
Abstract
The purpose of this study was to assess the relationship of mammographic breast density (BD) and cell proliferation/focal adhesion kinase activation–seeking radiotracer technetium 99m pentavalent dimercaptosuccinic acid (99mTc(V)-DMSA) uptake in women with different breast histologies, that is, mild epithelial hyperplasia (MEH), florid epithelial hyperplasia (FEH), mixed ductal carcinoma in situ with invasive ductal carcinoma (DCIS + IDC), and pure IDC. Fifty-five women with histologically confirmed mammary pathologies were submitted preoperatively to mammography and 99mTc(V)-DMSA scintimammography. The percentage and intensity of 99mTc(V)-DMSA uptake and the percentage of BD were calculated by computer-assisted methods and compared (t-test) between the breast pathologies. In breasts with increased BD, FEH and DCIS + IDC were found. On the contrary, pure IDC and MEH were identified in breasts with significantly lower BD values. In breasts with increased 99mTc(V)-DMSA area and intensity of uptake, FEH was the main lesion found compared to all other histologies. Linear regression analysis between BD and 99mTc(V)-DMSA uptake area and intensity revealed significant coefficients of correlation (r = .689, p < .001 and r = .582, p < .001, respectively). Increased BD correlates with the presence of FEH and mixed DCIS + IDC but not with pure IDC or MEH. Its close relationship to 99mTc(V)-DMSA, which also showed an affinity to FEH, indicates that stromal microenvironment may constitute a specific substrate leading to progression to different subtypes of cancerous lesions originating from different pathways.
INCREASED MAMMOGRAPHIC BREAST DENSITY (BD) is associated with increased risk for breast cancer in the general population.1–3 Recent studies have demonstrated that BD is associated with an increased occurrence not only of invasive ductal carcinoma (IDC) but also of ductal carcinomas in situ (DCIS) 4 and even of florid epithelial hyperplasia (FEH), 5 which could constitute potential precursors in the process of mammary carcinogenesis. The biologic basis of augmented breast cancer risk in women with high BD has not been clarified. It is still unknown whether the stroma, epithelium, or both play a key role in the malignant transformation of dense fibroglandular breast tissue. 1 There is accumulating evidence that many growth factors, such as platelet-derived growth factor (PDGF), insulin-like growth factor (IGF), vascular endothelial growth factor (VEGF), and calcitonin gene–related peptide (CGRP), can act directly or indirectly and activate several pathways in the carcinogenic process.6–14
Technetium 99m pentavalent dimercaptosuccinic acid (99mTc(V)-DMSA) is a well-known cell proliferation–seeking radiotracer with affinity for neuroendocrine and soft tissue tumors, such as medullary thyroid carcinoma and lung, breast, brain, and metastatic bone lesions. 15–27 Based on in vivo scintigraphic studies, we initially suggested that its cellular uptake mechanism is closely related to cellular proliferation, as expressed by the Ki-67 immunohistologic index28–30 and at the same time independent from estrogen receptor (ER) status.23,24 Denoyer and colleagues elucidated the exact mechanisms: the tracer reflects phosphate ion (Pi) transport and metabolism, entering cancer cells specifically via the type III Na/Pi cotransporter, this uptake being driven by the cellular levels of phosphorylated (ie, activated) focal adhesion kinase (FAK), a keystone of accelerated proliferation.26,27
Recent in vivo and in vitro studies have demonstrated its potential to depict increased cellular proliferation not only in invasive carcinoma but also in epithelial hyperplasia of the usual type and in preinvasive mammary lesions (ie, DCIS), independently of the presence of estrogen and progesterone receptors.15,26–33 This retrospective study aimed at identifying a possible relationship between mammographic BD and scintimammographic 99mTc(V)-DMSA uptake in various breast histologies. It also investigated whether women with dense breasts, possibly disclosing or expressing a proliferating potential, could be discriminated visually or on the basis of semiquantitative analysis of 99mTc(V)-DMSA intensity of uptake and benefit from biopsy and possible proper chemoprophylactic treatment.
Materials and Methods
From a cohort of women scheduled for breast surgery during the previous 2 years owing to suspicious findings on palpation and/or mammography, we selected 55 (mean age 53.2 ± 11.8 years) who had a complete set of presurgical tests, that is, mammography and 99mTc(V)-DMSA scintimammography. Histology in this population revealed lesions classified as follows:
Benign nonproliferating, constituting mild epithelial hyperplasia (MEH) of the usual type or papillary apocrine change (n = 20)
FEH of the usual type (n = 10) (Figure 1),
DCIS, alone or associated with IDC (DCIS ± IDC, n = 17)
Pure IDC (n = 14).
