound is a large dimeric manganese porphyrin (MnP2) (4,4′-Bis(manganese (III) 5,10,15-tris(4-sulfonatophenyl)porphin-20-yl)biphenyl). Relaxivities are r1 = 14.1 mM−1 s−1 and r2 = 18.0 mM−1 s−1 at 3 T, which are roughly three times larger than that of gadolinium diethylene triamine pentaacetic acid (Gd-DTPA), and MnP2 exerts an effect that is stable in the blood pool for at least 60 minutes. 16 The benefits of having both an anomalously high relaxivity and long retention associated with this MRI contrast agent can be further augmented through the use of UTE imaging to substantially improve lung parenchymal enhancement.
In this proof-of-concept study, we propose that the use of a high-relaxivity T1 blood-pool MRI contrast agent together with UTE imaging can substantially improve lung MRI by offering large SNR gains in the parenchyma. Furthermore, the long-circulating property of our new MnP2 compound facilitates imaging by increasing the time window over which enhancement is sustained and imaging can be performed. Lung imaging in rats on a 3 T clinical MRI scanner demonstrates the benefits of this approach over Gd-DTPA and conventional T1-weighted three-dimensional gradient echo acquisitions.
Materials and Methods
Animals
All procedures were approved by our institutional animal care committee and conducted in accordance with the national standards on animal care. Ten healthy female Long-Evans rats (Charles River, Wilmington, MA) were used in this study. Rats were induced on 2.5% isoflurane delivered through a nosepiece and maintained on 2% isoflurane for MRI. Rats were placed prone, resting on top of a water blanket maintained at 36°C (HTP-1500, Adriot Medical Systems, Loudon, TN) and placed inside the imaging coil. A 24-gauge angiocath was inserted into the lateral tail vein for contrast injection during imaging.
MRI Acquisition
Imaging was performed on a 3 T MRI scanner (Achieva 3.0T TX, Philips Medical Systems, Best, the Netherlands) using a 32-channel receive-only head coil. The protocol consisted of a standard high-resolution T1-weighted three-dimensional spoiled fast field echo (T1w-FFE) sequence with the following parameters: repetition time (TR) = 4.8 ms, TE = 1.9 ms, flip angle (FA) = 25°, number of signal averages (NSAs) = 8, 120 mm field of view (FOV), 20 slices 2 mm thick, and 0.6 × 0.6 mm in-plane resolution. The UTE sequence was a three-dimensional multiecho gradient-echo acquisition with radial readout: TR = 15 ms, TE1 = 210 μs, TE2 = 2.5 ms, NSA = 1, 120 mm FOV, 30 slices 2 mm thick, and 0.6 × 0.6 mm in-plane resolution. The UTE was repeated for FA = 10°, 30°, and 70°. Both the T1w-FFE and UTE sequences were acquired prior to injection of contrast agent and at 5, 20, and 60 minutes postinjection. Contrast was injected intravenously as a bolus (0.5–0.6 mL volume), followed by a 1.5 mL saline chaser. Acquisitions were performed on spontaneously breathing animals. No cardiac or respiratory gating was used.
For contrast administration, four different agents were compared: MnP2, manganese(III) tetraphenylporphine sulfonate (MnTPPS), manganese(III) [5,10,15,20-tetrakis(carboxy) porphyrinato] (MnTCP), and Gd-DTPA (Bayer, Toronto, ON). To evaluate the performance of MnP2, conventional Gd-DTPA was chosen as the control and two other agents were also assessed: MnTPPS, which has a lower relaxivity (r1 = 8.63 mM−1 s−1) and faster clearance than MnP2, and MnTCP, which is essentially a Gd-DTPA analogue but with a slightly higher relaxivity (r1 = 7.90 mM−1 s−1).15,16 All contrast agents were administered at a dose of 0.05 mmol/kg (per paramagnetic metal ion), with the exception of MnP2, which was also tested at roughly one-third the dose (0.015 mmol/kg). Rats were randomly assigned to different contrast agents: 5 rats for MnP2, 2 for MnTPPS, 7 for MnTCP, and 10 for Gd-DTPA. When the same animal was used repeatedly to evaluate different contrast agents, at least 3 days elapsed between injections.
Data and Statistical Analysis
MRI data were transferred to an independent workstation for data analysis using Matlab version 8.1 (MathWorks, Natick, MA). UTE images acquired at both an ultrashort TE (TE1) and a longer TE (TE2) were compared to their subtraction image (subUTE = UTE(TE1) — UTE(TE2)) and to conventional T1w-FFE. The coronal slice that yielded the maximum area of parenchymal tissue was chosen for analysis, and a region of interest was then drawn to encompass the entire lung. The SNR was computed as the mean signal in the lung divided by the standard deviation (SD) of background signal in air. Relative enhancement was calculated as the difference between the post- and preinjection signal, normalized by the preinjection signal.
