
Abstract
This review focuses on drug use during pregnancy and the perinatal period, a constellation that is seen more often. Drug use in pregnant women poses an increased risk for adverse health outcomes both for the mother and child. Care is often complicated by social and environmental factors, as well as psychiatric comorbidities. It is, therefore, very important to provide drug-using pregnant women with optimal ante-, peri- and post-natal care. Health professionals should approach them in a nonjudgmental and supportive way, and provide them with the same care and attention as nondrug-using women. Adequate care requires interdisciplinary teams. Ideally, healthcare providers should be specialized in the care of drug-using pregnant women.
Since the 1980s, an increase of drug use in women of childbearing age has been observed [1–7]. The exact number of drug-dependent women is unknown because epidemiological data rely almost exclusively on voluntary patient reports [1,8]. The causes of drug use are likely to be multifactorial including biological, psychological, as well as social factors. The care of drug-using women during pregnancy is challenging, as the mother's and infant's health might be compromised, and this has to be considered. Furthermore, it is not only the drug itself that harms the pregnant woman and the fetus, but these women may live in difficult social circumstances, and psychiatric comorbidity is frequent. Evidence-based standards of care would thus be beneficial. This review aims to provide an overview of the current literature findings considering PubMed listed papers primarily within the time period of 1983–2013. In addition, an established interdisciplinary model of care implemented at a university women's hospital in Switzerland will be presented and discussed.
Vrious effects of drugs in the context of reproduction
Drug use & fertility
Impaired fertility associated with heroin use has been previously demonstrated [9], both in men and women [10,11]. Even low doses of narcotics can impair normal ovarian function and ovulation and therefore reduces the probability of conception. Interestingly, in a longitudinal study on 191 heroin- and cocaine-addicted women, among whom less than a third had a regular cycle, Schmittner et al. demonstrated that the menstrual bleeding pattern began to normalize during methadone maintenance [12]. Even if this was just one of few studies, it leads to the hypothesis that the stability of methadone maintenance might interfere less with menstrual function than illicit heroin use. Improved fertility, in addition to better medical care as a result of substitution programs, might be possible explanations for the increase in drug-using pregnant women around the turn of the millennium [12].
Drug effects on mother & child
Substance abuse not only harms the patient herself but also the unborn child [13]. Table 1 shows a summary of the effects of different substances on mother and child.
Drug effects on the mother and child.
FAS: Fetal alcohol syndrome; FASD: Fetal alcohol spectrum disorders; IUGR: Intrauterine growth retardation; SGA: Small-for-gestational age; SIDS: Sudden infant death syndrome; THC: Tetrahydrocannabinol.
Data taken from [27].
Problems include preterm labor and low birth weight in general [1,27], and special complications, such as myocardial infarction, cerebrovascular accidents and placental abruption, in cocaine-using women owing to the vasoconstrictive effects of the drug [28]. However, the effects of in utero cocaine exposure are also correlated with other factors, such as prenatal exposure to tobacco use, other drugs and the environment [29]. Examining direct effects of specific drugs is, therefore, challenging since most of the women are poly-drug users [30,31]. The fact that the effects on mother and child are likely to be multifactorial complicates care even more [32–34]. Factors, such as smoking, poor diet, stress and chaotic lifestyle, appear to be the most important etiological factors. Outcomes associated with drug use are, therefore, results of either the effect of the drug itself or of problems related to growth restriction and/or premature delivery. Furthermore, there is a paucity of research regarding newer drugs such as ecstasy, bath salts or synthetic cannabinoids [1,30,35].
In a study on 247 drug-using women and 741 controls conducted over a 4-year period, drug-using women were still at significant risk of adverse obstetric and perinatal outcomes, with significantly more preterm births, a higher incidence of low birth weight and intrauterine growth restriction despite coordinated prenatal care. The risk of placental abruption was also higher [36].
