
Abstract
International agencies have advocated scaling-up of midwifery resources as an important method for improving maternal health and reducing maternal mortality rates (MMR). The cost-effectiveness of midwife-led versus physician-led intrapartum care is an important consideration in the human resource planning required to reduce MMR. Studies suggest that midwife-led teams can achieve comparable effectiveness and outcomes using less medically intensive care compared with physician-led teams. In the absence of adequate medical cost data, decision makers should consider the substantially lower average costs for three main drivers: salaries, benefits and incentives (≥two-times lower); preservice training (three-times lower) and attrition (two-times lower) necessary to deliver intrapartum care at the level of midwife competencies. This suggests that scale-up of midwifery resources is a less expensive and more cost-effective way to reduce MMRs and could potentially increase access to skilled intrapartum care.
High maternal mortality rates (MMRs) in many developing countries continue to impede progress toward the United Nations Millennium Development Goal 5 (MDG 5; Improve Maternal Health), including Target 5A, to reduce MMRs 75% from 1990 levels, and Target 5B, to provide universal access to reproductive care. Additional substantial investments in skilled birth attendant training and deployment are needed in developing countries in order to improve access to reproductive health and to reduce MMRs. Many developing countries suffer from severe shortages in skilled healthcare workers in part because of limited financial resources, misguided strategies focused on low-skilled professionals or trained birth attendants, pressures to reduce public sector expenditures, previous insufficient investment in training, high attrition rates, population growth and maldistribution of human resources. A strategy that developing countries are implementing to address this human resource gap involves moving along the continuum of maternal and neonatal care from a higher cadre of healthcare workers (i.e., physicians) toward a lower cadre of workers (e.g., midwives and trained birthing assistants) [1]. However, the use of lower levels of healthcare workers without supervision or defined career paths has raised concerns regarding quality of care [2,3].
Skilled birth attendant has been defined by the WHO, International Confederation of Midwives and International Federation of Gynaecologists and Obstetricians as: “An accredited health professional – such as a midwife, doctor or nurse – who has been educated and trained to proficiency in the skills needed to manage normal (uncomplicated) pregnancies, childbirth and the immediate postnatal period and in the identification, management and referral of complications in women and newborns” [4]. Over the past 25 years, international agencies have called for an intensive scale-up of skilled birth attendants, particularly trained midwives, to reduce maternal mortality, increase access to reproductive health and support a woman's right to quality care [5].
The midwife (or equivalent) is a member of the chain of professionals, necessary for maternal health ranging from community to referral services, and is an important part of the solution. Compared with physicians, midwives can be trained faster and at lower cost, have lower salaries and have higher retention rates. These factors suggest that scale-up of midwifery resources is a cost-effective way to increase rates of skilled birth attendance and reduce MMRs [6]; however, data on the cost–effectiveness of midwife-led versus physician-led care in developing countries are mainly lacking.
This paper contributes to the literature by recommending an economic framework for policy makers in developing countries to inform their investments in skilled birth attendants and by evaluating published evidence on the effectiveness and cost–effectiveness of midwife-led versus physician-led intrapartum care.
Background
Every year, nearly 300,000 women die in childbirth and millions more suffer from a serious pregnancy-related illness or disability following birth [6–8]. Lack of access to skilled birth attendance and emergency obstetric care (EMOC) by the poorest populations is largely responsible for high maternal death and disability rates [7,8].
The link between increased access to skilled birth attendance and reduced MMR has been well established. Global efforts to scale-up skilled birth attendance are focused on reducing maternal death and more generally on supporting countries to achieve MDG 5A and 5B targets. By providing family planning services, high-quality basic EMOC and timely referrals to facilities with physician-supervised comprehensive EMOC capabilities, midwives and other skilled birth attendants with midwifery competencies can prevent most maternal deaths and disabilities resulting from obstetric hemorrhage, infection, eclampsia, prolonged/obstructed labor, and puerperal sepsis, assuming the availability of adequate supplies and equipment and a referral infrastructure [3–4,9–12]. Here we are invoking the definitions that basic EMOC encompasses parenteral administration of antibiotics, oxytocics and anticonvulsants; assisted vaginal delivery; manual removal of the placenta and removal of retained products while comprehensive EMOC expands on those skills to also include caesarean birth, blood transfusion and maternal and neonatal resuscitation [7].