All calculated values were expressed as mean ± SD. Differences in the SNR among the various acquisition sequences were compared using two-way analysis of variance (ANOVA), with the main effects being the different sequences (ie, UTE(TE1), UTE(TE2), subUTE, and T1w-FFE) and the FA for UTE. A full model was used to take into account the main effects and interactions at all levels. Post hoc Tukey-Kramer testing for multiple comparisons was then performed at the 95% confidence level. Relative enhancement across different contrast agents and changes in enhancement with time postinjection were compared using ANOVA followed by post hoc Tukey-Kramer analysis. Where significance is reported, a p value of 5% was used.
Results
The combination of UTE MRI and administration of a high-relaxivity T1 contrast agent provided superior enhancement of the rat lung. Figure 1 shows UTE images acquired at TE1 and TE2, their difference image subUTE, and conventional T1w-FFE before and 5 minutes after intravenous injection of MnP2 at a dose of 0.05 mmol/kg. The lung is clearly visible on the ultrashort TE image, UTE(TE1), but parenchymal signal decays substantially by the time of the second echo, UTE(TE2), such that there is little difference from a conventional T1w-FFE. Note, however, that UTE is more robust to physiologic motion compared to T1w-FFE. To take advantage of rapid T2* decay intrinsic to the lung, a difference image subUTE can be used instead of UTE(TE1) to suppress signal from background tissue while highlighting lung parenchyma.

Ultrashort echo time (UTE) lung MRI using a high-relaxivity blood-pool contrast agent. MRI acquired in healthy rats at 3 T (A) prior to and (B) 5 minutes after intravenous injection of MnP2 (0.05 mmol/kg). The ultrashort UTE image (UTE(TE1)) provides substantial enhancement of lung parenchyma compared to either conventional T1w-FFE or UTE acquired at a longer echo (UTE(TE2)). A subtraction image (subUTE) can be used to highlight the lung while suppressing background tissue. TE1 = 210 μs; TE2 = 2.5 ms; flip angle = 30°.
Figure 2 quantifies SNR gains from a UTE acquisition approach versus conventional T1w-FFE. An FA of 30° for UTE imaging is seen to maximize SNR in lung tissue compared to either 10° or 70°, and the differences with FA are significant (p < .05). At an optimal angle of 30°, the SNR for UTE(TE1) and subUTE is significantly greater (p < .05) than that provided by T1w-FFE, by a factor of 4 and 3, respectively. However, UTE(TE2) and T1w-FFE images are not significantly different.

Optimization of a signal to noise ratio (SNR) in lung parenchyma. Comparison of SNR in the MnP2-enhanced rat lung between UTE and conventional T1w-FFE. UTE images acquired with a flip angle (FA) of 30° provide a higher SNR than at 10° or 70°. At FA = 30°, UTE(TE1) and subUTE provide a significantly higher SNR than T1w-FFE (*p < .05).
Figure 3 shows the advantage of using a contrast agent with high relaxivity and blood-pool behavior. The lung is easily visualized on both UTE(TE1) and subUTE only when MnP2 was administered. The other contrast agents, which had either much lower relaxivity or a less stable blood-pool profile, or both, did not yield visibly clear enhancement of the lung. Figure 4 compares the relative enhancement achieved on a UTE(TE1) sequence with the different contrast agents. Enhancement was greatest for MnP2 and significantly higher compared to other agents (p < .05). Likewise, MnTPPS yielded greater enhancement than MnTCP or Gd-DTPA (p < .05), with no difference observed between the latter two. Note that these comparisons are based on a dose of 0.05 mmol/kg. Administration of MnP2 at 0.015 mmol/kg produced enhancement similar to that of Gd-DTPA at 0.05 mmol/kg.
