
Abstract
Global expression profiling of pancreatic cancers has identified two cell surface molecules, claudin 4 and prostate stem cell antigen (PSCA), as being overexpressed in the vast majority of cases. Two antibodies, anti-claudin 4 and anti-PSCA, were radiolabeled with iodine 125 (125I) for imaging pancreatic cancer xenografts in mice using gamma scintigraphy and single-photon emission computed tomography-computed tomography (SPECT-CT). Immunofluorescence staining of intact and permeabilized Colo357 human pancreatic cancer cells showed strong extracellular staining by both anti-PSCA and anti-claudin 4. Biodistribution studies in claudin 4 and PSCA-expressing Colo357 and PANC-1 subcutaneous xenograft models in mice showed that [125I]anti-claudin 4 tumor to muscle ratio uptake was 4.3 in Colo357 at 6 days postinjection and 6.3 in PANC-1 xenografts at 4 days postinjection. Biodistribution of [125I]anti-PSCA showed tumor to muscle ratio uptake of 4.9 in Colo357 at 6 days postinjection. Planar gamma scintigraphic imaging in Colo357 xenograft-bearing mice showed clear tumor uptake of [125I]anti-claudin 4 by 24 hours postinjection and by 48 hours postinjection for [125I]anti-PSCA. SPECT-CT imaging with [125I]anti-claudin 4 and [125I]anti-PSCA in an L3.6PL orthotopic xenograft model showed strong tumor and spleen uptake at 5 days postinjection. Both anti-claudin 4 and anti-PSCA demonstrate promise as radiodiagnostic and possibly radiotherapeutic agents for human pancreatic cancers.
IN 2006, 213,000 people globally are expected to be diagnosed with pancreatic cancer and 213,000 people are expected to die from the disease. 1 Diagnosis of pancreatic cancer is often obtained after fine-needle biopsy of a suspicious lesion detected by magnetic resonance imaging or computed tomography (CT), but by then, metastases are usually evident.2–4 Patients with metastases or other reasons for nonresectable disease have a median survival of only 6.8 months. 5 Typically, only 10% of patients diagnosed with pancreatic cancer are candidates for surgical resection with curative intent. Even for those who are eligible for surgery, the postoperative survival mean is only 17 months. 6 The low survival rate is a direct result of the advanced stage at which the disease is detected and lack of suitable markers that could be useful for screening. For those patients presenting with known or suspected pancreatic cancer, new methods of detection to locate primary and metastatic lesions that also have curative potential are urgently required. In addition, for patients with established advanced disease, novel strategies for targeted therapies are needed that can potentially bypass the minimal impact of conventional anticancer agents in this disease.
Global expression analysis of pancreatic cancers using a multitude of platforms (serial analysis of gene expression, complementary deoxyribonucleic acid [DNA], and oligonucleotide microarray analyses) have revealed that claudin 4 and prostate stem cell antigen (PSCA) are up-regulated in the vast majority of human pancreatic cancers.7,8 Claudin 4 is a 22 kDa transmembrane receptor normally found in tight junctions. Claudin 4 is strongly expressed within virtually all primary and metastatic pancreatic cancers and in most pancreatic intraepithelial neoplasia (PanIN) lesions, the histologic precursors of infiltrating ductal adenocarcinoma. 9 Claudin 4 is also expressed in normal breast, prostate, bladder, and gastrointestinal mucosa, although expression is substantially less than in pancreatic cancer tissue samples. PSCA is a 13.5 kDa glycosylated transmembrane protein normally expressed in the basal cells of prostate glandular tissue. PSCA is overexpressed in ≈ 80% of prostate carcinomas and correlates with a high Gleason grade, extracapsular spread, and androgen independence. 10 PSCA expression in the pancreas is highly specific for pancreatic adenocarcinoma, whereas PanINs also express PSCA in 40% of examined cases.7,11
Up-regulated expression in pancreatic cancer relative to normal tissue and possession of extracellular transmembrane domains make both claudin 4 and PSCA attractive candidates for radioimmunoscintigraphy and radioimmunotherapy. In particular, the high expression of claudin 4 in PanIN makes it attractive as an early marker of disease. 9 Despite being expressed early, claudin 4 expression is also maintained throughout metastatic progression. 9 An anti-claudin 4 monoclonal antibody (mAb) is commercially available, and an anti-PSCA polyclonal antibody was developed for radiolabeling with iodine 125 (125I). These 125I-labeled antibodies were examined both in vitro and in vitro for their ability to bind specifically claudin 4 and PSCA-expressing pancreatic cancer cells and xenografts in immunodeficient mice.