The proportion of pregnant women who continue to drink alcohol in pregnancy is noteworthy [37,38]. A large, recent prospective, multicenter cohort study on healthy nulliparous females with singleton pregnancies, with the main aim of developing screening tests to predict adverse outcomes, such as preeclampsia, small gestational age neonates and spontaneous preterm birth, did not demonstrate a strong association between (occasional to heavy amounts of) alcohol consumption in early pregnancy and these outcomes. However, these effects are likely not only dependent on quantity consumed, but also on the timing of exposure. It is also noteworthy, that this study did not investigate the association between alcohol consumption in pregnancy and long-term neurocognitive outcomes of children with fetal exposure to alcohol [39]. Therefore, the authors of this review believe that there is not enough evidence to suggest that any amount of alcohol is safe during pregnancy.
Complex psychosocial situation & lack of prenatal care
Drug and alcohol use, and the resulting problems mostly precede pregnancy. Likewise, comorbidity can either be a cause or consequence of drug use. Drug-using women's reproductive health is affected by many factors, such as poor social environment, malnutrition, inadequate hygiene, sexually transmitted infections, physical abuse or a history of prostitution [40–43].
It is known that the lack of antenatal care is associated with worse outcomes for mother and child [36]. In a retrospective study on 211 women who came to delivery without any antenatal care, drug abuse was the most prevalent reason for this behavior [44]. Furthermore, in a postpartum cohort of 812 low-income women who delivered at a tertiary care center, cocaine or opiate abuse was predictive of little or no antenatal care [45].
Drug-using pregnant women may not use (and may not have access to) the traditional maternity services the same way nondrug-using women do. They tend to present late, have difficulties in attending appointments, and when they present, they might not admit their drug use [46]. Possibly owing to fear of stigmatization or legal consequences, drug-using or alcoholic pregnant, or postpartum women often deny their drug habit, the possible harmful effects and the need to seek appropriate care and, therefore, often receive no care at all [32,47].
Psychiatric comorbidity
Clinicians should be aware of psychiatric comorbidities in the population of drug-using women [13,31,48], and both psychiatric comorbidities and the patient's habit of consuming drugs have to be approached [49]. According to an Australian population-based, retrospective study, depression is the most common psychiatric disorder followed by anxiety disorders. Almost half of all drug-using mothers were affected by depression [50]. These mothers had more previous pregnancies and suffered more often from domestic violence. Since prenatal care and social outcome may be worse for these mothers and their children, the authors recommend that all pregnant drug-using women should be assessed for psychosocial disorders in order to facilitate timely interventions [50].
Pregnancy care for drug-using women
Pregnancy
Even if the risk of each pregnancy of a drug-using woman has to be assessed on an individual basis, some of these pregnancies need to be considered as potential high-risk pregnancies, and thus, specialized (obstetrical) interdisciplinary teams should engage in their care [31,48].
An aspect that might be neglected when assessing drug-using women are concomitant factors, such as cigarette smoking, alcohol use and poor social circumstances, which are all common in women using illicit drugs [32]. In a case–control study on 370 full-term gestations, the three main risk factors for fetal growth retardation were tobacco, low prepregnancy weight and low socioeconomic status [51]. Most pregnant women using cocaine and/or heroin appear to be cigarette smokers. In general, babies whose mothers smoked during pregnancy tend to have lower birth weights; an effect that appears to be dose-dependent with a higher number of cigarettes per day related to lower birth weight [52].
It is important to use a consistent, easy-to-use screening tool and a nonjudgmental approach to evaluate patients for possible drug use. There is controversy regarding whether screening should be undertaken systematically in all pregnant women or just in selected patients suspected of drug abuse [53]. The American Congress of Obstetricians and Gynecologists suggest easily applicable screening tests in the form of questionnaires [34,54]. In our institution (University Hospital Basel, Switzerland), screening by means of urine drug tests is performed repeatedly – provided the patient consents – when clinically indicated. Furthermore, fetal exposure to illicit drugs or alcohol in utero can be detected by meconium analysis, reflecting exposure during the second and third trimester, by means of chromatographic techniques [55–57].
Interdisciplinary approach to care
Neonatal outcomes may be positively influenced as shown in an interventional study on a large sample of 6774 pregnant women. Rates of assisted ventilation, low birth weight and preterm delivery improved when mothers received substance abuse treatment integrated with prenatal care [58]. Nowadays, most studies suggest that drug-using pregnant women are in need of multidisciplinary antenatal care with medical, social and psychological support [59–61]. Comprehensive, interdisciplinary treatment programs are likely to have a positive impact on outcomes [62–67]. The one retrospective study that failed to demonstrate a positive effect was not designed to show an effect of an interdisciplinary approach. Furthermore, no detailed information on the type of interdisciplinary teamwork is provided [36].
