
Abstract
The aim of this study was to explore the diagnostic performance of 99mTc-3(poly-(ethylene glycol),PEG)4-RGD2 (99mTc-3PRGD2) scintimammography (SMM) in patients with either palpable or nonpalpable breast lesions and compare SMM to mammography to assess the possible incremental value of SMM in breast cancer detection. We also investigated the αvβ3 expression in malignant and benign breast lesions. Ninety-four patients with 110 lesions were included in this study. Mammograms were evaluated according to the Breast Imaging Reporting and Data System (BI-RADS) by a specialized imaging radiologist. Prone SMM was performed 1 hour after injection of 99mTc-3PRGD2. Scintigraphic images were interpreted independently by two experienced nuclear medicine physicians using a three-point system, and the kappa value was calculated to determine the interreader agreement. The McNemar test was used to compare SMM and mammography with respect to sensitivity, specificity, and accuracy. Diagnostic values for breast cancer detection were evaluated for each lesion. Immunohistochemistry was performed to evaluate integrin αvβ3 expression. Histopathology revealed 46 malignant lesions and 64 benign lesions. The overall sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of SMM were 83%, 73%, 77%, 69%, and 85%, respectively. The kappa value between the two reviewers was 0.63. The diagnostic values of SMM were higher than those of mammography in evaluating overall breast lesions. A sensitivity of 91% was achieved when SMM and mammography results were combined with 60% of all false-negative mammography findings classified as true-positive results by SMM. Integrin αvβ3 expression was positively identified using SMM imaging. SMM is a promising tool to avoid unnecessary biopsies when used in addition to mammography and can be used to image αvβ3 expression in breast cancer with good image quality.
BREAST CANCER is by far the most common malignancy among women worldwide and was also the leading cause of cancer death among women age 20 to 59 years. 1 The American Cancer Society estimates that 234,580 new cases of breast cancer were diagnosed in 2013, which is expected to account for 15% of all female cancer deaths. 1
Early detection of breast cancer can significantly reduce mortality.2,3 To date, mammography is the standard detection method for breast carcinoma. However, it is not ideal for identifying the presence of malignancy because the false-negative rate can be as high as 34%, which often leads to delays in treatment and a false sense of security. 4 Furthermore, the positive predictive value (PPV) can be as low as 15% for nonpalpable tumors and 22% for palpable tumors, resulting in a large number of unnecessary biopsies. 5
In an effort to strengthen the diagnostic capacity of mammography, scintimammography (SMM) with various radiopharmaceuticals has been explored in the detection of breast cancer. 6 Among these radiopharmaceuticals, 99mTc-sestamibi (99mTc-MIBI) has been one of the most successful candidates. 7 Extensive single-center and multicenter clinical trials demonstrated that SMM using 99mTc-MIBI has high sensitivity (ranging from 69 to 93%) and high specificity (ranging from 69 to 94%) for the detection of breast cancer. 8 However, this tracer was originally dedicated for cardiac imaging and not specifically designed for tumor imaging. The exact mechanism of malignancy detection is still largely unknown, which limits evaluation for the biologic status of the tumor. Furthermore, the image quality with 99mTc-MIBI is not optimal, which may not allow a reliable interpretation. 9
Integrin αvβ3, a heterodimeric glycoprotein, is preferentially expressed on several types of cancer cells, including in melanoma, glioma, and ovarian and breast cancers.10,11 Because arginine-glycine-aspartic acid (RGD) can bind strongly to integrin αvβ3, many RGD peptide probes have been developed to image αvβ3 expression.12–15 99mTc- 3PRGD2 is a well-designed, dimeric RGD peptide that shows high tumor uptake in mouse breast cancer xenografts. 16 Previously, our group applied this novel tracer for noninvasive differentiation of solitary pulmonary nodules (SPNs). The tracer demonstrated an impressive image quality with high sensitivity in detecting malignant SPNs. 17
In this study, we performed 99mTc-3PRGD2 SMM in patients with abnormal mammograms or palpable breast abnormalities. The aim was to explore the diagnostic performance of SMM and to compare SMM to mammography to assess the possible value of SMM in breast cancer detection. At the same time, we used SMM to noninvasively image αvβ3 expression in breast cancer.