Methods
General
All cell culture media and reagents were purchased from Sigma (St. Louis, MO) unless otherwise mentioned. Radioiodine ([125I]NaI, carrier free) was purchased from MP Biomedicals (Costa Mesa, CA) and IODO-GEN from Pierce (Rockford, IL). RL-NHL cells (stock number CRL-2261) and PANC-1 cells were obtained from the American Type Tissue Collection (Manassas, VA), and Colo357 cells were provided by Caroline Hill (London Research Institute); L3.6PL cells, a highly metastatic variant of Colo357 cells, were provided by Isiah Fidler (The University of Texas M. D. Anderson Cancer Center, Houston). Anti-PSCA rabbit polyclonal antibody was generously provided by Robert E. Reiter (University of California, Los Angeles). 12 Anti-claudin 4 mouse mAb was purchased from Zymed Laboratories (San Francisco, CA), and anti-CD20 mouse mAb was purchased from Novus Biologicals (Littleton, CO). Rabbit anti-mouse-fluorescein isothiocyanate (FITC) secondary antibody was purchased from MP Biomedicals. Hoechst nuclear stain was obtained from Molecular Probes (Eugene, OR). Fluorescence microscopy was performed using a Nikon Eclipse E400 using the green (425–475 nm) and blue (350–450 nm) channels.
Radioiodination of Antibodies
Typically, 20 μg of purified antibody in 100 μL of phosphate-buffered saline (PBS), pH 7.5, was added to an iodogen-coated vial. [125I]NaI was then added to the vial as 2 to 5 mCi in 2 to 5 μL of 0.1 M NaOH, pH 10. The solution then sat at room temperature for 10 minutes before each labeling solution was loaded onto a PBS-equilibrated Sephadex G-25 desalting column (Amersham Biosciences, Piscataway, NJ) to remove unincorporated radioiodine. The radiochemical yield was typically 30 to 40%. The radiochemical purity met or exceeded 95%, as determined by instant thin-layer chromatography. Specific activities ranged from 20 to 35 μCi/μg. Antibodies were labeled within 24 hours of use and were stored in sterile PBS at 4°C after labeling and desalting.
Cell Culture
Colo357 cells were cultured as described previously 13 with the addition of penicillin (100 U/mL) and streptomycin (100 μg/mL; Invitrogen Corp., Carlsbad, CA). PANC-1 cells were cultured under the same conditions as Colo357. RL-NHL cells were cultured in RPMI 1640 medium with 2 mM L-glutamine adjusted to contain 1.5 g/L of sodium bicarbonate, 4.5 g/L of glucose, 10 mM HEPES, and 1.0 mM sodium pyruvate, 90%; fetal bovine serum, 10%; penicillin, 100 U/mL; streptomycin, 100 μg/mL. L3.6PL cells were cultured as described previously. 14
Immunofluorescence
Colo357 cells were grown in T175 flasks to ≈ 80% confluency before seeding into Lab-Tek II chamber slides at a density of 100,000 cells/well. Cells were allowed to attach over 48 hours before immunofluorescence staining.
RL-NHL cells were grown in T175 flasks as nonadherent spheroids. The spheroids were gently disrupted by pipetting before seeding into chamber slides at a density of 100,000 cells/well. Cells were allowed to settle over 48 hours prior to immunofluorescence staining.
Cell cultures were probed either in their native state with primary antibody or were fixed with 2% paraformaldehyde prior to the addition of the primary antibody. For cells that were probed in their native state, fixation with 2% paraformaldehyde for 30 minutes occurred following incubation with primary antibody.
Chamber slide cultures were then cooled to 4°C, where all immunofluorescence steps were carried out. All steps were followed by two washes with cold PBS, pH 7.5. Each chamber was first blocked with 5% goat serum in PBS for 1 hour. Primary antibody (anti-PSCA 1:1,000, anti-claudin 4 1:270, or anti-CD20 1:370) was applied in PBS to each slide and allowed to bind for 1 hour. Secondary antibody (rabbit anti-mouse-FITC conjugate, 1:100) was applied in PBS and allowed to bind for 30 minutes. Hoechst nuclear stain (1:3,000) was applied in PBS for 10 minutes. At this point, the chamber wells were removed and the slides were prepared for viewing with mounting media and a coverslip. Fluorescence microscopy was carried out using a Nikon Eclipse E400 fluorescence microscope equipped with a green and blue filter and digital camera.
Preparation of Xenograft Models
All in vivo experimental procedures were undertaken in compliance with US laws governing animal experimentation and were approved by the Johns Hopkins University Institutional Animal Care and Use Committee.