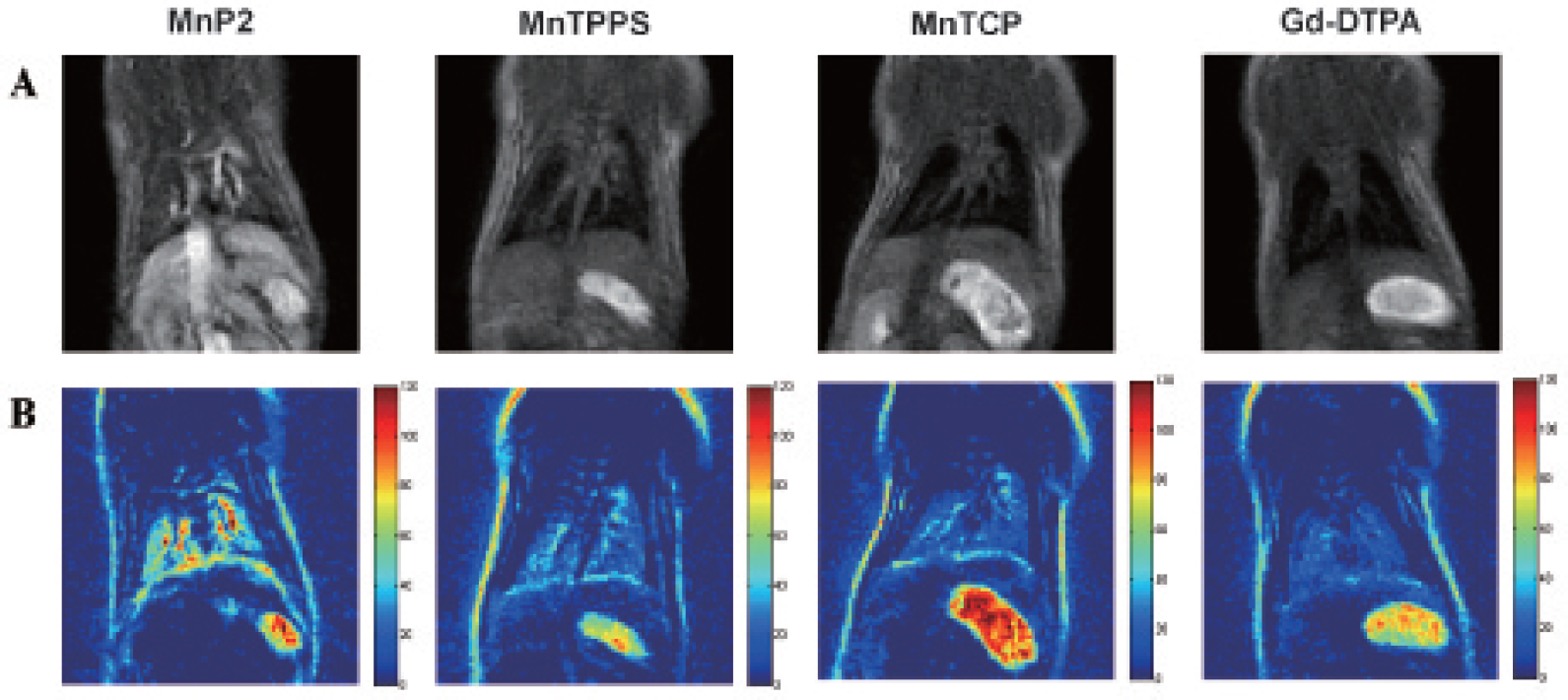
MnP2 provides greater enhancement of lung parenchyma than Gd-DTPA and other lower-relaxivity contrast agents. UTE(TE1) images (A) and subUTE images (B) acquired at a flip angle of 30° in healthy rats 5 minutes after intravenous injection of various contrast agents at 0.05 mmol/kg.

Relative enhancement of lung parenchyma across different contrast agents. Enhancement of lung tissue relative to preinjection signal for MnP2 and agents with decreasing relaxivity (MnTPPS, MnTCP, Gd-DTPA). Significant difference from Gd-DTPA is denoted (*p < .05).
Lung enhancement provided by MnP2 is sustained for at least 60 minutes postinjection (Figure 5). There is a slight decrease in lung parenchymal signal on UTE(TE1) images, from 62.2 ± 2.0 at 5 minutes to 55.8 ± 0.9 at 60 minutes, but the change was not significant.

Sustained enhancement of lung parenchyma with MnP2. MRI acquired (A) 5 minutes, (B) 20 minutes, and (C) 60 minutes after intravenous injection of MnP2 (0.05/mmol/kg) shows no significant decrease in signal over at least an hour. TE1 = 210 μs; TE2 = 2.5 ms; flip angle = 30°.
Discussion
Lung MRI has the potential to provide high-resolution assessment of lung structure and function on a regional basis and without exposure to ionizing radiation or radioactive tracers—all the capabilities desired in conventional methods for lung assessment. Achieving significant enhancement of the lung parenchyma, however, has been one of the greatest challenges for lung MRI. In this study, we demonstrated a new concept of combining UTE imaging and a high-relaxivity blood-pool MRI contrast agent for superior enhancement of lung parenchymal tissue. A high relaxivity allows very sensitive delineation of the lung, whereas long retention in the blood pool offers a wide time window for imaging and, therefore, the opportunity to acquire high-resolution, high-quality images related to a number of parameters and to reexamine if necessary. The use of UTE MRI further enhances the SNR, and subUTE MRI can be used to suppress background tissue by leveraging intrinsic T2* decay in the lung. The results observed in healthy rats on a 3 T scanner strongly support the potential of this new approach for sensitive, high-resolution imaging of lung structure and function.
