
Abstract
The effectiveness of microbubble-mediated ultrasound molecular imaging and drug delivery has been significantly affected by the axial laminar flow of vessels which prevents ultrasound contrast agents (UCAs) from targeting vascular endothelium. Studies show that acoustic manipulation could increase targeted UCA adhesion in microcirculation and some small vessels. In this study we demonstrate that ultrasound radiation force (USRF) can also significantly enhance the targeted adhesion of microbubbles in both small and great vessels. Our results indicate that the UCA adhesion targeted to ICAM-1 expressed on mouse cremaster microvascular endothelial cells increase about 9-fold when USRF is applied at 1 MHz and 73.9 kPa. The adhesion of anti-CD34 microbubbles to the endothelia of rat abdominal aorta was visually analyzed using scanning electron microscopy for the first time and thousands of microbubbles were found attached to the aortic endothelia after USRF application at the same acoustic parameters. Our data illustrate that targeted adhesion of anti-CD34 microbubbles is possible in normal abdominal aorta and we demonstrate the potential of using USRF in molecular imaging of a vascular target.
MICROBUBBLE ULTRASOUND CONTRAST AGENTS (UCAS) have been widely used in ultrasound imaging to enhance the blood perfusion of tissues. 1 They are small enough to travel through circulation to provide echogenic bodies for ultrasound scattering. Contrast-specific targeted ultrasound imaging, first demonstrated in human plasma clots by Lanza and colleagues, 2 has received a lot of attention. Studies have shown that microbubbles have the potential to be used as targeted UCAs or as drug delivery vehicles.3,4 Many specific molecular ligands, such as antibodies, peptides, asialoglycoproteins, and polysaccharides, could be conjugated to the outer surface of the microbubbles for highly specific adhesion to targets. 5 Molecular imaging and molecular targeted therapy are of significant clinical relevance in many aspects, including imaging of specific molecular targets, pathways, cellular processes, and even regional drug or gene delivery.6,7 So far, specific targeted ultrasound contrast imaging has demonstrated the ability to assess intravascular thrombus,2,8,9 tumor angiogenesis,10,11 and postischemic injury 12 using specific targeted UCAs.
Limitations in Specific Microbubble Targeting
However, targeted imaging is far from clinically acceptable because it is difficult to obtain consistent, significant visual contrast harmonic imaging except in the intravascular thrombus.8,12 For most targeted imaging, ultrasound imaging is unable to obtain strong and vivid contrast images from the burst of adhesive targeted bubbles that could last only a few seconds.6,8,13 The reason for this is perhaps mainly due to relatively insufficient targeted microbubbles that can be bound to the corresponding receptors on the vascular endothelium. Microbubbles tend to move in the central axial flow with erythrocytes in laminar flow,14–17 hardly getting an opportunity to contact the targeted receptor on the vascular wall.
Ultrasound Radiation Force
Ultrasound radiation force (USRF) is one of the mechanical effects of ultrasound propagation in media. Usually, USRF consists of two components: the primary force, which pushes microbubbles away from acoustic source, and the secondary force, which tends to aggregate or repulse microbubbles. Studies in a microvascular fluid chamber model demonstrated that USRF generated by low-amplitude ultrasound (120–900 kPa) pushed the targeted microbubbles away from the central flow to the wall of a 200 mm cellulose vessel in vitro. 18 It has been reported in several articles that USRF is able to move microbubbles away from the central stream toward the endothelium at low-peak negative pressure in vivo and promote microbubble targeting adhesion in vivo using a mouse cremaster muscle inflammation model.18,19 Acoustic radiation force has also been suggested as a mechanism to enhance the delivery of therapeutic substances.20,21 Nevertheless, the number of accumulated microbubbles (either the anti-P-selectin or the anti-αvβ3 integrin targeted microbubbles) on the endothelia was still limited, even with the help of USRF. Only an approximately 4-fold increase in the femoral vein and a 20-fold increase in the femoral artery have been reported. 19 The retention of UCA targeted to P-selectin can reach an 80-fold increase in vitro. 22 Under this condition, it might be difficult to produce strong contrast ultrasound imaging in vivo.
In this study, we attempted to promote the adhesion of targeted microbubbles to the endothelial surface in great number using USRF in vivo. The retention of anti-intercellular adhesion molecule 1 (anti-ICAM-1) microbubbles and anti-CD34 microbubbles was examined in two animal models: inflammation in cremaster microcirculation in mice and the normal abdominal aorta of rats.
