
Abstract
Keywords
Female genital cutting affects over 140 million women worldwide. Prevalent in certain countries of Africa and the Middle East, the practice continues among immigrants to industrialized countries. Female genital cutting is a deeply rooted tradition that confers honor on a woman and her family, yet also a traumatic experience that creates significant dermatological, gynecological, obstetric and infectious disease complications. Little is known about postmenopausal health in cut women. The international community views this practice as a human rights violation. In addition to genital health complications, the medical community must confront an understudied concern of what happens as this population ages. These challenges must be addressed to provide optimal care to women affected by female genital cutting.
Female genital cutting (FGC) comprises all procedures that involve partial or total removal of the external female genitalia, or injury to the female genital organs, for cultural or nontherapeutic reasons [1]. The WHO estimates that over 140 million women and girls worldwide have been subjected to this practice and that each year about 3 million more girls are at risk for some form of genital cutting. It occurs at high rates in 28 countries in Africa and to some degree in certain countries of the Middle East and Asia (Yemen, Oman, Saudi Arabia, United Arab Emirates, Bahrain, northern Iraq, Malaysia, Indonesia, Pakistan, India and southern Israel). The WHO defines four main categories of FGC (Figure 1) [2]:

Type I: excision of the prepuce with partial or total excision of the clitoris (clitoridectomy);
Type II: excision of the clitoris with partial or total excision of the labia (clitoridectomy and/or labial excision; types of FGC that involve cutting of the clitoris are known in some places as the Sunna form);
Type III: excision of part or all of the external genitalia and narrowing and covering the vaginal opening by joining and fusing the raw edges of the labia with stitches or glue, leaving a small opening for the flow of urine and menses (infibulation, also known as the Pharaonic form);
Type IV: includes other forms of nontherapeutic genital alteration such as pricking, piercing, incising the clitoris or labia; stretching the clitoris or labia; cauterizing the clitoris and surrounding tissue; scraping the vulvar vestibule; cutting the vagina; and introducing caustic substances, poultices or herbs into the vagina to create tightening or narrowing of the vaginal vault.
Because cutting often involves rudimentary techniques, the WHO describes subsets of these categories to approximate the range of possible outcomes (Table 1).
Growing numbers of immigrants from countries where this practice is common have settled in North America, Western Europe, Australia and New Zealand, bringing the practice with them. Global authoritative bodies, which have declared the procedure a violation of bodily integrity and human rights, use the term, female genital mutilation. Because women from affected regions may not view themselves as having been mutilated, this review uses the neutral term, ‘female genital cutting’. The authors have a particular interest in how FGC affects a woman's quotidian quality life, from everyday menstrual health and hygiene, to sexual health, pregnancy, childbirth, and postmenopausal challenges. This review describes the cultural determinants of the practice, its impact on health and wellbeing, and areas where further research is needed. Limited research exists on the prevalence and consequences of FGC within immigrant communities to the developed world, perhaps because practice is illegal in many immigrant-receiving communities. The goal of this review is to highlight the health and emotional concerns of these women with sensitivity so that we can improve their quality of life.
Prevalence
The practice of FGC has ancient sources, although no definitive evidence exists on how it began. It was part of ancient Egyptian culture and has been found in mummies [3]. Some speculate that it may have originated with the ancient Greeks or in pre-Islamic Arabia. In the 19th century, clitoridectomy was advocated in England and North America for the treatment of hysteria and masturbation, a theory that was eventually debunked [4]. Today, cutting is most prevalent in 28 countries of Africa, with the highest rates in Egypt, Somalia, Sudan, Eritrea, Guinea, Sierra Leone, Mali and Djibouti (Table 2). The type of FGC varies depending on the country, the traditional practices of the region, religious beliefs, levels of education and economic development and the ethnicity and tribe to which the woman belongs (Table 3) [5–9].
Prevalence of female genital cutting in traditional societies of the developing world.

Data taken from [21].
NA: Not available; NK: Not known, no detailed demographic breakouts found; NR: Not reported.