A complete assessment involves not only lung morphology but also physiologic processes such as perfusion, ventilation, and oxygen transfer. UTE alone may be used morphologically to assess lung density. 10 However, a contrast-enhanced protocol, as described in this work, is the gold standard for obtaining information on perfusion and vascular abnormalities (eg, alterations in blood flow, blood volume, and vessel size) and can indirectly identify ventilation defects. An important point to bear in mind is that no single technique can measure all the desired properties. For example, hyperpolarized MRI provides a more direct measurement of ventilation but is not established for measuring perfusion. Likewise, our new approach is sensitive to a subset of important processes, including perfusion and ventilation. Most importantly, it provides substantial enhancement of the lung parenchyma and is easy to implement, requiring no additional specialized hardware or equipment. As such, this approach would be valuable as both a substitute for conventional lung MRI and a complement to hyperpolarized MRI.
To demonstrate the need for a high-relaxivity blood-pool contrast agent, we used our new manganese porphyrin compound MnP2 as proof of concept. Practically, there is no restriction on the type of contrast agent employed, as long as it exhibits high relaxivity (with strong T1 effects that are able to show through competing T2* effects on a UTE acquisition) and long retention to widen the window for imaging. Currently, commercially available blood-pool agents, such as Ablavar, do not provide relaxivities comparable to that of MnP2. 14 At higher field strengths such as 7 T, the relative relaxivity advantage provided by MnP2 is expected to be even greater. Furthermore, MnP2 has a very long retention in blood, showing enhancement even 24 hours postcontrast administration. 16 What remains to be determined is its toxicity, although no animal exhibited either short- or long-term side effects. MnP2 was designed from a chemistry perspective to be even safer than Gd chelates such as Gd-DTPA and Ablavar, and toxicity studies are ongoing as we work on translating this new agent from preclinical to clinical application.
The UTE acquisition presents several advantages for lung imaging. First and foremost, a very short TE enables lung parenchyma to be visible, even without contrast administration. When contrast is administered, the T1 effect of the contrast agent can show through more easily than on conventional sequences. Radial UTE acquisitions are also more robust to motion compared to conventional sequences. It was recently reported that lung images virtually free of motion artifacts could be generated in free-breathing small animals. 17 Gobbo and colleagues achieved reasonable image quality of the lung without cardiac or respiratory gating. 12 In this study, we also used free-breathing to maintain a constant TR. Acquisitions in rats revealed the presence of motion artifacts in T1w-FFE images but not in UTE images.
Although the purpose of this study was to demonstrate the concept of UTE imaging using a high-relaxivity contrast agent—specifically, to demonstrate that UTE sequences can benefit immensely from T1 contrast agents that provide an unappreciated but heavy T1 weighting—some optimization was needed to illustrate the value of this new approach. For example, we determined the FA that would maximize the SNR, and we compared enhancement from using two different doses of contrast agent. The optimal FA and dose would have to be determined more precisely, but an optimal angle of 30° as determined in this study is largely consistent with the dose and range of postcontrast T1 values achieved in various tissues, including blood and liver, as determined previously. 16 Note that we optimized the FA for MnP2 and not for the other contrast agents because enhancement was generally low for these other agents regardless of the FA. In the future, we can further augment SNR gains by further reducing the ultrashort echo TE1. Another area of investigation is how MnP2 is retained in lung tissue, whether retention in blood is the sole mechanism or if trapping in alveoli presents an additional influence. We will also incorporate animal models of lung disease to evaluate the sensitivity of the proposed approach in detecting subtle changes in lung morphology and function.
Conclusion
This study presented a new approach for highly sensitive lung MRI based on contrast-enhanced UTE imaging using a high-relaxivity blood-pool contrast agent. It was shown that the combination of UTE and this novel contrast agent provided substantial SNR gains in the lung parenchyma compared to conventional acquisitions and to Gd-DTPA. Furthermore, a steady-state was maintained for at least 60 minutes postinjection, thus providing a long time window for obtaining high-resolution, high-quality images and the ability to measure a number of physiologic parameters.
Footnotes
Acknowledgments
We thank Melanie S. Kotys-Traughber from Philips Healthcare (Cleveland, OH) for implementing the UTE sequence and Charles Mougenot from Philips Healthcare for support.
Financial disclosure of authors: This study was supported by the Heart and Stroke Foundation (#000223 awarded to H.- L.M.C.) and the Natural Sciences and Engineering Research Council of Canada (#355795 awarded to H.-L.M.C. and #489075 awarded to X.-a.Z.). A patent application has been filed for the contrast agent MnP2. Zhang XA, Cheng WR, Haedicke I, Cheng HL, Gd-free MRI contrast agents (US patent appl. #2013101159, Canadian patent appl. #2013101162).
Financial disclosure of reviewers: None reported.