Materials and Methods
Patients
The patient population was primarily selected based on physical breast examinations and mammographic findings. To be enrolled in the study, the patient needed to have no history of other breast diseases that could affect image quality and had already been scheduled for percutaneous biopsy or surgery. Surgeries were carried out based on the clinical situation and willingness of the patient. Some patients had low Breast Imaging Reporting and Data System (BI-RADS) assessment scores, but palpable breast lesions were still present. Patients voluntarily underwent a percutaneous biopsy and an SMM test. Ninety-four patients (92 women, 2 men; 110 lesions) with abnormal mammograms, palpable breast abnormalities, or both were enrolled. Exclusion criteria included pregnancy, lactation, and a body weight greater than 80 kg.
Written informed consent was obtained from all subjects. The study and use of the new radiotracer 99mTc-3PRGD2 were approved by the local independent Ethics Committees and the Institutional Review Boards of China-Japan Union Hospital, Changchun, China.
All patients underwent percutaneous biopsy or surgery within 2 weeks of imaging. A final diagnosis was concluded by pathologists affiliated with the hospital. The largest dimension of the tumor was considered the pathologic size.
Mammography
Mammography was performed using craniocaudal and mediolateral oblique views. Mammograms were evaluated on a per-lesion basis by a specialized imaging radiologist according to the BI-RADS. The radiologist was unaware of histopathology, SMM findings, and physical examination data of patients during evaluation. Mammograms were considered positive for malignancy if the BI-RADS score was ≥ 4. When additional imaging was recommended, patients were scored as BI-RADS category 0 and excluded from the study. The parenchymal patterns “heterogeneously dense” and “extremely dense” were defined to represent dense breasts, whereas “almost entirely fat” and “numerous vague densities” were used to classify breasts as fatty.
99mTc-3PRGD2 SMM
Radiolabeling and quality control procedures for 99mTc- 3PRGD2 were performed as described previously. 17 99mTc-3PRGD2 with a mean radioactivity of 849 ± 115 MBq was administered via a single intravenous bolus injection 1 hour prior to imaging and followed by a 10 mL saline flush.
Anterior planar images and lateral images obtained in the prone position were acquired by a gamma camera (Philips Healthcare, WA) interfaced to an Imagamma system (Philips Healthcare)-based computer. The system is equipped with a low-energy, parallel-hole collimator. All images were acquired within 13 minutes of injection with a 20% energy window centered on 140 keV. During acquisition of the static lateral images, the subject was prone with the breast hanging freely. The distance between the breast and the detector was minimized.
Interpretation of SMM
All images were interpreted qualitatively by two experienced nuclear medicine radiologists. Visual analysis was performed on a per-lesion basis and in a blinded fashion. A three-point scale system was adopted to describe the degree of uptake by breast lesions. The rules for classification were as follows: grade 1, no abnormal increased uptake; grade 2, mildly increased uptake; grade 3, definite focal increased uptake. Homogeneous uptake in both breasts was classified as grade 1. SMM was considered positive for malignancy if the visual score was ≥ 2. Disagreements between reviewers were resolved by consensus with a third experienced reviewer as a referee.
Immunohistochemistry of αvβ3 Expression
The immunohistochemistry of αvβ3 expression of the breast tissue sample was performed as described previously. 17 The abnormal tissues were snap-frozen, sectioned (3 μm), and immersed into 10% neutral buffered formalin for fixation for 24 hours at 4°C. For immunohistochemical investigation, the specimens were stained using the biotinylated monoclonal anti-αvβ3 antibody LM609 (1:100; Chemicon Europe, EMD Millipore Corporation, Billerica, MA) and detected after peroxidase staining with 3-amino-9-ethylcarbazole (AEC; Vector Laboratories, Burlingame, CA) as the substrate. Analysis of staining was performed by a senior pathologist, who was unaware of the results of the SMM data.