Informed consent was acquired in every case prior to scintimammography. The study was in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee and Scientific Board of our hospital.
99mTc(V)-DMSA Scintimammography and Image Analysis
99mTc(V)-DMSA was prepared using a domestically available kit (DMS(V)/Demoscan, National Center of Physical Sciences, Institute of Radioisotopes and Radiodiagnostics Demokritos, Athens, Greece) labeled with 99mTc within our Department of Nuclear Medicine. Scintimammography was performed on a single-head gamma camera (Sophycamera DS7, Sopha Medical Vision International, Buc Cedex, France) equipped with a high-resolution, parallel-hole collimator and connected to a dedicated computer (Sophy NxT, Sopha Medical Vision International). The matrix was set at 256 × 256 pixels, and the photopeak was centered at 140 keV, with a symmetric 10% window. Lateral prone early and late planar images (at approximately 10–20 and 60–70 minutes, respectively) were acquired after intravenous administration of 925 to 1,100 MBq tracer activity. Acquisitions were obtained using a special positioning pad (PBI-2 Scintimammography Pad Set, Pinestar Technology Inc., Greenville, PA).
Breast radiotracer uptake in early and late images was first evaluated visually. Any focally increased accumulation was regarded as associated with invasive pathology, whereas any other pattern of a more widespread diffuse uptake was considered as corresponding to preinvasive lesions (DCIS, FEH), in accordance with our previous reports.29,30 Therefore, comparison of the focal radiotracer uptake in IDC with the other groups was considered unnecessary and irrelevant to our purpose of discriminating the nature of the underlying lesion.
Semiquantitative analysis was also performed by two independent researchers. Radiotracer uptake area was calculated at the late (60-minute) images by drawing regions of interest (ROI) encompassing the total breast and the area of focally and/or diffusely increased tracer uptake in the lateral view; then we divided the number of pixels within these two regions. We repeated the aforementioned procedure in the anterior scintigraphic image, and the average tracer uptake area of these two views was considered the tracer uptake area of the breast under investigation. Lateral and anterior breast images were processed using Mirage Processing Station's toolbox software 5600 (Segami Corporation, Paris, France) connected to the Sophycamera DS7.
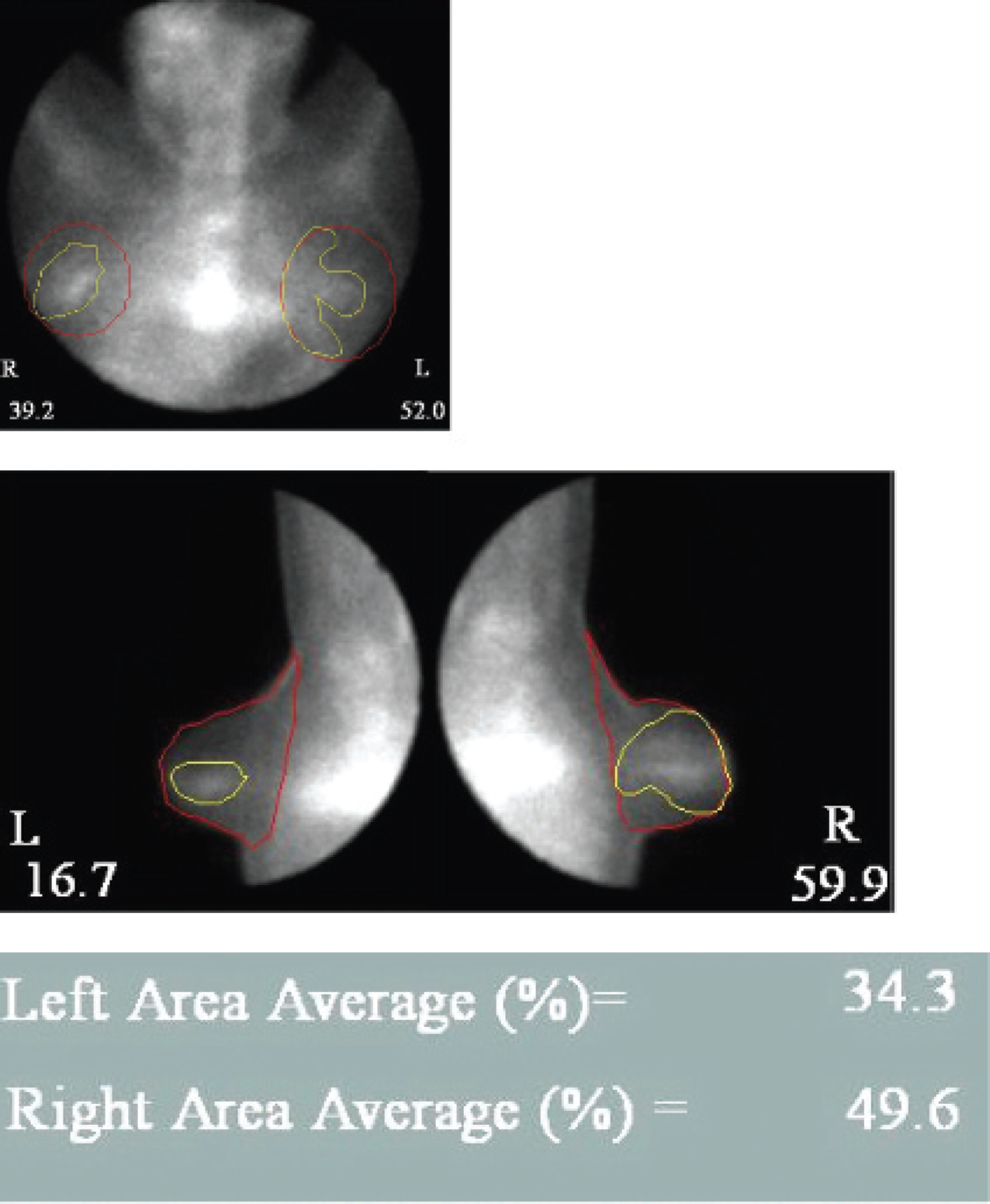
A patient with florid epithelial hyperplasia in both breasts.
Semiquantitative analysis also included study of the intensity of uptake of the radiotracer by calculating the lesion to background (L/B) activity ratios in the areas of increased radiotracer uptake, by drawing an ROI of standardized size and shape over the maximal activity area and over the surrounding normal breast, and then dividing the ROI-encompassed activity counts. L/B calculation was performed in late images (hereafter referred to as L/BLATE), representing the intensity of parenchymal accumulation. 18 If there was a large deviation between the measurements of the two researchers, a third one would perform the semiquantitative analysis as well.