Materials and Methods
Contrast Agent Preparation
Lipid-coated microbubbles called Zhifuxian were used in this study. Zhifuxian is a stable microbubble for ultrasound contrast imaging developed in our laboratory by encapsulating perfluoropropane in a lipid shell. The main preparation procedure is as follows. Certain quantities of 1,2-dipalmitoyl-sn-glycero-3-phosphatidylglycero (DPPG), 1,2-distearoyl-sn-glycero-3 phosphocholine (DSPC) (Genzyme Pharmaceuticals LLC, Liestal, Switzerland), and polyethylene glycol 4000 (PEG-4000) were well hydrated with ultrapure water in a 60°C thermostatic water bath. The resulting suspension was divided into 2 mL vials (1 mL/vial) and underwent a 24-hour freeze-and-dry process. The dried powder of the lyophilization was dispersed by 1 mL mixed liquor of 50% glucose, propylene glycol, and glycerine with a volume ratio of 8:1:1. After the air in the vial was substituted with perfluoropropane, the vial was shaken with a high-speed mechanical amalgamator at a frequency of 4,500 rotations per minute for 45 seconds.
The microbubble size distribution and concentration were determined by a RC-3000 Coulter counter (OMEC Technology Co., Ltd. Zhuhai, China), and the microbubbles had a mean particle diameter of 0.8 μm, with 98% of the particles less than 8 μm and a microbubble concentration of 6 to 9 × 109/mL. Two types of targeted contrast agents were used in this study. In the cremaster microvasculature inflammation experiment, we used fluorescein isothiocyanate (FITC)-labeled anti-ICAM-1 monoclonal antibody (Beijing Biosynthesis Biotechnology Co., Beijing, China) as the targeting ligand and the anti-CD34 monoclonal antibody (Beijing Biosynthesis Biotechnology Co., Beijing, China) was employed in the experiment targeting aortic endothelial adhesion. Both of the targeted contrast agents were prepared by means of biotin-streptavidin chemistry, as in Lindner and colleagues' study. 12 The size distribution and concentration of microbubble dispersions were characterized using a Mastersizer 2000 (Malvern Instruments Ltd, Worcestershire, UK). A fluorescence microscope (DM IRB, Leica Microsystems, Wetzlar, Germany) was used to observe the fluorescent targeted microbubbles, and a flow cytometer (Epics XL, Beckman Coulter Inc., Brea, CA) was employed for calculating the binding ratio of the microbubble of anti-ICAM-1 antibody. The anti-CD34 microbubble was not originally FITC labeled, so we conjugated it with a corresponding antibody (IgG-FITC) only when we performed flow cytometry (FACSCalibur, BD Biosciences Co., Franklin Lakes, NJ) for calculating the binding ratio.
Ultrasound for Acoustic Treatment
The ultrasound for acoustic treatment was generated by an air-backed, spherically 25 mm diameter disk, nonfocused, planar transducer. The front surface area of the transducer was 6.25 cm2. The transducer was driven by a wave generator and a power amplifier specially designed for it. The transducer was operated with a central frequency of 1.1 MHz, a pulse repetition frequency of 10 kHz, and a duty cycle of 90%. Acoustic pressure calibrations were performed using a needle hydrophone (TNU001A, NTR Systems Inc., Seattle, WA) and a preamplifier (A17 dB, Specialty Engineering Associates, Sunnyvale, CA) connected to a digital oscilloscope (9350, LeCroy Corporation, Chesnut Ridge, NY) for the transducer's acoustic output. The measurement was taken at the central axis of the transducer and 1 mm away from the surface using the needle hydrophone. The results showed that the acoustic pressures can be switched between 54.2 and 73.9 kPa, corresponding to the acoustic intensities (spacial-peak-temporal-average intensity [ISPTA]) of 0.12 and 0.22 W/cm2, respectively.