Types of female genital cutting in African countries.

NA: Not available; NR: Not reported.
The practice continues among immigrants to the developed world. The European Parliament estimated that up to half a million women living in the European Union have been subjected to FGC, with 180,000 more at risk [25]. In 2001, it was estimated that 174,528 women residing in England and Wales had been born in a country that practices FGC, a figure considered to be an underestimate [26]. Based on the 2000 US census, the US CDC and the African Women's Health Center in Boston estimated that over 200,000 girls and young women in the USA were at risk for undergoing FGC [27]. However, between 2000 and 2012, the population of African-born immigrants to the USA more than doubled, from 750,000 to 1,724,000 [28]. A total of 48% are women and 68% are from countries in North Africa, Eastern Africa and Western Africa where FGC is most prevalent [28]. Although prevalence varies by ethnicity, region and tribe, assuming that the prevalence of FGC among women in immigrant communities reflects that reported by the WHO for their country of birth overall, we estimate from 2012 figures that roughly 340,000 women in the USA may be affected or at risk for FGC (Table 4).
Estimates of African-born immigrant populations in the USA potentially affected or at risk for female genital cutting, based on 2012 American Community Survey, US Census Bureau.
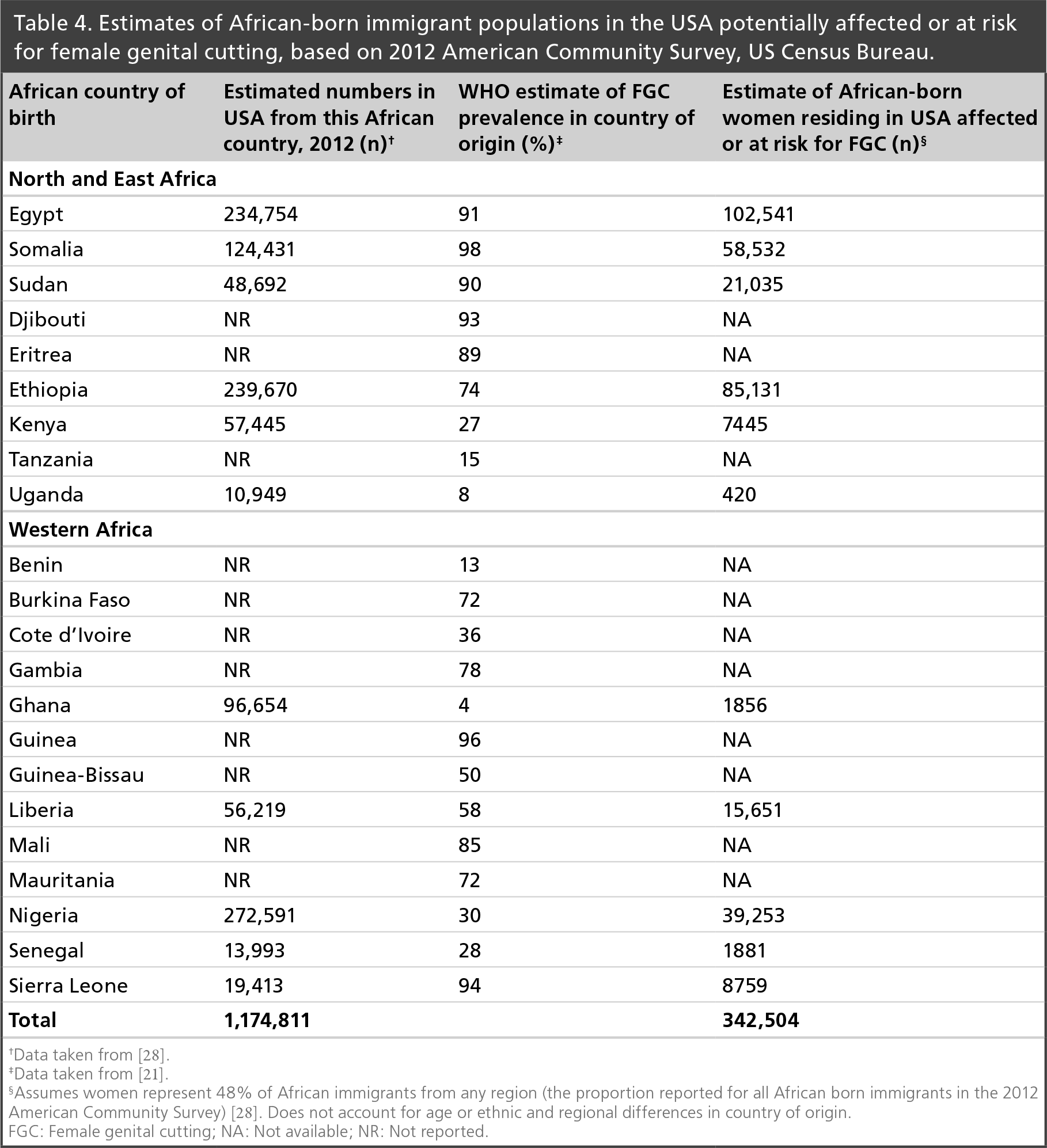
Data taken from [28].