To increase skilled birth attendance, developing countries must address human resources for health management, including training, recruitment, deployment and retention, which will all influence the in-flow and out-flow of workers. Developing countries with the poorest health indicators need to achieve appropriate coverage of facilities and have the minimum package of activities and the minimum required human resources for health for each level of the health system. These countries are also those affected by the most severe shortages of qualified healthcare workers [13]. In 57 countries, health workforce shortages have been deemed critical (i.e., <2.3 health workers/1000 population) and are disproportionately severe in rural and remote areas [14]. Major causes of shortages include a lack of previous investment in preservice training, attrition of healthcare workers [15,16], a lack of preservice training capacity, an insufficient supply of qualified students to enter preservice training, maldistribution of healthcare workers and consequent inequities in access to care and rapid population growth. By one set of estimates, an additional 550,000 midwives and nurses and 240,000 physicians will be needed to fulfill the growing healthcare needs in 31 African countries, necessitating investments of US$1.5 billion and US$1.1 billion (2007 US$), respectively [1].
The situation in urban areas of lower income countries and in middle income countries differs from that of the poorest, rural areas. In this situation, the existing number of healthcare workers and funds for training more healthcare workers may be sufficient, but there may be problems of maldistribution. As countries grow richer, there is a tendency to deploy physicians to more districts. Studies suggest that growth in physician-led intrapartum care may be associated with over-medicalization, specifically a disproportionate increase in rates of caesarean birth [17,18]. Decisions regarding investments in human resources in each country must consider how best to achieve the appropriate balance between midwives and physicians for optimal and cost-effective results.
Current data on the effectiveness & costs of midwife-led versus physician-led intrapartum care
Generally speaking, cost–effectiveness analysis compares the incremental difference in costs to the incremental difference in effectiveness [19]. Cost–effectiveness frameworks inform evidence-based policymaking focused on efficient health resource investment decisions regarding how to achieve the best health outcomes for a given set of possible investments.
Assessing the cost–effectiveness of scaling up midwife-led versus physician-led intrapartum care depends on the availability of accurate, high-quality data. In developing countries, data from experimentally designed studies are largely lacking. The results of one study from Nepal [20] showed that midwife-led intrapartum care was less resource intensive, less costly and as safe and effective as physician-led intrapartum care (Table 1). This study compared intrapartum care received by two similar groups of pregnant women at low obstetrical risk in midwife-led (n = 550) versus physician-led units (n = 438). Compared with women receiving physician-led care, women who delivered in the midwifery unit were significantly less likely to have an episiotomy (36% likelihood), undergo caesarean birth (63%) or receive oxytocics to augment labor (74% reduction); there was also a trend toward shorter hospitalization compared with women who delivered in the consultant-led maternity unit. No significant differences in neonatal or maternal mortality were observed between the groups.
Although the context differs markedly in developing and developed countries, the results from the study in Nepal are consistent with those of several randomized and other well-designed prospective and retrospective studies conducted in developed countries
Midwife-led versus physician-led models of intrapartum care in low risk women in Nepal: selected procedure outcomes and resource use.

LOS: Length of stay; NS: Not significant; RR: Relative risk.
Midwife-led versus physician-led models of intrapartum care in low-risk women: selected procedure outcomes.

Physician-led comparisons subgrouped by obstetricians and family practitioners.
FP: Family practitioner; NA: Not available; NS: Not significant; OB-GYN: Obstetrician-gynecologist; OR: Odds ratio; RR: Relative risk.
Midwife-led versus physician-led models of intrapartum care in low-risk women: hospitalization length of stay and economic outcomes.

Covers costs of maternal care 300 days antepartum and 180 days postpartum.
LOS: Length of stay; NA: Not available; NS: Not significant.