Animals and Treatment Protocol
Fifteen male Chinese Kunming (KM) mice, weighing about 20 g, were used to examine UCA retention in mouse cremaster muscle microcirculation. Nine Sprague-Dawley (SD) rats, 4 weeks of age and weighing from 100 to 120 g, were used to examine UCA retention in the rat abdominal aorta. All procedures were performed in accordance with the approval of the Institutional Review Board of Xinqiao Hospital. Anesthesia of all animals was induced by intraperitoneal injection of 420 mg/kg body weight chloral hydrate in a 7% saline solution (Kelong Chemical Engineering, Chengdu, China). Body temperature was maintained by air conditioning. Construction of the cremaster muscle inflammation model was performed by scrotal injection of 500 ng tumor necrosis factor α (Pepro Tech Inc. London, UK). After surgical preparation of the cremaster muscle of a male KM mouse, the cremaster muscle was fixed to the stage and coupled with coupling gel for the ultrasound treatment. The ultrasound transducer was fixed and contacted to the cremaster with a 1 mm thick coupling gel. The gel underneath the cremaster tissue was about 1 cm. For absorption of the ultrasound reflection, we put a foam rubber plate on the operation table under the gel. The foam rubber was about 2 to 3 cm thick.
In the rat study, the abdominal aorta was surgically exposed about 2.5 cm segments above the bifurcation of the left and right common iliac artery using longitudinal incision. The transducer was also perpendicularly fixed 3 mm above the anterior wall of the aorta and they were coupled with gel. All of the targeted and nontargeted microbubbles were administered to the caudal vein through a 5-scalp needle.
Acoustic Treatment
Both rats and mice were divided into three groups: the low USRF plus microbubble group (54.2 kPa + UCA), the high USRF plus microbubble group (73.9 kPa + UCA), and the control group (0 kPa + UCA). In the aorta study, there were three rats in every group, and in the cremaster study, there were five mice in every group. In the two US + UCA groups, ultrasound insonation and intravenous microbubble injection were both applied, and 54.2 kPa acoustic pressure was applied in the low USRF group and 73.9 kPa in the high USRF group. UCA administration was performed only in the control group. In the rat study, a bolus of 106 UCA was injected into the caudal vein. In the mouse study, a bolus of 106 UCA was injected into the caudal vein. Immediately after intravenous UCA injection, the cremaster or the abdominal aorta was insonated for 5 minutes and the control group was in sham ultrasound exposure (0 kPa).
Analysis
The targeted UCA adhesion in the cremaster microvasculature was observed by laser confocal microscopy (TCS SP5, Leica Microsystems, Wetzlar, Germeny) 10 minutes after ultrasound insonation and removal of the cremaster muscle from the body. The cremaster sample was magnified 630-fold using a 63× oil immersion objective and photographed using a high-resolution charge-coupled device camera. Fluorescent microbubbles in the cremaster vasculature were illuminated using a filter set specific for FITC (λex = 490–495 nm and λem = 520–530 nm). Each vessel was visualized from anterior to posterior of the vessel wall. Quantification of UCA adhesion was determined by green fluorescence intensity within the vessels between 7 and 20 μm in diameter in each sample. Image-Pro Plus software (Media Cybernetics, Inc., Silver Spring, MD) was employed to analyze the data of the mean intravascular fluorescent area (the measured fluorescent areas divided by total vessel area) and the integrated optical density (IOD) (mean fluorescent density multiplied by fluorescent area) per intravascular area. The data were presented as mean intravascular fluorescent area per venule ± standard deviation and as mean IOD per venule ± standard deviation.
In the rat aorta study, the retained UCA on the aortic wall was observed by scanning electron microscopy (SEM). To examine the endothelial surfaces, the proximal end of the insonated abdominal aorta was first cut open to drain the blood until it stopped 10 minutes after insonation. Then a 5 mm segment in the middle of the targeted aorta was carefully cut and harvested using microcirculation scissors. The sample was then prepared for SEM by cropping out the anterior wall and two lateral walls, so only an approximately 5 mm × 1 mm segment of the posterior wall was left. During the procedure, the posterior wall was carefully protected without touching. Then the aortic lumen was gently rinsed in phosphate-buffered saline buffer and fixed in glutaraldehyde overnight. The tissues were prepared for SEM imaging using serial ethanol dehydration and critical point drying. The tissues were then mounted to SEM stubs with silver paste and sputter-coated with 100 Å of gold. The number of retained UCAs was counted in 10 continuous fields of view under an electron scanning microscope.
For quantification of UCA targeting adhesion, a visual analogue scale (Table 1) was used to estimate the bubble retention. The mean score and standard deviation were calculated using Microsoft Excel 2007 (Microsoft Corporation, USA).