To optimize the ante- and post-natal care for mother and child, an interdisciplinary team, including an obstetrician–gynecologist coordinating the involved special services, should be developed. As shown in Figure 1, one health professional should be designated as the case manager. In our institution, this is a gynecologist and member of our division of social and psychosomatic gynecology. This specialized service is possible, as we are a tertiary care university hospital serving a population of approximately 300,000 people. This service is well accepted and used. Most of the patients are referred by their primary-care providers, in addition to drop-ins at the moment of delivery. Divergent from the regular antenatal-care patients, they are seen more frequently – at most every 2–4 weeks.
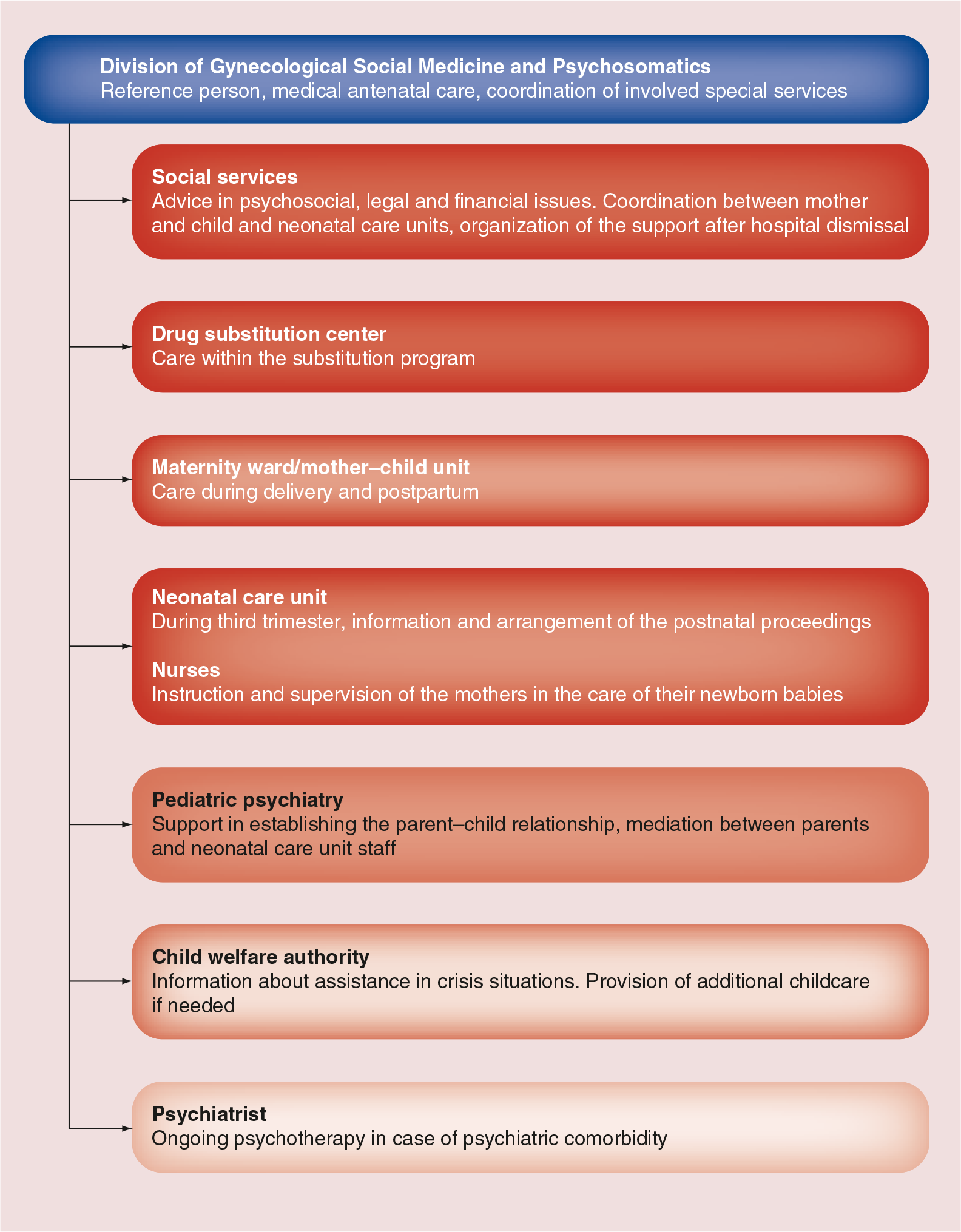
The Basel model of interdisciplinary care of drug-using women.