An alternative cost–effectiveness model of midwife-led versus physician-led intrapartum care for developing countries
Because quality data are scarce, it is not possible to construct accurate cost–effectiveness models based on maternal mortality rates, neonatal mortality rates, complication rates and birthing resource costs to compare midwife-led to physician-led programs in developing countries.
An alternative approach to assessing cost–effectiveness in developing countries could be to evaluate differences in cost drivers (including salary, benefits, incentives, preservice training, in-service training, attrition, administration and monitoring and evaluation) and compare them to expected differences in effectiveness measured by outcome measures, such as maternal deaths, newborn deaths or complications averted (
Based on simulations using the OneHealth Tool [34], the programmatic components for which differences in costs between physician- and midwife-led intrapartum care are expected to be greatest include salary (including related benefits and incentives), preservice training and attrition rates. As explained below, it is anticipated that midwife-led intrapartum care will have lower costs than physician-led care, driven primarily by salaries, benefits and incentives on average being one half or less that of physician-led care, preservice training costs one-third that of physician-led care and midwife attrition being roughly half that of physician attrition rates. Differences associated with in-service training and administrative costs were not anticipated to be major drivers of the cost differences between midwife-led and physician-led care.
Relative effectiveness & safety
Within the set of competencies common to midwives and physicians, the evidence from industrialized nations indicates that the effectiveness and safety of intrapartum care provided by both types of healthcare professionals are comparable [21–24, 26–30]. Because of the lack of experimentally designed comparative studies of effectiveness between midwife-led and physician-led care in developing countries, we have used the results of comparative studies in developed countries (described previously) to conclude that there are no obvious differences in effectiveness between midwife-led and physician-led care. The sample size of these studies was insufficient to allow for comparisons of maternal mortality. In general, the tendency for midwife-led care to be significantly less medically intensive (
Relative salary
Salaries and incentives are estimated to comprise approximately 16% of the incremental costs of scaling up the health system for all cadres of health workers according to the High-Level Taskforce on Innovative Financing for Health Systems [35]. According to the WHO CHOICE salary database, the salary for a physician or medical specialist is generally at least twice that of a salary for a nurse/midwife (
Relative cost of training
Preservice training is estimated to account for approximately 8% of the incremental costs of scaling up the health system for all cadres of health workers according to the High-Level Taskforce on Innovative Financing for Health Systems [31]. Training costs include recurrent costs such as tuition, room and board and supplies, as well as capital costs relating to the construction or rehabilitation of educational facilities and installation of major equipment. In the High Level Task Force in Innovative Financing (2010) and the World Health Report [35,36], the WHO assumed that the total preservice education costs were a multiplicative factor of the gross domestic product per capita, where the estimated cost of a midwife's preservice training was about a third the cost of a physician's preservice training. This relative cost is a reflection of the shorter time period for midwifery training and the narrower focus of midwifery training (routine birthing care and basic EMOC) relative to physician training [37]. Additionally, several countries are considering or are in the process of shifting the training of nurse/midwives, which requires 7 or 8 years, to the training of midwives, which requires 3 years, to enhance cost–effectiveness.
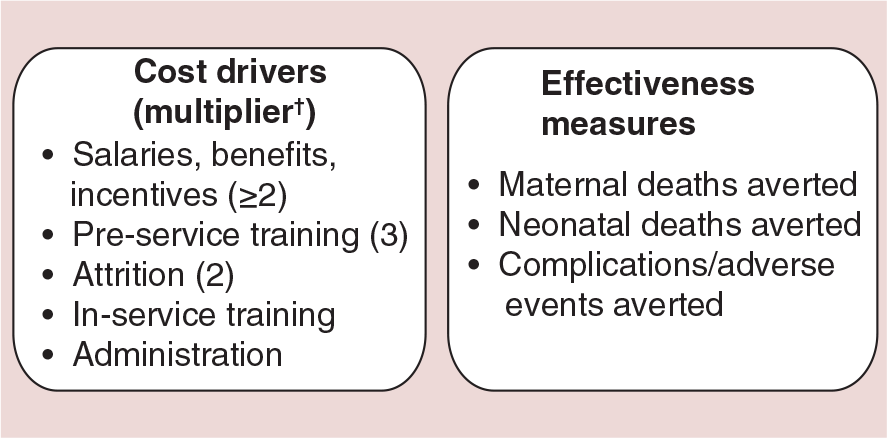
Proposed cost–effectiveness model for midwife-led versus physician-led intrapartum care in developing countries.