Subcutaneous Xenografts
Male severe combined immunodeficient (SCID) mice (18–20 g) were obtained from Charles River Laboratories (Wilmington, MA). They were inoculated either behind the forearm or in the flank with 1 to 3 × 106 cells in Hanks' Balanced Salt Solution and an equal volume of Matrigel (Becton, Dickinson and Company, San Jose, CA). Mice were imaged or used in biodistribution experiments when the tumors reached 7 to 10 mm (Colo357) or 1 to 3 mm (PANC-1) in diameter.
Orthotopic Xenografts
Male athymic nude mice were subcutaneously implanted with 1.5 × 106 L3.6PL cells until a palpable tumor xenograft was present. The tumor was then harvested and cut into 2 × 1 mm pieces. SCID mice were then anesthetized with 3.5% isoflurane in oxygen. An incision was then made in the left anterior flank to permit orthotopic placement of a freshly excised 2 mm diameter L3.6PL tumor xenograft fragment under the capsule of the pancreas. The tumor fragment was then secured with sterile sutures. The wound was then closed with a sterile wound clip, and the mice were monitored throughout recovery. Mice were imaged when the “pancreatic primary” tumors were first palpable. Following imaging experiments, necropsies were performed to confirm the presence of ≈ 4 mm diameter orthotopic tumors.
Rodent Biodistribution
Colo357 xenograft-bearing SCID mice were injected via the tail vein with 74 becquerels (Bq) (2 μCi, 5 μg/kg) of [125I]anti-CD20, [125I]anti-PSCA, or [125I]anti-claudin 4. PANC-1 xenograft-bearing SCID mice were injected with the same amount of either [125I]anti-claudin 4 or [125I]anti-CD20. Three to four mice each were sacrificed by cervical dislocation at 2, 4, and 6 days postinjection. The liver, kidneys, small intestine, bladder, muscle, heart, lungs, stomach, large intestine, spleen, and tumor were quickly removed. A 0.1 mL sample of blood was also collected. The organs were weighed and the tissue radioactivity was measured with an automated gamma counter (1282 Compugamma CS, Pharmacia/LKB Nuclear, Inc, Gaithersburg, MD). The percent injected dose per gram of tissue (% ID/g) was calculated by comparison with samples of a standard dilution of the initial dose. All measurements were corrected for decay.
Planar Gamma Scintigraphy
SCID mice, each bearing either a subcutaneous Colo357 human pancreatic carcinoma xenograft (7–10 mm in diameter) forward of the flank or an RL-NHL CD20+human lymphoma xenograft below the forearm, were anesthetized with intraperitoneal administration of a combination of ketamine (72 mg/kg), xylazine (6 mg/kg), and acepromazine (6 mg/kg). Mice were then injected intravenously via the tail vein with 7.4 MBq (200 μCi, 10 μg) of [125I]anti-CD20, [125I]anti-PSCA, or [125I]anti-claudin 4 in 200 μL of saline. Mice were then positioned on the bed of an X-SPECT small animal single-photon emission computed tomograpy (SPECT) scanner (Gamma Medica Inc., Northridge, CA) and were kept anesthetized using isoflurane in oxygen (0.5–1%, approximately 1 L/min). The mice were imaged following 2, 4, and 6 days of uptake using a low-energy, high-resolution parallel hole collimator (Gamma Medica) to obtain 10-minute static, planar scans.
SPECT-CT
Two female SCID mice each implanted with an orthotopic L3.6PL xenograft were injected intravenously with 185 MBq (5 mCi, 42 μg) of either [125I]anti-claudin 4 or [125I]anti-PSCA in saline. Every 48 hours, the mice were anesthetized first with acepromazine and ketamine as above and maintained under 1% isoflurane in oxygen. The mice were positioned on the X-SPECT (Gamma Medica) gantry and were scanned using two low-energy, high-resolution pinhole collimators (Gamma Medica) rotating through 360° in 6° increments for 60 seconds per increment. Immediately following SPECT acquisition, the mice were then scanned by CT (X-SPECT) over a 4.6 cm field of view using a 600 μA, 50 kV beam. The SPECT and CT data were then coregistered using the supplier's software (Gamma Medica) and displayed using AMIDE (<http://amide.sourceforge.net/). Data were reconstructed using the ordered subsets-expectation maximization algorithm.