Depending on the individual situation and needs for care, disciplines, such as drug-substitution centers, social workers, neonatologists, psychiatrists, pediatric psychiatrists, family physicians and child welfare authorities, should be involved. In our setting, it is the obstetrician–gynecologist who serves as the primary reference point for the patient and takes the lead in the interdisciplinary team, by coordinating and integrating the disciplines that are needed. This process needs to be as easy and comfortable for the patient as possible since compliance is an issue.
Women who present with a history suggestive of drug use, should receive the same care as women who do not use drugs, including determination of gestational age by ultrasound; keeping in mind that the population of drug-using women is often underserved. It is advantageous to diagnose pregnancy as timely as possible. To identify women at risk who present in the antenatal phase, the gynecologist has to take the history of past and present drug use, including necessary details, such as participation in substitution programs or intravenous application of drugs. Co-ordination and management of the substitution should be performed by the substitution center. In addition, testing for sexually transmitted diseases and hepatitis C should be undertaken, when considering that, according to a recent study, 41% of drug-using women had evidence of previous exposure to the hepatitis C virus [68].
In our institution, a round table is established during the third trimester, at which the involved disciplines plan postnatal care. This serves as an information platform for the teams, and also establishes contact between the ante- and post-natal caretakers and the patient, in order to address their issues and concerns. In this context, the neonatologists have the opportunity to inform the patient about postnatal substitution.
Admission & delivery
At presentation, for example, admission for delivery, midwives and obstetricians need to be aware of unusual behavior or agitation. Furthermore, physiological signs of drug abuse, such as dilated or constricted pupils, increased or decreased respirations, bradycardia or tachycardia, hypotension or hypertension, all depending on the substance used, should be registered [8]. These can be both signs of intoxication and withdrawal, and should prompt further testing to confirm drug use and rule out preeclampsia. These symptoms might be harmful for both the mother and child [69]. As substance use and smoking are associated with an increased risk of placental insufficiency, growth restriction and possible fetal distress, monitoring has to be especially thorough; during pregnancy with regular ultrasounds and during labor by continuous heart beat monitoring [32]. Neonatal care should be readily available in the maternity ward. Postnatal care needs to be adjusted to the needs of the patient, for example, withdrawal signs or other necessary treatments for the newborn [46,70].
Breastfeeding
Breastfeeding is beneficial in a number of ways. Apart from its short- and long-term medical and neurodevelopmental benefits [71], it helps bonding between mother and child, which is particularly important when the mother is using drugs. Nevertheless, only approximately 15% of patients were still breastfeeding at discharge in a study from the UK [72].
In methadone-substituted women with no parallel consumption of other drugs, breast-feeding is not contraindicated. However, in a study with small group sizes, fewer infants in the breast-fed group required pharmacotherapy for neonatal abstinence syndrome, an effect that was not statistically significant. Interestingly, this study showed low concentrations of methadone in breast milk, which were not related to maternal intake, supporting the recommendation for breastfeeding among methadone-maintained women [73]. The effect of breastfeeding on severity of neonatal withdrawal symptoms has also been reported elsewhere [46,74]. As children of drug-using women are often delivered preterm or are small-for-gestational age, breastfeeding is particularly useful [75]. Breastfeeding should, therefore, be encouraged in methadone-substituted women [76,77]. Data on breastfeeding are less clear with regard to other drugs, such as cocaine and heroin [78,79], and are often based on case reports or – series [76]. With regard to cocaine, it is crucial for the healthcare provider to counsel patients both on the serious potential risks of cocaine exposure (e.g., potential agitation, irritability, seizures, hypertension and tachycardia), and on the advantages of breastfeeding, to allow for an informed choice [80]. Both cocaine and marijuana are soluble and can potentially become trapped in the breast milk [76]. For cannabis exposure through milk, no increase in neonatal risk has been shown; however, there are no appropriate studies on this, to date [81–83]. Some authors discourage breastfeeding in mothers who regularly use marijuana [76]. Occasional users who are not able to stop, should be evaluated on a case-by-case basis [83]. Cannabis smoke exposure to the child, and breastfeeding during the hours after cannabis use, should be avoided [84].