Visual Analogue Scale Scoring Standard

Statistics
In all studies, the statistical significance between groups was subjected to one-way analysis of variance, which assumes that the population variances are equal. A p value less than .05 was deemed statistically significant, and all data were analyzed using SPSS 13.0 software (SPSS Inc, Chicago, IL).
Results
The larger anti-ICAM-1 microbubbles shone ring-like bright green fluorescence under fluorescence microscopy at 400× magnification (Figure 1), but the images of the submicron ones were displayed like fluorescent dots. The diameters of the targeted UCAs ranged from 1 to 4 μm, with an average diameter of 3 μm, and a bubble concentration of 4 to 9 × 106/mL. The size distributions of the nontargeted microbubbles exhibited a normal distribution, but the two targeted UCAs did not show a standard normal distribution, with less than 0.5% of the particles greater than 8.0 μm, in diameter (Figure 2). A small distribution peak of the anti-ICAM-1 microbubble was present around 4 to 5 μm. For the binding ratios calculated from the two flow cyctometers, the nontargeted control UCA was 17.3% and 0.15%, whereas the ratios of anti-ICAM-1 and anti-CD34 UCAs were as high as 94.7 ± 1.4% and 74.9 ± 6.7% (Figure 3 and Figure 4), respectively. The binding ratios were different on nontargeted UCAs, possibly owing to the different sensitivity of the two cytometers.

The targeted microbubble conjugated with anti-ICAM-1-FITC monoclonal antibody shone ring-like green fluorescence under fluorescence microscopy (400×). Scale bar represents 25 μm.

Size distributions of the nontargeted and two targeted ultrasound contrast agents used in these experiments. Malvern Mastersizer analysis was used to determine the microbubble (MB) size characteristics. ICAM-1 5 intercellular adhesion molecule 1.
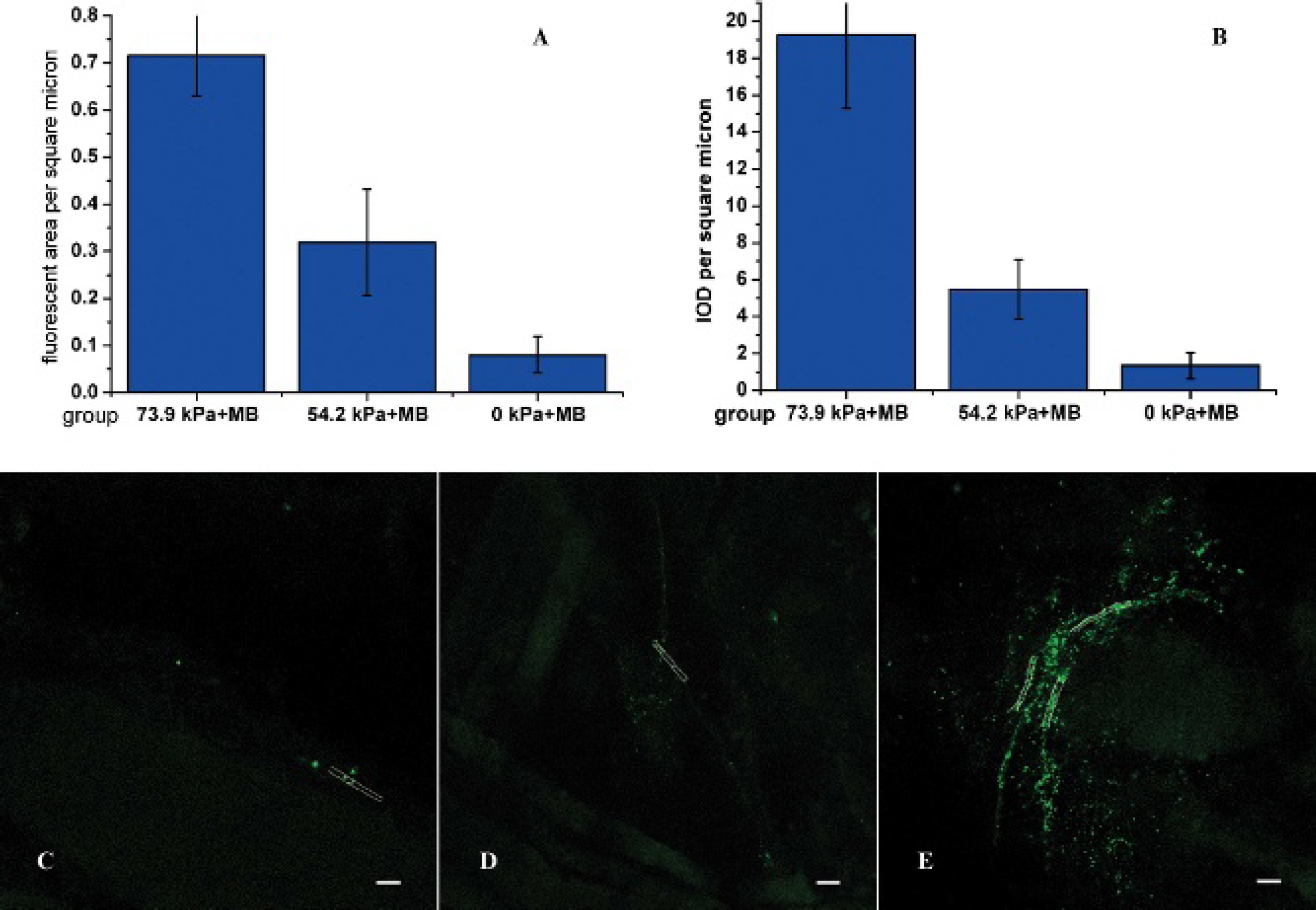