Results
Immunofluorescence Staining of Colo357 Cells Reveals Extracellular Epitopes for Both Anti-Claudin 4 and Anti-PSCA
Antibodies directed against extracellular epitopes are likely more effective for in vivo imaging than antibodies directed against intracellular epitopes owing to superior access of antibodies to the former. 15 We undertook immunofluorescence imaging with both permeabilized and nonpermeabilized cells to determine if the anti-claudin 4 and anti-PSCA antibodies were directed against intracellular or extracellular epitopes, respectively. Figure 1 shows immunofluorescence images of Colo357 cells stained with anti-claudin 4, anti-PSCA, and negative control anti-CD20. In the upper panels, membrane staining by anti-claudin 4 and anti-PSCA of unfixed, nonpermeabilized cells demonstrates that these two antibodies do indeed recognize extracellular epitopes. The lack of staining by anti-CD20 indicates that both anti-claudin 4 and anti-PSCA staining are antigen specific. The bottom panels in Figure 1 show staining of permeabilized cells, demonstrating uniform, intracellular staining by anti-claudin 4 and anti-PSCA antibodies. Negative control cells, RL-NHL, which express CD20, were also grown and probed with all three antibodies, and these cells were labeled only with the anti-CD20 antibody (data not shown).

Immunofluorescence staining of Colo357 cells with anti-claudin 4, anti-prostate stem cell antigen (PSCA), and anti-CD20 antibodies. A to C represent staining of nonpermeabilized (NP) cells. D to F represent staining of cells permeabilized with 2% paraformaldehyde prior to the addition of primary antibody (340 original magnification for all images). A and D are NP and permeabilized cells, respectively, stained with anti-claudin 4 monoclonal antibody (mAb). B and E are NP and permeabilized cells, respectively, stained with anti-PSCA antibody. C and F are NP and permeabilized cells, respectively, stained with anti-CD20 mAb. The inset in C and F is Hoechst nuclear staining of NP cells.
Rodent Biodistribution in Xenograft-Bearing Mice Shows Moderate Uptake of Anti-Claudin 4 and Anti-PSCA in Colo357 Xenografts and Increased Uptake in PANC-1 Xenografts
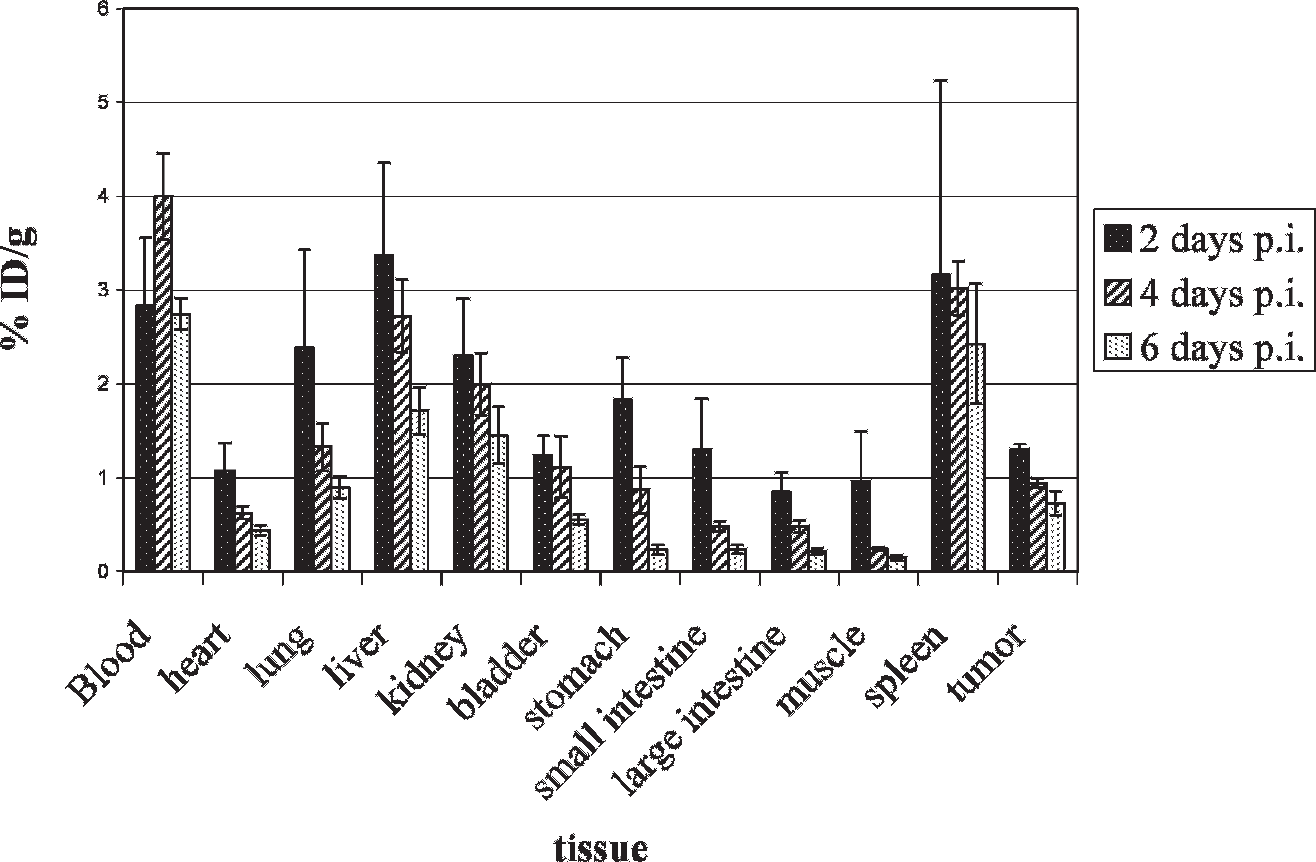