Statistical Analysis
Data are expressed as mean ± SD. The kappa statistical test was used to determine interreader agreement for visual analysis of planar scans. The McNemar test was used to compare planar visual analysis and mammography with respect to sensitivity, specificity, and accuracy, whereas the Fisher exact test was used to compare the PPV and negative predictive value (NPV) of the two methods. Diagnostic values for breast cancer detection were calculated on a per-lesion basis. For all statistical analyses, a p value < .05 was considered statistically significant.
Results
Patient Information
The mean age of the subjects was 53.6 ± 10.2 years (range 23–74 years). Of the patient population, 21.3% (20 of 94) were premenopausal and 17.0% (16 of 94) had dense breasts. A total of 110 lesions were identified. Among them, 79.1% (87 of 110) were palpable and 20.9% (23 of 110) were nonpalpable. The prevalence of malignancy was 41.8% for all lesions. According to the BI-RADS classification, 22 mammograms were classified as category 1, 14 as category 2, 13 as category 3, 33 as category 4, and 28 as category 5.
Scintimammography
The results of SMM, palpability, histologic diagnosis, and size of the lesions are summarized in Table 1. There were 38 true-positive findings, and the most frequent malignancy in this group was invasive ductal carcinoma (IDC). Twenty-eight of the 38 true-positive lesions (73.7%) were palpable. The average histologic size among the true-positive tumors was 2.9 ± 1.6 cm (range 1.0–8.5 cm) in the greatest dimension. The smallest detectable malignant lesion with SMM was 1.0 cm in diameter.
SMM Results, Histology, Palpability, and Size of Breast Lesions
NPAL= nonpalpable lesion; PAL= palpable lesion; SMM = scintimammography.
No size was given.
Eight cases were identified as false negative, including five IDC and three ductal carcinomas in situ (DCIS). Four of these cases were nonpalpable. Three cases of DCIS were smaller than 1 cm in histologic size. The average histologic size of the 5 cases of false-negative IDC was 2.1 ± 0.5 cm (range 1.5–2.7 cm) in the greatest dimension.
Of the 47 true-negative results, 26 lesions were identified as adenosis based on histopathology. The remaining lesions were 18 fibroadenomas, 2 cysts, and 1 lipoma. Seven of these cases were nonpalpable. There were 17 false-positive findings, made up of 6 fibroadenomas, 8 cases of adenosis, 2 abscesses, and 1 cyst. Fifteen of these cases were palpable.
For tumors smaller than 1 cm in the greatest dimension, the sensitivity of SMM was 0% (95% CI 0–56). The sensitivity of SMM was 86% (95% CI 49-97) for tumors between 1 and 1.5 cm and 91% (95% CI 78–97) for tumors larger than 1.5 cm. The weighted kappa value for the blinded SMM visual interpretation between the two reviewers was calculated as 0.63, indicating substantial interobserver agreement.
Diagnostic Performance of SMM and Mammography
As shown in Table 2, the sensitivity, specificity, and accuracy calculated for the overall lesions did not differ significantly between SMM and mammography (p > .05, analyzed by McNemar test). PPV and NPV between the two methods also did not differ significantly (p > .05, analyzed by Fisher exact test).
Comparison of Diagnostic Performance between SMM and Mammography

NPAL= nonpalpable lesion; PAL= palpable lesion; SMM = scintimammography.
Six malignant lesions (all palpable) that had been classified as false negative by mammography were categorized as true positive by SMM. Therefore, 13% (6 of 46) of malignant lesions were only detected by SMM. For 60% (6 of 10) of all false-negative mammograms, SMM correctly identified malignancy, leading to a sensitivity of 91% (95% CI 80–97) when the results of SMM and mammography were combined.