The fluorescent images of the anti-ICAM-1 targeted microbubble retention in the microvasculature of mice cremaster. Microbubble retention was observed by laser scanning confocal microscopy (630×). The upper panel shows the mean fluorescent area (A) and the integrated optical density (IOD) values (B) of retained microbubbles per venule ± standard deviation in each group. A few weak green fluorescent particles could be seen in the 0 kPa group (C). More green fluorescent particles and branches were found in the 54.2 kPa ultrasound radiation force (USRF) group (D). Significant integrated vasculature shining green fluorescence was found in the 73.9 kPa USRF group (E). Some vessel walls are outlined in white. Scale bar represents 50 μm.
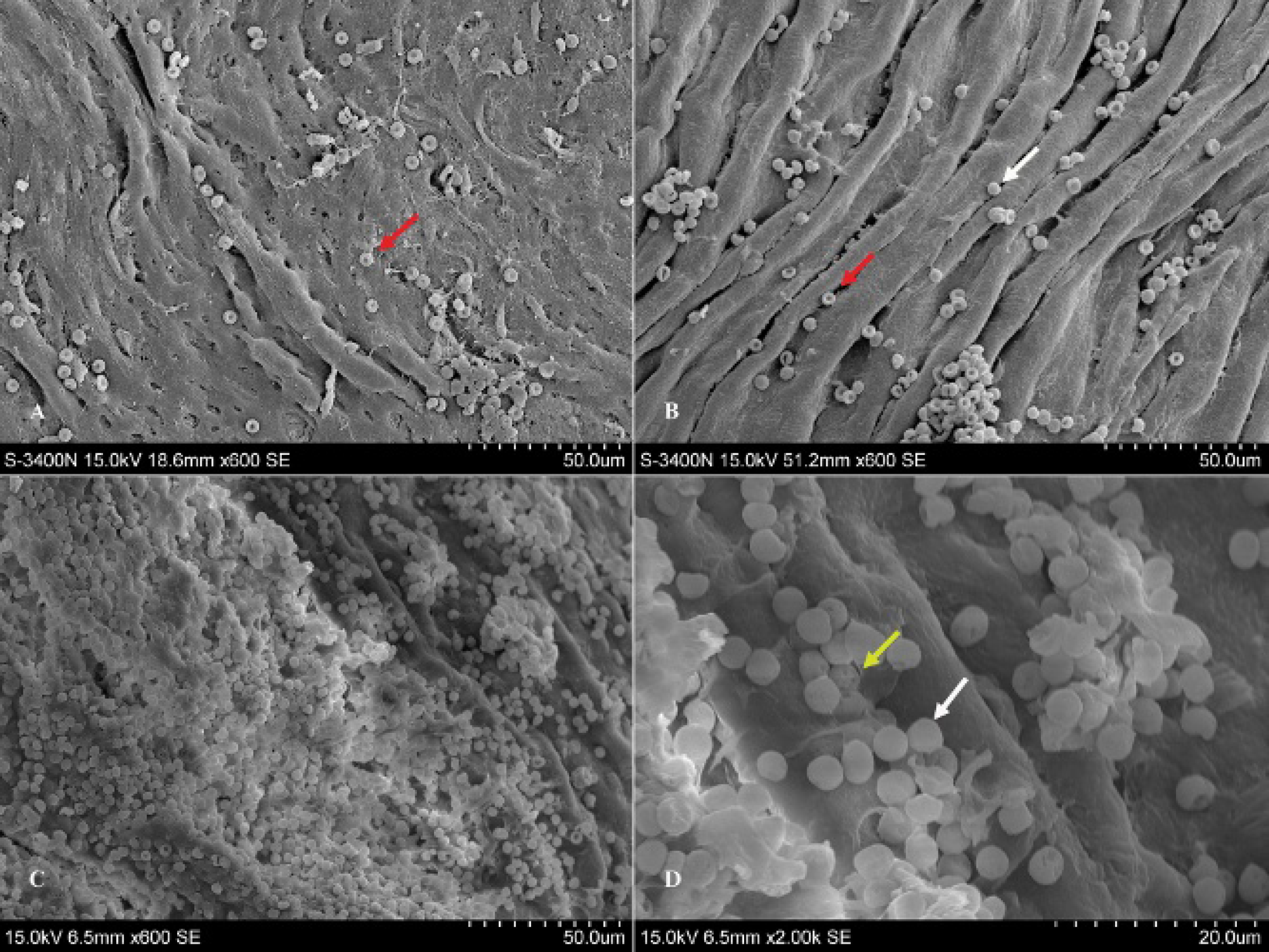
Scanning electron microscopy images of the anti-CD34 targeted microbubble retention on the endothelium of rat abdominal aorta. A few bubbles could be spot adhered to the vascular endothelia in the control group without ultrasound radiation force (USRF) application (A). Increased targeted microbubble retention (white arrow) on the aortic endothelia with application of 54.2 kPa USRF (B). The red arrows indicate erythrocytes with a biconcave shape (A, B). A huge number of microbubbles attached to the aortic endothelia in the 73.9 kPa USRF group (C). These microbubbles (white arrow) had a tendency to aggregate. Tiny pores (yellow arrow) and some deformation were found in the surface of the microbubbles (D).
The increases in the fluorescent visual intensities and areas of the mice cremaster microcirculation in the two USRF groups were visually more significant when compared to the control. Few fluorescent spots could be seen in the microvasculatures of the 0 kPa group (see Figure 3C). With the application of 54.2 kPa USRF treatment, some scattered green fluorescent particles could be visualized along with the vasculatures (see Figure 3D). Especially in the 73.9 kPa group, integrated fluorescent branch vessels in the