Anti-claudin 4, anti-PSCA, and anti-CD20 antibodies were radiolabeled with 125I, and tracer amounts (2 μCi, 74 Bq, ≈ 80–100 ng) were injected into SCID mice bearing 7 to 10 mm Colo357 subcutaneous xenografts. Equal amounts of anti-claudin 4 and anti-CD20 were also injected into SCID mice bearing 2 to 3 mm PANC-1 subcutaneous xenografts. The mice were sacrificed at 2, 4, and 6 days postinjection and selected organs were harvested. Table 1 lists the % ID/g in all collected tissues for all three labeled antibodies. Most of the nontumor tissues displayed fairly uniform uptake for all three antibodies. Spleen uptake of [125I]anti-CD20, however, was approximately 20% higher than that of either anti-claudin 4 or anti-PSCA. CD20-expressing white blood cells are frequently stored in the spleen. Also, the average uptake of [125I]anti-claudin 4 was slightly higher in the small intestine than for either anti-PSCA or anti-CD20. This is expected since the small intestine is known to express claudin 4. 16 Figure 2 shows a graph of [125I]anti-claudin 4 biodistribution in Colo357 and PANC-1 xenografts. From this graph, it can be seen that the highest uptake for most tissues occurred on day 2 (except for blood and spleen). The liver (4.5% ID/g), spleen (3.7% ID/g), and PANC-1 tumor (4.0% ID/g) displayed the highest uptake values. The liver value represents enterohepatic metabolism of the antibody as liver tissue does not express significant amounts of claudin 4. 9 Spleen uptake reflects antibody sequestration. Tumor to muscle ratios for both Colo357 and PANC-1 xenografts peaked on day 6 (4.3) and day 4 (6.3), respectively. The increased uptake of [125I]anti-claudin 4 in PANC-1 xenografts over Colo357 xenografts is likely due to the smaller, more metabolically active PANC-1 xenograft size (2–4 mm) relative to the Colo357 xenografts (7–10 mm).

Biodistribution of [125I]anti-claudin 4 in Colo357 and PANC-1 xenograft-bearing mice. Severe combined immunodeficient mice harboring either 5 to 7 mm subcutaneous Colo357 xenografts or 2 to 4 mm PANC-1 subcutaneous xenografts were injected with 2 μCi (74 Bq, ≈ 60–100 ng) of [125I]anti-claudin 4 monoclonal antibody and were sacrificed on days 2, 4, and 6 postinjection. Selected tissues were harvested, weighed, and counted in an automated gamma counter. Values shown here represent the percent injected dose per gram (% ID/g) and were done in triplicate or quadruplet. By 6 days postinjection, the Colo357 tumor to muscle ratio had reached approximately 4.3 and the PANC-1 tumor to muscle ratio had reached 6.3 at 4 days postinjection.