Buprenorphine might also be safe during breastfeeding and opioid-dependent women can be counseled accordingly [76,77,85,86]. There appears to be no relationship between maternal buprenorphine dose at delivery and the severity of neonatal abstinence syndrome, the amount of morphine needed for treatment and the duration of treatment [87]. The outcomes of newborns of pregnant women using methadone and buprenorphine appeared to be similar, with the exception that buprenorphine-exposed infants presented with significantly larger head circumference and tended to have higher weight and length [88]. According to a recent Cochrane review, the differences between methadone and buprenorphine (or slow-release morphine) do not allow for a conclusion that one treatment is superior to another [89].
A very recent retrospective, observational assessment of meconium toxicology performed on samples of a high-risk patient cohort, however, demonstrated that, at least a third of pregnant women on methadone-maintenance therapy continue to use at least one additional opioid narcotic [90]. No significant difference was found for opioid or other illicit drug use between the methadone-positive and -negative meconium samples, indicating similar patterns of substance use during late pregnancy. The authors of the study speculated that, subtherapeutic dosing might have created withdrawal symptoms leading to additional substance use. In addition, these results may be an indication of partly inadequate delivery of addiction support services [90].
In our institution, breastfeeding is possible in methadone-substituted women, provided that weekly (but unheralded) urinary toxicology screens are negative for other drugs.
Postpartum period
Special attention has to be given to the postpartum period [91]. Alcohol withdrawal, for example, generally occurs after 48 h, thus, in the postnatal ward, the woman might appear to be agitated and have problems caring for her baby during this time. Users of cocaine and amphetamines might even be abusive and exhibit strange or inappropriate behavior.
Neonatal abstinence syndrome
Opiate-dependent women should be informed that neonates exposed during pregnancy need to be monitored closely for symptoms and signs of neonatal withdrawal [92], as 60–90% of neonates with in utero exposure to opiates suffer from drug withdrawal [86,93]. Withdrawal symptoms typically depend on the substance, and are predominantly autonomic, neurologic or gastrointestinal. They generally occur within 24 h after delivery for heroin and 2–6 days for methadone. This is in contrast to symptoms of benzodiazepine withdrawal, which can be delayed [94,95]. A British study on neonatal abstinence syndrome found great variability in policies for its detection and treatment [96]. Neonatal abstinence syndrome has not been conclusively demonstrated in marijuana- or cocaine-exposed neonates [97,98].
An often unrecognized entity is the neonatal nicotine withdrawal syndrome, albeit its existence is questioned by some authors [99]. Its onset is typically within 12–24 h of life and resolves usually within 36 h, rarely requiring treatment [100,101]. Neonatal nicotine withdrawal syndrome may be misdiagnosed as infant colic when a smoking, breastfeeding mother discontinues breastfeeding [102].
Bonding
Breastfeeding has a positive impact on bonding; however, as drug-using women often have difficulties in building a relationship with their newborn, additional support by a pediatric psychiatrist might be helpful [40]. Furthermore, a psychiatrist or psychologist has the skills to provide mediation when conflicts between the patient and staff occurs, and is thus ideally part of the interdisciplinary team. In other settings and depending on local resources, the general practitioner, social worker or addiction counselor may have a similar role, with the advantage that they continue to follow the woman and her child in the postpartum period.
As associated legal and social problems can impede appropriate care, and can impair the ability of the mother to care for her child after birth, well-functioning social services should be involved [32]. Systematic information of the child welfare authority about drug-using mothers allows assistance in crisis situations and provision of help if additional childcare is needed.