cremaster usually appeared (see Figure 3E). The UCA retention area and IOD in the 73.9 kPa group were much higher than those of the 54.2 kPa group and the control group (Table 2). The average intravascular fluorescent area of the 73.9 kPa group was increased approximately 9-fold and 2.3-fold over that of the 0 kPa control group and the 54.2 kPa group, respectively. The IOD of the 73.9 kPa group showed approximately 14.4-fold and 3.5-fold increases over that of the 0 kPa group, and the 54.2 kPa group, respectively (see Figure 3, A and B).
Mean Intravascular Fluorecent Area (Posterior Wall) per Vessel Segment and Mean Integrated Optical Density per Vessel in Cremaster Microvasculature

IOD = integrated optical density.
p < .05 compared to the 0 kPa group.
Data were computed from laser confocal microscopy offline.
In the rat study, the diameter of the abdominal aortas ranged from 3.5 to 4.0 mm. SEM was successfully performed in all specimens. Only the intact microsphere without the biconcave sign was considered the targeted microbubble and was taken into account for quantification. The results of the visual score are shown in Table 3. The microbubble attached to the aortic endothelium appeared to be huge in number in the 73.9 kPa group (see Figure 4). The number of microbubbles per sight (210 × 147 μm2, 630×) was countless and could be in several thousands, with an average score of 3.37 on a visual analogue scale. As expected in the 0 kPa group, the number of microbubbles retained on vascular endothelium without USRF was rare and fewer than 5 per sight, with a mean score of 0.47. In the 54.2 kPa group, the resting microbubbles were a little more than that of the control group, with a mean score of 1.07. Erythrocytes were easily discriminated by the peculiar biconcave shape. In addition, some tiny holes smaller than 0.5 μm could be found in the surface of some microbubbles at the magnification of 2,000× (see Figure 4).