Uptake Values for [125I]Anti-Claudin 4, [125I]Anti-Prostate Stem Cell Antigen, and [125I]Anti-CD20 in Colo357 Xenograft-Bearing SCID Mice
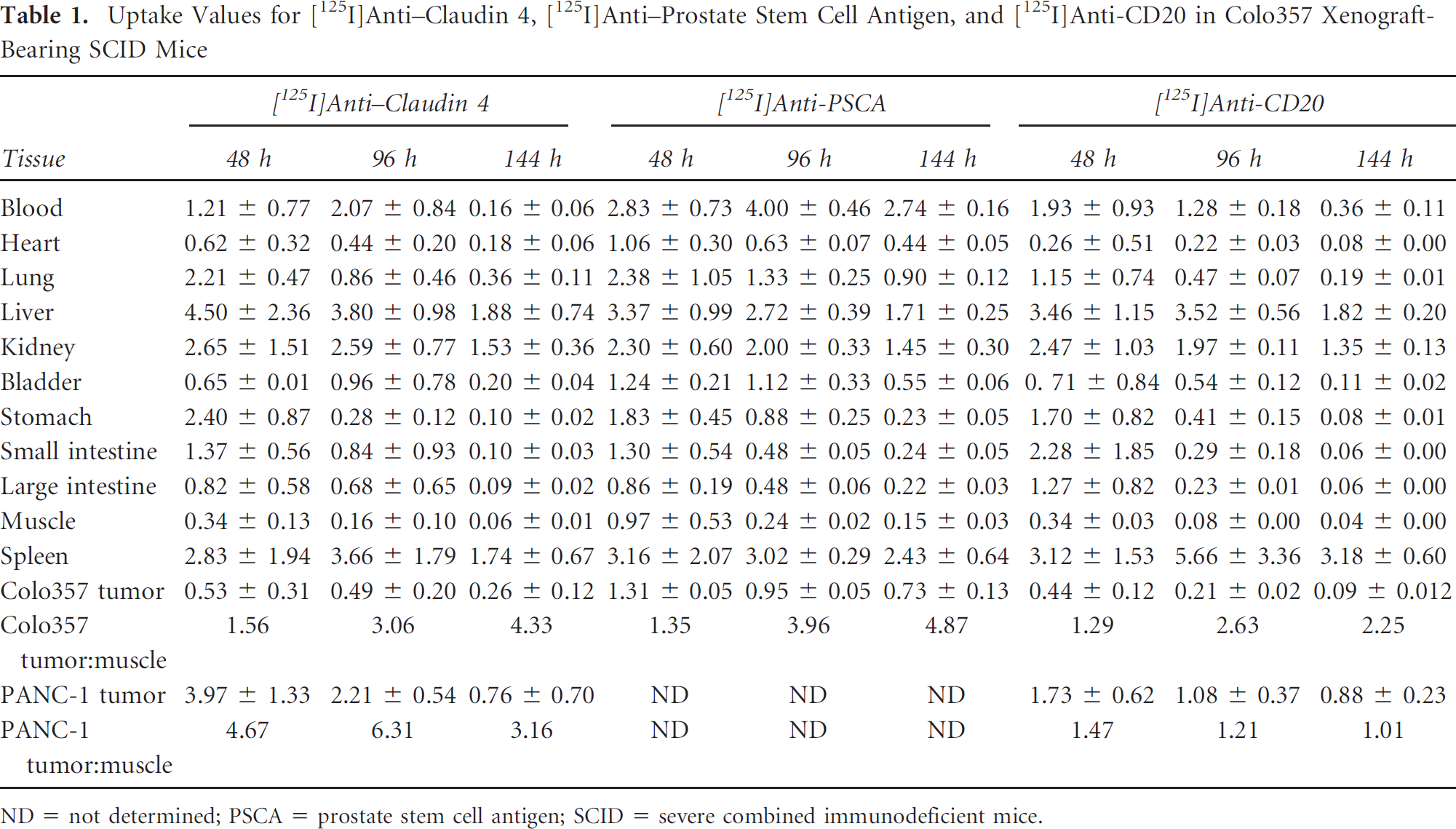
ND = not determined; PSCA = prostate stem cell antigen; SCID = severe combined immunodeficient mice.
Radiolabeled anti-PSCA displayed favorable biodistribution in Colo357 xenograft-bearing mice (Figure 3, Table 1). Aside from the blood values, all other tissue uptake values peaked on day 2. Colo357 tumor uptake peaked at 1.3% ID/g, although the tumor to muscle ratio was highest on day six (4.9). Studies of [125I]anti-PSCA with PANC-1 xenograft models were not possible owing to insufficient availability of this antibody in protein-free buffer (important for radiolabeling).
Biodistribution of [125I]anti-prostate stem cell antigen (PSCA) in Colo357 xenograft-bearing mice. Severe combined immunodeficient mice harboring 5 to 7 mm subcutaneous Colo357 xenografts were injected with 2 μCi (74 Bq, ≈ 60–100 ng) of [125I]anti-PSCA antibody and were sacrificed on days 2, 4, and 6 postinjection. Selected tissues were harvested, weighed, and counted in an automated gamma counter. Values shown here represent the percent injected dose per gram (% ID/g) and were done in triplicate. By 6 days postinjection, the tumor to muscle ratio had reached approximately 4.9.