Immunohistochemistry of αvβ3 Expression
Of the 94 patients (110 lesions) who completed the study, only 49 patients (32 malignant lesions, 17 benign lesions) had samples available for immunohistologic staining. Twenty-seven lesions of the 32 malignant samples with a visual score ≥ 2 in SMM were confirmed to be positive for integrin αvβ3 expression. Of the 17 benign samples, 4 lesions with a visual score ≥ 2 were confirmed to have positive integrin αvβ3 expression. Expression of the integrin αvβ3 was identified predominantly on the endothelium of newly formed blood vessels (Figure 1). All 18 lesions, either malignant or benign, with a visual score of 1 in SMM, were found to barely express integrin αβ (Figure 2).

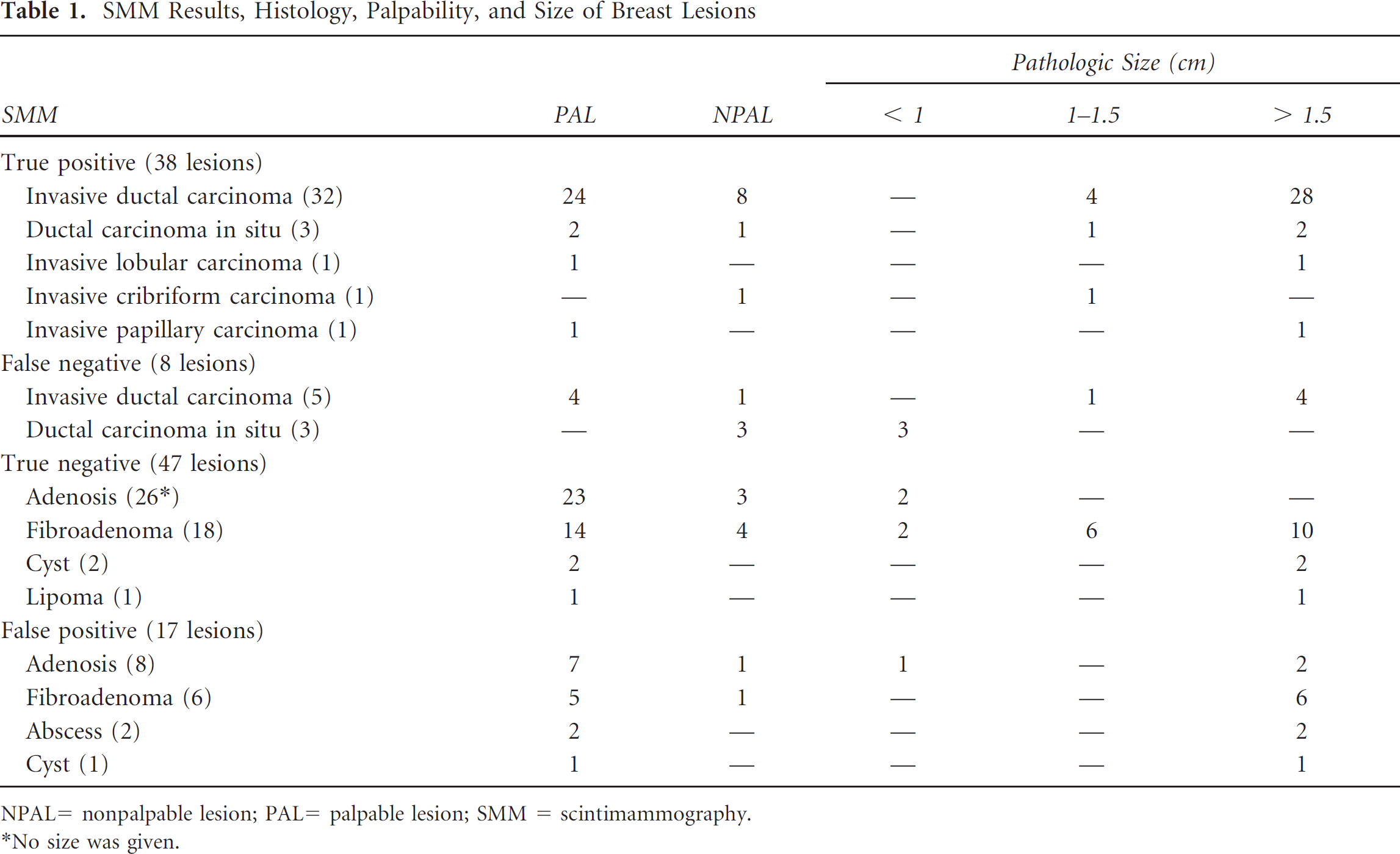
Example of a true-positive SMM result. A, A lesion in the left breast was identified by mammography, BI-RADS category 5. B and C, High uptake of the radiotracer was observed in the lesion. D, Histopathology staining indicates ductal carcinoma in situ. E, Immunohistochemistry demonstrates intense αvβ3 expression in tumor vessels. Scale bar: 100 μm. Scale bar: 100 mm. Arrows indicate the tumor location in each experiment.