Mammography and Image Analysis
Craniocaudal and mediolateral views of all presurgical mammograms were digitized using a high-resolution x-ray scanner (UMAX PowerLook 2100XL, UMAX Systems GmbH [USG], Willich, Germany). All images were captured at 300 dpi 14-bit grayscale depth. Using Image J version 1.38g, a Java-based image processing software (Research Services Branch, National Institutes of Mental Health, Bethesda, MD), two independent researchers manually drew an ROI (by polygon selections) that defined the whole breast area and the dense breast area in both craniocaudal and mediolateral views. The dense breast area (as the percentage of the whole breast area) was determined in a manner similar to the scintigraphic estimation of radiotracer uptake area as described earlier; we calculated the dense breast area in craniocaudal and mediolateral views by dividing the areas encompassing the total breast and the area of dense breast and then averaged these two ratios. In case of a large deviation between the two researchers, a third researcher would perform the breast density measurements as well.
Histology
In our study, MEH and papillary apocrine change comprised the group of benign nonproliferating lesions. FEH of the usual type included moderate or severe ductal epithelial hyperplasia (without atypia). The distinction criteria between FEH and MEH were based largely on epithelium thickness: in moderate hyperplasia, the epithelium is five or more cell layers thick. In some instances, strands of epithelium extend across or bridge the lumen, resulting in the formation of secondary glandular spaces in the hyperplastic epithelium. The distinction between moderate and severe hyperplasia is not sharp. In general, the affected ducts are appreciably enlarged and the luminae are nearly or completely filled by the proliferating epithelium. Thus, we decided to use the term FEH regarding cases of moderate or severe epithelial hyperplasia of the usual type.
Data Analysis
Linear regression analysis was performed between dense breast area and radiotracer uptake area and intensity at 60 minutes. Continuous data are expressed as mean ± standard deviation. Dense breast area and radiotracer uptake area and intensity were compared between the different histologic groups using the nonparametric, two-sided Mann Whitney U test. For all comparisons, a p value less than .05 was considered significant.
Results
Histology revealed 20 cases of MEH or papillary apocrine change, 10 cases of FEH, 17 cases of DCIS (4 pure and 13 associated with IDC), and 14 cases of pure IDC.