Biodistribution studies with radiolabeled anti-CD20, a negative control, revealed no specific tumor uptake (< 0.5% ID/g maximal uptake; Figure 4, Table 1), whereas the spleen displayed high uptake (3.1%, 5.7%, and 3.2% ID/g) on days 2, 4, and 6 postinjection, respectively (see Figure 3). Liver and kidneys displayed similar uptake to that observed with radiolabeled anti-claudin 4 and anti-PSCA.

Biodistribution of negative control [125I]anti-CD20 in Colo357 and PANC-1 xenograft-bearing mice. Severe combined immunodeficient mice harboring either 5 to 7 mm subcutaneous Colo357 or 2 to 4 mm PANC-1 xenografts were injected with 2 μCi (74 Bq, ≈ 60–100 ng) of [125I]anti-CD20 and were sacrificed on days 2, 4, and 6 postinjection. Selected tissues were harvested, weighed, and counted in an automated gamma counter. Values shown here represent the percent injected dose per gram (% ID/g) and were done in triplicate. There was no appreciable tumor uptake, whereas the spleen showed the most accumulation of tracer.
Planar Gamma Scintigraphy and SPECT-CT Show Specific Uptake of Anti-Claudin 4 and Anti-PSCA in Colo357 Subcutaneous Xenografts
We undertook planar gamma scintigraphy imaging of Colo357 subcutaneous xenograft-bearing mice with [125I]anti-claudin 4, [125I]anti-PSCA, and a negative control ([125I]anti-CD20) to determine whether the fully intact antibodies, anti-claudin 4 and anti-PSCA, have potential as in vivo imaging agents by delineating tumor location while demonstrating low background radioactivity. Biodistribution studies give quantitative results of tracer uptake but may not show their qualitative utility. Figure 5 shows images of [125I]anti-claudin 4 and [125I]anti-PSCA uptake in xenograft-bearing mice. Panels A to C show [125I]anti-claudin 4 uptake from 2 days postinjection (see Figure 5A) through 6 days postinjection (see Figure 5C). Note the discernable tumor uptake even by day 2. Days 4 and 6 postinjection largely show tumor uptake (yellow arrow, T) with a small amount of liver uptake and thyroid uptake (green arrow, Th) owing to dehalogenase activity and accumulation of free iodine. Thyroid uptake can be reduced or blocked by pretreatment with NaI.

Planar gamma scintigraphy of Colo357 xenograft-bearing mice. Mice were injected with 200 to 300 μCi (7.4–11.1 MBq, 10–15 μg) of [125I]-labeled antibody and were imaged using a Gamma Medica X-SPECT with a single low-energy high-resolution collimator at 2, 4, and 6 days postinjection. A to C show a mouse imaged with [125I]anti-claudin 4 at 2, 4, and 6 days postinjection, respectively. Note that by day 6 postinjection (C), only the tumor (yellow arrow and T) and thyroid (green arrow and Th) are visible. D to F show a mouse imaged with [125I]anti-prostate stem cell antigen (PSCA) at 2, 4, and 6 days postinjection, respectively. By day 6 postinjection, the tumor and thyroid display the highest visible uptake. G to I show a mouse imaged with control antibody [125I]anti-CD20 at 2, 4, and 6 days postinjection, respectively. Note the absence of tumor uptake (yellow arrow and T) and heavy spleen uptake (red arrow and S).
Panels D to F in Figure 5 show uptake of [125I]anti-PSCA in a Colo357 xenograft-bearing mouse at days 2 (see Figure 5D) through 6 (see Figure 5F) postinjection. As with anti-claudin 4, the tumor is clearly visualized at 2 days postinjection, despite apparent liver and thyroid uptake. By 4 days postinjection (see Figure 5E), the tumor uptake is qualitatively nearly equal to the liver uptake, and by 6 days postinjection (see Figure 5F), the tumor uptake appears equally intense as the liver uptake.
[125I]Anti-CD20 was also administered to Colo357 xenograft-bearing animals to test specific binding to the tumor. Panels G to I show heavy spleen uptake with some liver uptake owing to antibody metabolism. There is no observed tumor uptake (yellow arrow and T denote the location of the tumor). [125I]Anti-CD20 was also administered to a SCID mouse bearing a subcutaneous RL-NHL xenograft, which resulted in strong liver uptake on day 2 and mild tumor uptake on day 6 postinjection (data not shown).