Example of a true-negative SMM result. A, A lesion in the right breast was identified on mammography, BI-RADS category 2. B and C, No tracer uptake was observed in the lesion. D, Histopathology staining indicates adenosis. E, Immunohistochemistry demonstrates scarce αvβ3 expression in the tissue sample. Scale bar: 100 μm. Arrows indicate the tumor location in each experiment.
Discussion
Nuclear medicine techniques with targeted tracers are just emerging with the advent of the molecular imaging era, although they have been applied for the detection of malignancy for several decades. 99mTc-3PRGD2 exhibited a rapid clearance from the blood, largely by the kidneys. The effective radiation dose was calculated as we previously reported. 17 We found that the effective radiation dose is significantly lower than the limit set by International Commission on Radiological Protection (ICRP) Publication 60, 18 showing an acceptable radiation burden. The high sensitivity of 99mTc-3PRGD2, an angiogenesis-targeted tracer, which demonstrated effectiveness in evaluating SPNs, prompted us to test its diagnostic performance in breast cancer. To the best of our knowledge, this is the first application of 99mTc-3PRGD2 in breast cancer.
In the present study, we compared the performance of 99mTc-3PRGD2 SMM and mammography in evaluating breast lesions. The results showed that although the values for 99mTc-3PRGD2 SMM were higher, the diagnostic performance between them was not significantly different (99mTc-3PRGD2 SMM vs mammography: for sensitivity, p = .8; for specificity, p = .2; for accuracy, p = .4 calculated by McNemar test; for PPV, p = .3; for NPV, p = .6 calculated by Fisher exact test). Yet 13% of malignant lesions were only detected by 99mTc-3PRGD2 SMM. The combination of the two techniques can increase sensitivity to 91%. Taking into account the simplicity and good interobserver agreement of the 99mTc-3PRGD2 SMM procedure, we believe that this new approach may have the potential to increase the sensitivity of mammography in clinical practice.
According to an evidence-based analysis performed on 47 studies between 1994 and 1999, the NPV of SMM with 99mTc-MIBI for breast cancer averaged 76%. 19 By using 99mTc-3PRGD2 SMM, we achieved a value of 84%. The result suggests the potential and important role that 99mTc-3PRGD2 SMM holds in ruling out malignancy and thus avoiding unnecessary biopsies for breast lesions.
The overall sensitivity of 99mTc-3PRGD2 SMM was not as high as expected in this study. We speculate that the false-negative results were caused by the size and locations of these lesions. We observed eight false-negative cases in total. Of these cases, four lesions were palpable and four were nonpalpable. The three cases of DCIS had lesions smaller than 1 cm (two at 0.8 cm, one at 0.2 cm). For the five cases of IDC, the mean size of the lesions was 1.95 ± 0.48 cm, and most of the lesions were located in the medial part of the breast, which is further away from the detector.