The lesions presented in breasts with increased BD were FEH and DCIS + IDC. On the contrary, pure IDC and MEH were found in breasts with significantly lower BD values. FEH was the breast lesion found in breasts with a greater percentage of 99mTc(V)-DMSA area and intensity of uptake compared to all other histologies, which were found to show significantly lower %99mTc(V)-DMSA uptake area and intensity. Linear regression analysis between BD and 99mTc(V)-DMSA uptake area and intensity in the whole patient population revealed significant coefficients of correlation (r = .689, p < .001 and r = .582, p < .001, respectively; Figure 2 and Figure 3). Table 1 summarizes the descriptive characteristics in each histologic group, including age, mammographic BD, and radiotracer uptake area and intensity. Table 2 displays the p values estimated for comparisons between the histologic groups (MEH, FEH, and DCIS) regarding the studied mammographic and scintigraphic imaging parameters.
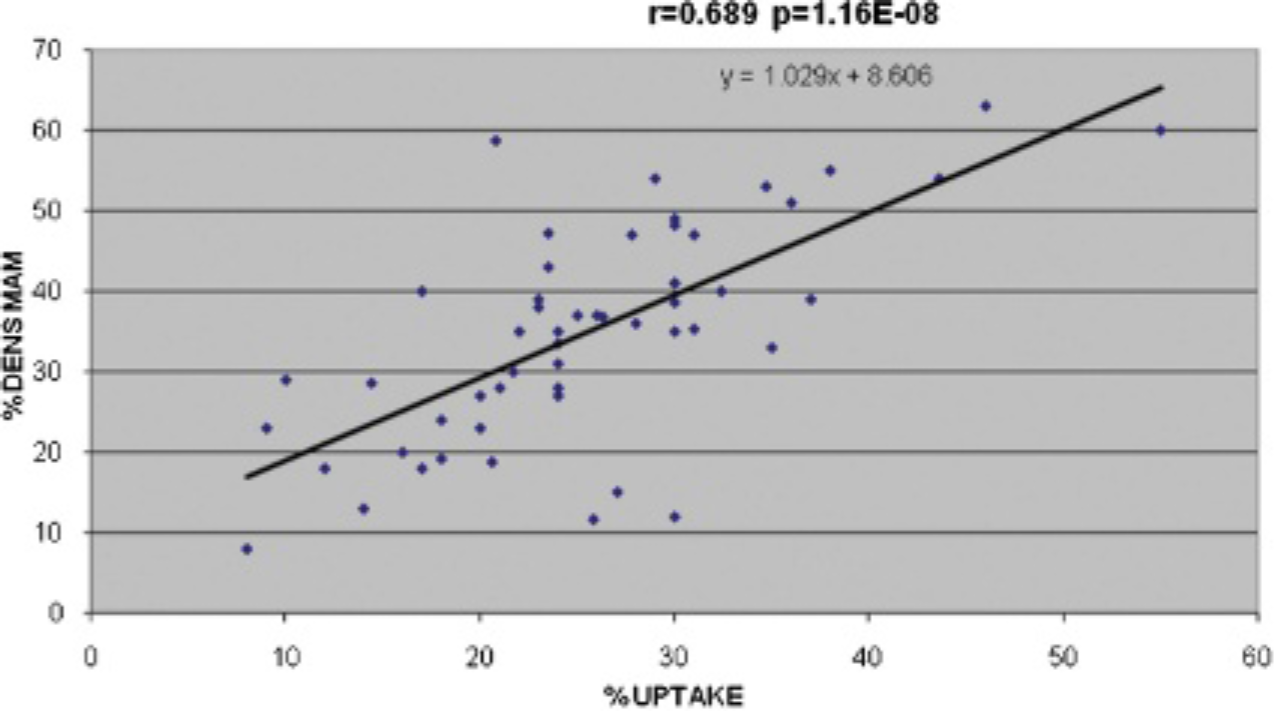
Overall linear regression analysis between breast density and 99mTc(V)-DMSA uptake area revealed a significant coefficient of correlation.
Discussion
The findings of this study indicate that FEH and DCIS ± IDC were associated with significantly increased %BD compared to MEH and pure IDC. Reports from the recent literature are in agreement with our findings regarding the incidence of FEH and DCIS ± IDC in women with increased BD. However, these studies were performed on isolated groups of breast lesions without attempting a direct comparison of %BD in different breast histologies.1,4–8 Boyd and colleagues, using a methodological model similar to ours, tried to identify the relative risk of various breast histologies with respect to %BD. 32 Surprisingly, they found that the higher relative risk between the above-mentioned breast lesions for women with > 75% BD involved severe epithelial hyperplasia followed by DCIS and nonproliferating breast lesions.