Another potential source of cost differential between midwives and physicians arises from the need for new school construction or expansion. The construction of new training facilities is likely to be required if the preservice training needs vastly exceed the current production capacity. The International Finance Corporation estimated start-up costs range from US$2 to US$10 million for a large, multidisciplinary medical university compared with US$0.3 to US$2 million for a school for nurses, midwives and laboratory technicians [32].
Relative attrition rate
Attrition of healthcare workers is a major factor impeding the ability of many developing countries to scale-up skilled birth attendant coverage [13]. Attrition disproportionately affects rural and remote areas, contributing to high MMR burden [38]. The costs of attrition encompass not only loss of time, productivity and customers, but also workforce replenishment. Causes of attrition fall into two categories: voluntary and involuntary. Voluntary attrition may be related to low pay, poor working and living conditions, high work load/stress level or fear of contracting a serious illness such as HIV/AIDS [39], as well as migration opportunities. Involuntary attrition is associated with factors such as serious illness, dismissal, death and retirement [13,33,38], and is a relatively minor contributor to the overall causes of attrition. The attrition rate of midwives tends to be lower than that of doctors. For example, in 2008, the Zambia Ministry of Health estimated that the baseline estimate of total attrition for midwives was 4.5%, less than half of the 9.8% baseline estimate of total attrition for doctors [38]. Similarly, in 2006, the attrition rate for nurses and midwives in Nigeria was 1.4% or nearly half of the 2.3% attrition rate for doctors [40]. Other simulation-based estimates also support the contention that attrition rates are higher for physicians than midwives [13]. For all cadres of healthcare workers, it is critical that human resource strategies are implemented to minimize attrition through retention programs, especially in rural and remote areas where job satisfaction may be an acute concern. Additionally, human resource strategies are necessary to ensure service quality through appropriate monitoring, supervisory visits, in-service training and accreditation programs.
Discussion
There is an urgent need for substantial investment in midwifery training and deployment in developing countries to reduce maternal mortality and enable universal access to sexual and reproductive health. Skilled birthing care provided by midwives is perceived to be a cost-effective alternative to birthing care provided by physicians; however, this perception is not well supported with evidence. Policymakers in developing countries need evidence-based tools to invest scarce resources efficiently.
Few formal cost–effectiveness studies of midwife-led versus physician-led intrapartum care have been published. Studies of caesarean births performed by assistant medical officers and obstetrician/gynecologists in Mozambique and other African nations have shown comparable maternal outcomes for both cadres and greater cost–effectiveness for the assistant medical officers [41–43]. For midwives, a substantial amount of high-quality evidence from developed countries shows that with proper training, adequate resources and a quality infrastructure, midwife-led intrapartum care results in similar safety and effectiveness outcomes with fewer resources and lower costs compared with physician-led intrapartum care. At least one large study from Nepal has shown similar results [20], but more evidence on the cost–effectiveness of midwife-led care in developing countries is needed that account for country, region and intraregional and equitable variations in population risk profiles, healthcare resources and infrastructure. Conversely, the consistency of data showing more intensive medical resource utilization by physicians shown in these studies is reflected in studies in developing countries that have shown rapidly increasing rates of caesarean birth without clear evidence that this is related to either medical need or maternal preference [17,18].

Salaries for medical specialists were higher than nurse/midwives in sample countries (2005 US$).
In the absence of accurate data on costs and effectiveness of care in developing countries, an alternative model of cost–effectiveness based on programmatic components and various measures of effectiveness is recommended for use by policymakers in those countries. This cost approach combines the cost drivers of midwife- and physician-based programs, including salaries, preservice training and attrition, and effectiveness indicators.