For lesions with a size between 1.0 and 1.5 cm (n = 7), 99mTc-3PRGD2 SMM achieved a sensitivity of 86% (95% CI 49-97), which is comparable to that for SMM with 99mTc-MIBI.20,21 Hypothetically, a tracer with enough binding affinity such as 99mTc-3PRGD2 may detect most tumors with a diameter above 1 cm because tumor diameters rarely exceed 0.2 to 0.3 cm without angiogenesis. 22 However, the seemingly satisfactory result must be validated in a larger patient population. For tumors larger than 1.5 cm (n = 35), a sensitivity of 91% (95% CI 78–97) was achieved, which is comparable to that reported for SMM with 99mTc-MIBI.20,21
For palpable and nonpalpable lesions, 99mTc-3PRGD2 SMM demonstrated sensitivity of 88% (95% CI 72–95) and 71% (95% CI 45–88), respectively. The trend is consistent with the results from SMM with 99mTc-MIBI that demonstrated a superior sensitivity for palpable over nonpalpable breast lesions.8,23 However, 99mTc-3PRGD2 SMM achieved a sensitivity of 71% for nonpalpable lesions, which is comparable to a pooled sensitivity of 59% for SMM with 99mTc-MIBI. 23 The result may be explained by a different a mechanism. Given that the nonpalpable patient population in this study is small, further verification is still needed.
SMM with 99mTc-MIBI always showed a low sensitivity for DCIS.20,21 Consistently, in our study, 99mTc-3PRGD2 SMM yielded a sensitivity of 50% (95% CI 19–81) for DCIS (n = 6). In patients with nonpalpable DCIS (n = 4), the sensitivity of 99mTc-3PRGD2 SMM was only 25% (95% CI 5-70). 99mTc-3PRGD2 SMM performance did not improve in this subgroup compared to SMM with 99mTc-MIBI, possibly indicating that a size limitation exists for 99mTc-3PRGD2 SMM in the detection of DCIS. 7
Among 17 false-positive cases with 99mTc-3PRGD2 SMM, histopathology identified 5 fibroadenomas, 7 cases of adenosis, 2 abscesses, and 1 cyst. The high uptake of 99mTc-3PRGD2 in these lesions could be explained by the extensive involvement of angiogenesis during such pathologic events. 24 Thus, necessary caution should be paid for the interpretation of 99mTc-3PRGD2 SMM when it is used independently to differentiate breast lesions. Overall, 99mTc-3PRGD2 SMM yielded a specificity of 73% (95% CI 62-83), which is comparable to the mammography results in this study. The dense breast rate in the patient population was relatively low. Consequently, compared to a normal patient population, fewer cancers were obscured by dense tissue of the breast. This may explain the high NPV (80%) for mammography in this study.
There are several limitations to this study that call for further discussion. First, we only recruited patients with abnormal mammograms or palpable breast abnormalities that were not detected by mammography. Therefore, high-risk patients predominated in the analyzed population. Although we did our best to ensure an independent, unbiased reading of the 99mTc-3PRGD2 SMM results, it is conceivable that readers could have been biased by the fact that the vast majority of scans were from patients with a high risk of breast disease. Second, given that there is currently no available αvβ3 antibody that works on paraffin-embedded specimens, we had to use snap-frozen specimens for immunohistochemistry. This reduced the number of specimens with workable quality. Therefore, quantification and correlation of integrin αvβ3 expression with tracer uptake were not performed in this study. However, the data acquired so far support the assumption that differentiated uptake of 99mTc-3PRGD2 in malignant and benign lesions was due to different levels of αvβ3 expression.
Conclusion
99mTc-3PRGD2 SMM shows promise as an additional tool to mammography to avoid unnecessary biopsies. At the same time, 99mTc-3PRGD2 SMM can provide good image quality of αvβ3 expression in breast cancer. This technique may also allow response monitoring to breast cancer therapy through longitudinal imaging.
Footnotes
Acknowledgment
This research was supported by the National Natural Science Foundation of China (NSFC) projects (Grant number: 81271606), Research Fund of Science and Technology Department of Jilin Province (Grant number: 201015185 and 201201041).
Financial disclosure of the reviewers: None reported.