Overall linear regression analysis between breast density and 99mTc(V)-DMSA uptake intensity revealed a significant coefficient of correlation.
In the present research, FEH was the histology with the highest mean values of breast density, 99mTc(V)-DMSA uptake area, and intensity (L/B at 60 minutes).
All of these findings in conjunction with the strong correlation between %BD and 99mTc(V)-DMSA indices do not seem to be a simple coincidence. To support this suggestion, we tried to find a link between stromal microenvironment and 99mTc(V)-DMSA uptake. In our opinion, the most convincing evidence of a communicating network between anatomic stroma and functional factors was the estrogen-independent growth factors efficacy, FAK activation, and hypoxia found in increased BD and 99mTc(V)-DMSA activity.
Descriptive Statistics of the Age, Mammographic Breast Density Area, Scintimammographic Radiotracer Uptake Area, and Radiotracer Intensity

BD = breast density; DCIS = ductal carcinoma in situ; FEH = florid epithelial hyperplasia; IDC = invasive ductal carcinoma; L/B60 = radiotracer intensity: lesion to background ratio at 60 minutes; MEH = mild epithelial hyperplasia; RU = radiotracer uptake.
It has been demonstrated that the carcinogenic potential in dense breasts is independent of circulating sex hormones. 33 Furthermore, growth factors such as IGF, as well as mitogenic and angiogenic factors such as PDG and CGRP, have been reported to be associated with %BI exerting an autocrine activity through the stroma.34–37 99mTc(V)-DMSA uptake is also independent of ER. 33 A the same time, a relationship between 99mTc(V)-DMSA uptake and overexpression of the aforementioned growth factors PDGF and CGRP has been identified in cancerous cell lines10,37,38 and in premalignant, preinvasive, and invasive breast lesions in vivo. 11
Probability Values of Mammographic and Scintimammographic Comparisons between the Histologic Groups, Estimated by Mann-Whitney U Test

BD = breast density; DCIS = ductal carcinoma in situ; FEH = florid epithelial hyperplasia; L/B60 = radiotracer intensity: lesion to background ratio at 60 minutes; MEH = mild epithelial hyperplasia; NS = nonsignificant difference; RU = radiotracer uptake.
Another interesting common finding that could explain the above-mentioned convergencies and support the suggestion that 99mTc(V)-DMSA could image a hidden proliferative potential in dense breasts is that cells grown in a dense medium show increased expression of phosphorylated forms of FAK, a precocious state of malignant cell transformation. Denoyer and colleagues showed a strong correlation of 99mTc(V)-DMSA uptake and FAK in different cancerous cell lines. 26 Activated FAK has also been demonstrated to be overexpressed in premalignant compared to invasive breast lesions.39,40 Taking into account all the aforementioned data, we consider the increased 99mTc(V)-DMSA uptake in FEH and DCIS ± IDC as not incidental.
Women with FEH comprise a large group of patients at risk of developing breast cancer, although only some lesions will finally evolve to malignancy. On investigating the status and prospects of imaging cell proliferation, the positron emission tomography (PET) tracer 3‘-deoxy-3‘-[18F]fluorothymidine (FLT) has been shown to be most promising in monitoring tumor response rather than detecting primary tumors, needless to mention imaging (detection) of early proliferative lesions, such as FEH.41,42 Furthermore, the most commonly applied PET tracer, [18F]fluorodeoxyglucose (18F-FDG), has provided ambiguous findings and has proved inadequate to estimate the tumor biologic behavior of breast cancer, including cell proliferation, differentiation, histopathologic grading, and axillary lymph node status.42–44 Therefore, given that hitherto no other available imaging modalities may assist in detecting lesions with a considerable potential to progress to breast cancer, we have reasons to suggest that 99mTc(V)-DMSA scintimammography in combination with mammography may substantially contribute toward the visualization of these lesions.
Conclusion
Increased BD correlates with the presence of FEH and mixed DCIS + IDC but not with pure IDC or MEH. Its close relationship to the proliferation-seeking radiotracer 99mTc(V)-DMSA, which also showed an affinity to FEH, indicates that stromal microenvironment may constitute a specific substrate leading to progression to different subtypes of cancerous lesions (DCIS + IDC) totally different from pure IDC originating from different pathways.
Footnotes
Acknowledgments
We would like to thank Mr. Andreas Tsigris for pledging valuable support to the mammographic breast density measurements.
Financial disclosure of authors and reviewers: None reported.