Visual Scores of Retained Microbubbles on the Posterior Endothelia of Rat Abdominal Aortas

p < .05 compared to the 0 kPa group.
Retained microbubbles were observed by scanning electron microscopy and were scored according to a visual analogue scale.
Discussion
Microbubble-based targeted ultrasound contrast imaging highly relies on the binding of targeted microbubbles to the specific target. Unlike the contrast media in computed tomography or nuclear medicine, the microbubble UCA is a micron-scale particle, ranging from 2 to 8 μm. It cannot penetrate the vascular wall and is unable to find the target in the interstitial space. So only the molecular receptors within the vascular lumen can be used for targeted binding.
A major limitation of microbubble-based molecular imaging is related to the central axial localization of UCA in a laminar blood flow pattern.15–17 The shear forces imposed by blood flow prevent the targeted UCA with specific molecules from crossing the blood streamline to find the corresponding receptors on the endothelium. So this limitation in UCA targeting may explain why we cannot obtain visual enhancement by contrast second harmonic imaging. 23 Under this condition, it might be very difficult to practice microbubble-based molecular imaging in a clinic.
The effects of USRF on the bubble were first found by Bjerknes 24 and first applied by Dayton and colleagues in microbubble contrast agent manipulation. 25 The mechanism could be explained by primary and secondary radiation forces. The primary radiation force drives compressible objects at their resonant frequency, and the secondary radiation force can be a kind of force that causes the bubbles to attract each other.24–26
For this reason, USRF was used to push microbubbles across central flow for closer contact with the target in many studies.19,22,27–29 Zhao and colleagues demonstrated that the number of biotinylated microbubbles stuck to an avidin-coated synthetic vessel increased as much as 20-fold by using USRF driven at 3 MHz and 14 kPa. 27 The adhesion of UCA targeted to αvβ3 integrin expressed on endothelial cells of human umbilical vein increased 27-fold within a mimetic vessel when radiation force was applied at 3 MHz and 40 kPa. 27 The most significant study showed that USRF enhanced microbubble targeting nearly 80-fold to an in vitro P-selectin-coated flow chamber at 2 MHz and 122 kPa. 22
In spite of the high increase in microbubble retention up to 80-fold by using USRF in the above in vitro studies, Rychak and colleagues found that USRF treatment in vivo enhanced microbubble retention to P-selectin only 4-fold in mouse cremaster venules and femoral vein; it rose up to 20-fold in the femoral artery at a center frequency of 2.25 MHz and an ultrasound pressure of 50 kPa. 19
In this study, we investigated the impact of two different acoustic pressures on the targeting ability of targeted microbubbles in vivo. Two types of vessels, the inflamed cremaster microvasculature of the mouse and the normal abdominal aorta of the rat, were used to represent the flow conditions of the microvessel and the great vessel. Our results again proved the effects of USRF on targeted microbubbles done by Rychak and colleagues. 19 The mice model and some acoustic parameters used in this study were similar to those of Rychak and colleagues, but there were also some critical items that were different between our study and their work, such as targeted UCAs (anti-ICAM-1 microbubbles vs anti-P-selectin microbubbles), ultrasound frequency (1.1 MHz vs 2.25 or 5.0 MHz), ultrasound beam (plane vs focused), and acoustic pressure (73.9 kPa vs 50 kPa). 19
In the cremaster microcirculation experiment, laser confocal microscopy was used to verify the ability of USRF to assist microbubble adhesion. The mean intravascular fluorescent area representing microbubble retention targeted to ICAM-1 in cremaster venules rose approximately 9- and 4-fold, respectively, under ultrasound pressure of 73.9 kPa and 54.2 kPa than that of the control (0 kPa). This result was consistent with that of Rychak and colleagues. 19 The IOD not only represented microbubble retention but also suggested aggregation of the UCAs. The more microbubbles accumulated, the higher the IOD was in the same area. The mean intravascular IOD of the 73.9 kPa and 54.2 kPa group increased about 14.4-fold and 4.1-fold over that of the 0 kPa group, respectively (see Figure 3B). The higher increase in mean IOD over that of the mean intravascular area might indicate the tendency of microbubble aggregation and was significant under the pressure of 73.9 kPa.