Attitude towards drug-using pregnant women
Despite the obvious challenges for all disciplines in the care of drug-using women, the importance of being supportive and nonjudgmental is underlined in the literature reviewed for this article [103–105]. Care of drug-using women can be a tightrope walk between considerate care and paternalism, as both support and assistance are necessary. The patient–doctor relationship may be difficult, particularly in case of psychiatric comorbidity (e.g., borderline disorder), and requires patience. It is of utmost importance to work in a constant, transparent fashion in order to gain commitment from the mother's side by integrating her in the decision-making process. Institutionalized controls of toxicology screenings are recommended since they are more easily accepted.
Long-term outcome & preventive strategies
Although pregnancy might be a ‘window of opportunity’ for drug-using women, many patients do not succeed in maintaining the necessary stability over time [7]. According to several studies, this is only the case in less than half of the families concerned (risk factors: psychiatric comorbidity, history of prostitution, homelessness, delinquency and a drug-addicted partner) [40,41]. The partner, or the father of the current pregnancy, may also be a drug user. In a sample of 240 pregnant women who voluntarily entered a substance abuse treatment program, most fathers were supportive of seeking treatment. The majority of these urban, predominately African–American, opiate- or cocaine-dependent women, had long histories of drug use, which had often begun during adolescence. They often had family members with a history of alcohol and drug use. People in their social environment frequently animated their drug use [41].
Birth control
Another important issue is birth control, which may even be discussed during pregnancy so that the patients can choose a method by the time they deliver. Long-acting progestogen devices can be applied early in the postpartum period. In general, a pregnancy should be well planned in these patients and family-planning advice should be given. This allows discussing possible difficulties and preventive strategies in advance.
Conclusion
As caring for drug-using pregnant women is challenging, standards of care and an interdisciplinary approach is required. The ultimate aim of these interdisciplinary efforts is to reduce the risk for adverse outcomes for the mother and her baby, both during pregnancy, the neonatal period and in the long term. A well-implemented standardized approach may also alleviate the demanding task of health professionals who are engaged in caring for drug-using pregnant women, and could possibly reduce concomitant distress when the patient–doctor relationship is particularly difficult.
Future perspective
Early identification of drug-using habits and of the patterns of use by family practitioners, for example, in the preconception period, may provide the opportunity to assist affected women in reducing major health risks [106]. The surrounding social context in which drug use commonly occurs should certainly be taken into account. In order to comprehensively follow drug-addicted women during pregnancy, thorough knowledge of certain aspects, such as effects of the drugs on the fetus and of breastfeeding on the newborn, are crucial on one hand, but on the other hand, continuous, concise and interdisciplinary care may even be more important. A pregnancy might act as a sentinel event that can help drug-using mothers to start modifying their behavior [107]. This may also have an impact on their children.
Further research should focus on assessing and evaluating interdisciplinary strategies to prove their effects and efficacy in the respective settings.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Executive summary
Impaired fertility was common in heroin-using women in the past, but, nowadays, generally improves in the context of substitution programs.
Drug use in pregnant women poses an increased risk for adverse health outcomes both for the mother and child.
It is difficult to discern direct drug effects from other factors, such as smoking, poor diet, stress and poor social circumstances.
Besides the specific effects of the various substances on the fetus, drugs generally cause preterm labor and low birth weight.
Cigarette smoking, alcohol use and poor social circumstances are all common in women using illicit drugs, and are concomitant factors that might be neglected when assessing drug-using women.
Psychiatric comorbidity is frequent in drug-using women (e.g., depression and anxiety disorders).
Psychiatric comorbidity can either be a cause or consequence of drug use.
It is known that the lack of antenatal care is associated with worse outcomes for mother and child.
Comprehensive, interdisciplinary treatment programs are likely to have a positive impact on outcomes.
Care needs to be as easy and comfortable for the patient as possible since compliance is an issue.
Care of drug-using women can be a tightrope walk between considerate care and paternalism, as both support and assistance are necessary.
During delivery, special attention has to be paid to unusual behavior or physiological signs of drug abuse.
Breastfeeding is possible both in methadone- and buprenorphine-substituted women.
In the postpartum period, withdrawal generally occurs after 48 h for alcohol, after 24 h for heroin and after 2–6 days for methadone, meanwhile benzodiazepine withdrawal can be delayed.
Although pregnancy and consequent motherhood may be a ‘window of opportunity’ for drug-using women, many patients do not succeed in maintaining the necessary stability over time.