Implementation of the alternative model with simulated data on training, attrition and salaries from developing countries (using the OneHealth tool) indicates that, for many developing countries, scaling up midwife-based programs is expected to be more than twice as cost effective as scaling up physician-based programs, under assumptions of reasonably comparable effectiveness. Even more favorable cost–effectiveness ratios are attainable if reductions in the intensity of medical resource use resulted from midwife-led care. The substantially lower costs associated with midwives also suggest that even at lower effectiveness, midwife-led intrapartum care may still be more cost effective.
Research exploring the effectiveness outcomes in urban, rural and remote settings of care and in different subpopulations is warranted. Most effectiveness data collected in studies have been derived from low-risk pregnancies and cannot readily be extrapolated to higher-risk pregnancies. Development of data from diverse settings and subgroups would best inform where midwifery care is most effective and who benefits the most in developing countries.
The cost-effective scale-up of professionally trained midwives is a critical step toward breaking the stagnation in workforce shortages and persisting high MMRs. However, this effort can only be successful in the context of: implementing strategies to encourage midwives to work and live in rural and remote areas; complementary efforts to ensure quality of intrapartum care at all levels, whether that care is provided within a facility or a home [3]; an infrastructure that includes secondary and tertiary health facilities, adequate supplies and equipment, effective communication and referral/transport systems; and as part of a comprehensive human resources approach. These systems of care are found in countries that have been able to achieve low MMRs [44] such as China, Malaysia, Sri Lanka and Mexico.
Irrespective of whether the intrapartum care is midwife-led or physician-led, effective health system infrastructure is necessary to reduce maternal mortality. For example, in situations where comprehensive EMOC is required, an effective referral and transport system must be in place with the required communications, transportation, human resources, training and supervision elements established. The successful patient referral and transport would be to a higher level facility that is appropriately supplied with necessary items for performing comprehensive EMOC including electricity, sterile operating environment, anesthesia equipment, surgical instruments and supplies, neonatal resuscitation equipment, laboratory capabilities and the capacity for delivering blood transfusion. The establishment of a health system that can support the referral, transport and the appropriately supplied facility to support comprehensive EMOC requires substantial financial and time investments, a challenge in many developing countries.
The ability of midwives to succeed and remain in their jobs also depends on an enabling environment. Compared with solo practitioner models, studies suggest facility-centered models of care in combination with team-oriented midwifery care (in which midwives work with midwife assistants and other health providers) is a viable and more sustainable approach to meeting the need for basic and comprehensive EMOC, supportive working environments, sustained high-level quality of care, increased skilled delivery coverage, maintenance of clinical skills and improved retention of midwives in rural/remote areas [2,37,45–46]. Simulations indicate that this team-oriented approach could be scaled up much more quickly compared with deployment of solo health workers to increase skilled intrapartum coverage and accelerate reduction in MMRs [36,47].
The conclusion that midwife-led services are a cost-effective solution for reducing maternal mortality agrees with recently published simulations examining effectiveness and cost–effectiveness. Investments in sexual and reproductive health services, including scaling up of midwifery services, have been shown to be highly cost effective with rates of return of up to nine-times the economic and social benefit [48]. In countries in the lower tercile of the Human Development Index, universal coverage (95%) of the interventions delivered by midwifery services was projected to reduce maternal mortality by 82% with similar projected declines in neonatal mortality and stillbirths [49].
Conclusion
An alternative approach to evaluating investments in midwife-led versus physician-led intrapartum programs suggests that scale-up of midwifery resources by developing countries is a much less expensive and more cost-effective way to reduce MMRs based on its lower costs and similar effectiveness, and also a potentially more rapid way to increase access to skilled intrapartum care. Optimism about continuing the reduction in maternal mortality depends on adequate investment levels in midwifery and related resources.