Data taken from [21].
Assumes women represent 48% of African immigrants from any region (the proportion reported for all African born immigrants in the 2012 American Community Survey) [28]. Does not account for age or ethnic and regional differences in country of origin.
FGC: Female genital cutting; NA: Not available; NR: Not reported.
US healthcare providers should be aware of this growing at-risk population. States with the largest African-born populations are California, New York, Texas, Maryland and Virginia [29]. Sizeable numbers of immigrants from affected countries reside in the major metropolitan areas of: Los Angeles, Riverside, Orange County, San Diego and San Francisco, Oakland, San Jose, California; New York, Northern New Jersey, Long Island and New York, New Jersey, Pennsylvania; Houston, Galveston, Brazoria and Dallas, Fort Worth, Texas; and Washington, Arlington, Alexandria, Washington, DC, Virginia, Maryland, West Virginia [27]. In addition, sizeable enclaves of refugees from countries with civil unrest have formed in some mid-western cities. Somalis, for example, represent the largest influx of African refugees to the USA in the last two decades; 50,000 or more have settled in Minnesota and represent one in five immigrants to that state [30]. As of 2012, over 45,000 have settled in Columbus, Ohio, with 200 more arriving each month [31].
Cultural determinants
FGC is traditionally performed on young girls as an obligatory social norm to ensure an honorable and worthy womanhood. The age and manner in which procedure is performed varies. In some cultures, midwives and birth attendants perform the procedure on infants; in others, it is the purview of older female relatives or traditional circumcisers. In Egypt, traditional midwives or dayas were called upon historically, but today, medical personnel perform more than half of all procedures [10]. In most countries, girls are typically cut between the ages of 4 and 18 years, although the procedure is most often accomplished before menarche. In Egypt, for example, 80% of girls are cut between the ages of 5 and 9 years [32]; in Gambia, between the ages of 4 and 7 years [33]; in Mali, the median age is 6 years, with a range of 1–16 years [34]; in Tanzania, the median age is 10 years [6]; in Ethiopia over 80% are cut by age 11 years [15]; among Somalis, at least half are cut by age 8 years and 95% by age 12 years [12].
In traditional societies, girls are held down with spread legs and the operation is performed without anesthesia using unsterilized knives, razorblades, scissors, cut glass or sharp stones. In Type I, the most common form, the clitoris is held between the thumb and forefinger and amputated with a single stroke. Packing the wound with bandages under pressure stops the bleeding. Trained personnel may stitch the clitoral artery. In Type II, the clitoris and labia minora may be removed with the same stroke, and the extent of cutting varies. In Type III, the clitoris, labia minora and inner surface of the labia majora are removed, and the cut surfaces of the labia majora are stitched together with thorns or glued with sticky substances to create fusion. The girl's legs will be bound for several weeks to accomplish healing, during which time female relatives attend to her. The procedure creates a hood that covers the urethra and most of the vagina, leaving a small opening for the passage of urine and menses. By contrast, in subgroups such as the Arab Bedouin tribes of southern Israel, the ritual remains culturally important but has been reduced to a clitoral nick with one or two stitches [35].