Imaging of an orthotopically placed, and thus more clinically relevant, L3.6PL pancreatic cancer xenograft in SCID mice was also undertaken using SPECT-CT with [125I]anti-claudin 4 and [125I]anti-PSCA. These studies were performed using the L3.6PL line, a highly metastatic and aggressive subclone of Colo357, since these cells have been shown to grow reliably in the orthotopic location. 14 As indicated in Figure 6, the panels show transaxial, coronal, and sagittal views of fused SPECT and CT images. At 120 hours postinjection, both the tumor and spleen were clearly visualized in both [125I]anti-claudin 4 and [125I]anti-PSCA images despite the location of the tumor within the pancreas and adjacent to the liver. Following imaging at this time point, the mice were sacrificed and a necropsy was performed to measure directly the radioactivity present in the spleen, tumor, and liver. These measurements indicated that the tumor contained approximately 2.5 times more radioactivity than the spleen and almost twice as much activity as the liver.

SPECT-CT images of [125I]anti-claudin 4 and [125I]anti-prostate stem cell antigen (PSCA) uptake in severe combined immunodeficient mice bearing orthotopic L3.6PL xenografts. The mice were injected intravenously with 148 MBq (4 mCi, 42 μg) of either [125I]anti-claudin 4 or [125I]anti-PSCA in saline 120 hours prior to acquiring these images. Note that the tumor (T) and spleen (S) are clearly visualized even though both are located immediately adjacent to the liver (L).
Discussion
Molecular imaging is an increasingly useful tool for tracking the extent of disease both pre- and post-therapy. The current clinical standard for molecular imaging of pancreatic cancer is PET with [18F]fluorodeoxyglucose (FDG), including studies intended to refine the technique by employing alternative imaging times to enhance the tumor to background ratio.17,18 But FDG has limitations, including nonspecificity, whereupon it may be sequestered within inflammatory and malignant tissues. That is particularly true of pancreatic cancer, where there is often a strong, concurrent inflammatory component. Even lipomas can sometimes be mistaken for a pancreatic neoplasm on FDG-PET. 19 Others have developed peptide-based methods to distinguish pancreatic cancer from pancreatitis, such as those for neurotensin, 20 somatostatin, 21 or bombesin receptors 22 and antibody fragments directed toward MUC-1, a glycoprotein heavily expressed in epithelial cancers, including pancreatic cancer.23,24 Recently, phosphorothioate oligodeoxynucleotide-peptide chimeras have been proposed for imaging pancreatic cancer. 25
Both claudin 4 and PSCA were identified by global expression analysis as up-regulated markers in pancreatic cancer.7,8 Given their membrane localization and the presence of an extracellular domain, these proteins represent attractive candidates for targeted imaging and therapeutic strategies using radionuclide approaches. In fact, the claudin 4 protein, which is also the receptor for the Clostridium perfringens enterotoxin, has already been demonstrated in preclinical studies to be a potential target for pancreatic cancer therapy. 26 Similarly, the PSCA extracellular motif is currently undergoing evaluation as a target for immunotherapy in pancreatic cancers. 27 Thus, both cell surface antigens used by us represent rational choices to explore in the context of pancreatic cancer. The study presented here used 125I to radiolabel all three antibodies. 125I is a low-energy gamma photon emitter that is suitable for imaging small animals with a sensitive gamma camera. However, for use in the clinic, 123I- (SPECT) or 124I- (PET) based radiopharmaceuticals can be used. [123I]anti-claudin 4 and [123I]anti-PSCA are also likely to be useful for identifying sites of metastatic pancreatic cancer spread outside the liver in patients. Detection of nonhepatic metastatic lesions could lead to better treatment stratification, directed metastatectomies, or focused radiation of disseminated disease to improve prognosis. Because biodistribution studies show antibody clearance from all but the liver and spleen by 4 days postinjection, visualization of metastatic lesions outside these tissues should be possible.
For reasons of difficult logistics, that is, for patients to receive first an injection of radiolabeled antibody and then return 2 to 6 days later for SPECT imaging, development of minibodies or diabodies for both anti-claudin 4 and anti-PSCA to achieve faster pharmacokinetics is highly desirable. 28 Typically, radiolabeled minibodies and diabodies reach their target with adequate nontarget tissue clearance at only 2 to 12 hours postinjection.29–31 This would eliminate the need for patients to return to the outpatient facility for a second visit. Diabodies and even triabodies typically exhibit very high tumor uptake compared with intact monoclonal antibodies. 29 Furthermore, targeting claudin 4 and PSCA could also involve pretargeting strategies, such as conjugation of each to streptavidin or the use of biospecific antibodies. The work described herein was, however, merely intended to demonstrate the feasibility of each of these new markers for imaging pancreatic cancer and provides a rationale for adoption of one or more of the aforementioned strategies to improve tumor targeting.