Future perspective
In the near future, we anticipate that cost–effectiveness analysis will continue to be an increasingly important component of the health system planning cycle. As such, there will likely be more comparative cost–effectiveness studies related to the use of midwives-led versus physician-led intrapartum care in developing countries. Enhanced simulations associated with scaling up skilled birth coverage will be developed in the future where the complete health system implications (including all components of human resource planning, infrastructure development, equipment, logistics, governance, health information systems and health financing) will be fully incorporated. This simulation research will be important to inform strategies that can lead to the effective and efficient scale up of midwife-based birth coverage. As human resource challenges continue to present themselves in resource-cons trained environments, there will probably be a greater emphasis on the use of midwives for the provision of skilled birth attendance along with the necessary training, governance, supervision, referral systems and infrastructure to ensure safe delivery for mother and newborn. The result of these investments will be a continuation in the reduction of maternal and neonatal mortality rates.
Executive summary
Every year, nearly 300,000 women die in childbirth and millions more suffer from a serious pregnancy-related illness or disability following birth. Additional substantial investments in skilled birth attendant training and deployment are needed to improve access to reproductive health and reduce maternal mortality.
Many developing countries suffer from severe shortages in skilled healthcare workers in part because of limited financial resources, misguided strategies focused on low-skilled professionals or trained birth attendants, pressures to reduce public sector expenditures, previous insufficient investment in training, high attrition rates, population growth and maldistribution of human resources.
The cost–effectiveness of midwife-led versus physician-led intrapartum care can be assessed by evaluating differences in cost drivers (including salary, benefits, incentives, preservice training, in-service training, attrition, administration, and monitoring and evaluation) and comparing them to expected differences in effectiveness measured by outcome measures, such as maternal deaths, newborn deaths or complications averted.
Based on simulations using the OneHealth Tool, scaling up midwife-based programs is expected to be more than twice as cost effective as scaling up physician-based programs, under assumptions of reasonably comparable effectiveness.
Randomized and other well-designed prospective and retrospective studies have demonstrated comparable clinical outcomes for midwife-led and physician-led intrapartum care, even though midwife-led care is significantly less medically intensive (e.g., fewer caesarean births, episiotomies).
The salary for a physician or medical specialist is generally at least twice that of a salary for a nurse/midwife. In OneHealth Tool simulations comparing the costs of scaling up of physician versus midwife cadres, the ≥2-fold salary difference between midwives and physicians was the primary driver of cost differences. If benefits and incentive pay are adjusted to relocate health workers to remote areas and help alleviate the maldistribution of resources among urban and rural areas, then the compensation difference becomes even larger (as benefits and incentive pay are often proportional to the base salary).
The estimated cost of a midwife's preservice training was about one-third the cost of a physician's preservice training, a reflection of the shorter time period for midwifery training and the narrower focus of midwifery training (routine birthing care and basic EMOC) relative to physician training. In-service training costs were not anticipated to be a major driver of the cost differences between midwife-led and physician-led care.
Attrition rates are generally higher for physicians than midwives.
The cost-effective scale-up of professionally trained midwives is a critical step toward breaking the stagnation in workforce shortages and persisting high MMRs. Scaling-up of midwifery services can only be successful in the context of: implementing strategies to encourage midwives to work and live in rural and remote areas; complementary efforts to ensure quality of intrapartum care at all levels, whether that care is provided within a facility or a home; an infrastructure that includes secondary and tertiary health facilities, adequate supplies and equipment, effective communication and referral/transport systems; and as part of a comprehensive human resources approach. These systems of care are found in countries that have been able to achieve low maternal mortality ratios.
Author contributions
H Friedman and M Liang conceived the paper. H Friedman, J Banks and M Liang conducted the research. H Friedman and J Banks analyzed the data. H Friedman and J Banks wrote the paper. H Friedman, J Banks and M Liang provided interpretation of analysis, comments and writing of paper.
Footnotes
Acknowledgements
The authors thank Sennen Hounton, Luc de Bernis and Jacqueline Mahon of the United Nations Population Fund (UNFPA) for their helpful comments.
This work was supported by the United Nations Population Fund (UNFPA, NY, USA). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
The authors thank Complete Publication Solutions, LLC, for their editorial assistance, which was funded by the UNFPA.