As to the rat abdominal aorta experiment, USRF can also enable microbubble migrating toward the endothelium in great vessels, just as in microcirculation. SEM was employed to determine the adhesion of microbubbles on the surface of endothelia. SEM can provide direct vision of bubble adhesion instead of echodecorrelation or frequency-domain analysis, both of which are indirect methods for quantifying microbubble adhesion. 30 For the first time, we found that a huge number of microbubbles (probably thousands of bubbles) accumulated on the aortic endothelium per sight (210 × 147 μm2) with the help of 73.9 kPa USRF, but few microbubbles attached without USRF. Although the average visual scores rose only from 0.47 (the 0 kPa group) to 3.37 (the 73.9 kPa group), the actual number of microbubbles attached to the aortic endothelium could be over a thousandfold when compared to the control.
It is reported that significant clustering of UCAs usually happens at the same time as UCAs migrating after USRF application, with up to 80% of the adherent UCAs occurring in multiparticle aggregates. 22 This was believed to be the effect of secondary radiation force, which frequently happens at the resonant frequency of microbubbles. 18 In most studies, microbubble resonant frequencies (about 2–3 MHz) were chosen as the central frequency for UCA displacement, so UCAs tended to aggregate with USRF. In our previous study, USRF at 2 MHz tended to aggregate more bubbles than that of 1.1 MHz in a flow chamber, but 1 MHz was also validated in pushing the microbubbles. 31 To obtain more UCA adhesion to endothelium, we assume that 1.1 MHz ultrasound treatment may reduce the aggregation of bubbles, which might increase wider contact between the microbubble and the vessel wall.
Acoustic radiation has been investigated to enhance targeted UCAs conjugated to antibody of ICAM-1, vascular cell adhesion molecule 1 (VCAM-1), fibrin, RGD peptide P-selectin, 8 ′ 22 ′ 30 and &αvβ3-expressing cells 27 in vitro using various flow chambers. In this study, we used the anti-CD34 antibody as the targeting ligand to find mature endothelial cells. CD34 is a physiologic molecular marker of mature endothelial cells and endothelial progenitor cells. In peripheral blood, endothelial progenitor cells are almost nonexistent, so CD34 is mainly a target for endothelial cells. The reason why we chose CD34 is that the expression of CD34 on normal mature endothelium is stable, and this can reduce the error caused by differences in expression of other targeted molecules in individual mice or even various vascular endothelia in a rat. The results show that USRF can also promote the targeted CD34 microbubble adhesion significantly in rat abdominal aorta. Under SEM, thousands of microbubbles were found attached to the aortic endothelial area, which has not been reported in previous experiments and in the literature. From the results we can conclude that the targeted UCA could be manipulated significantly by using USRF, which not only confirms the results of previous studies but also demonstrates the possibility of further targeted ultrasound imaging or improvement in drug delivery by using the technique.
Our study had several limitations. In the mouse study, the cremaster muscle was removed for fluorescent observation of the targeted microbubbles. We cannot guarantee that all of the bubbles observed under the fluorescent microscope were from targeted microbubbles; a few of them might have been the bubbles trapped in the vessel after the cremaster was removed. In the rat study, we did not estimate the wall shear rate of the vessel, which is an important factor of microbubble accumulation. The targeted UCA displacement and accumulation could decrease with increasing the wall shear force rate. 22 We did not take the differences of ICAM-1 expression into consideration between mice or various vasculatures, which result in differences of ICAM-1 microbubble retention. The visual analogue score was not a precise method for microbubble quantification.
Conclusions
We have confirmed the ability of acoustic radiation force to manipulate targeted UCA adhesion in both small and great vessels in vivo, particularly in the normal rat aorta as a model of great vessels. SEM was initially employed for direct observation of the UCA adhesion on aortic endothelia. USRF treatment did produce a significant increase in UCA retention on aortic endothelium.
Footnotes
Acknowledgments
We thank Dr. Jianping Bin and Dr. Lijng Ji for directing the animal model preparation.
Financial disclosure of authors: This work was supported by the National Natural Science Foundation of China (No. 30772070).
Financial disclosure of reviewers: None reported.