Although attitudes are changing, FGC has been a deeply rooted societal norm and a number of cultural beliefs contribute to its significance [14,36,37]. It is a tradition and social obligation that brings honor to the girl and her family. Cutting reduces sexual drive and ensures that the girl remains chaste, marriageable and faithful. Although practiced by members of various religious traditions [8,35], in predominantly Muslim communities it is often believed to be a religious obligation, and the vernacular term, Sunna, which also conveys the traditions of the Prophet, imbues some religious significance [14,37]. However, in recent years, government bodies and religious leaders have campaigned against the practice, particularly in its most extreme forms. Hygiene and esthetic norms also play a role. In some societies, the external genitalia are considered unclean and unsightly; the clitoris is viewed as a male appendage that must be removed or an organ that must be bled for cleansing and purification [38]. Last, FGC is a rite of passage that reinforces cultural identity and a sense of belonging.
In some societies, the procedure is secret and young girls are unaware of the event until they are taken aside by their mothers or female relatives to have the procedure done. In others, girls will be advised that a special event is about to transpire, although its details may not be fully understood. Still others are told they will be cut but reassured that although it is painful, they will recover. Cultural cues reinforce its social significance [38]. Uncut girls may not be allowed to serve tea or prepare food because they are unclean, and may be teased or ostracized by their cut peers. Well-known derogatory terms reinforce the view that remaining uncut would be shameful. In some communities, FGC is a celebratory rite of passage. In Sierra Leone, for example, FGC takes place as part of a group initiation into the Bondo Society, a secret society of women [39]. The event, run by a society leader who also performs the cutting, takes place in a private clearing in the bush, where the girls will spend days or weeks to be instructed in the norms of womanhood. Initiates are rewarded with celebrations, gifts and public recognition. Whatever the context, the procedure is initially painful and traumatic, but girls are reassured that they have been brave and strong and are now pure, beautiful and worthy [38]. Through affirmation and inclusion, cut girls develop a sense of pride, cultural identity and social acceptance. Mothers and grandmothers gain respect for having done their duty to foster an ideal young woman.
Health consequences
Health complications may vary with the extent of cutting, although only a limited number of studies break out this risk systematically.
Immediate complications
When cutting is performed with rudimentary techniques and without anesthesia, the immediate complications can include severe pain; hemorrhage from the internal pudental artery or the dorsal artery of the clitoris; damage to the urethra, vulvar vestibule and vaginal walls; urinary retention during the period of healing from Type III cutting (infibulation); bone fractures due to pressure applied to the struggling girl; tetanus from unsterilized instruments; septicemia; shock due to blood loss and death (Table 5).
Health consequences of female genital cutting.

FGC: Female genital cutting; HSV: Herpes simplex virus.
Long-term complications Dermatological changes
Tissue damage and improper healing occasioned by the rudimentary cutting techniques create several complications. Chronic vulvar pain may result from trapped or unprotected nerve endings. Keloid scars, which are particularly common in people of African descent, result from progressive overgrowth of dense fibrous tissue (collagen) after wound healing [24]. Numerous cases of clitoral or vulvar epidermal inclusion cysts have been reported [40–43,57,58]. Inclusion cysts arise from invagination of the keratinizing epidermis into the dermis, and the cyst is lined with a wall of true epidermis. They are slow-growing, beginning as a painless swelling at the cut site and gradually increasing in size over several years to form a large clitoral or vulvar mass (in one study, 40% were larger than 3.5 × 6.5 cm at an average age of 17) [59]. Cysts are socially stigmatizing when they interfere with walking or sitting or are apparent to the spouse. Besides cysts and abnormal scars, two rare complications are neuroma of the clitoris, which also presents as a mass [24], and vulvar lymphangiactases, which appear as itchy, wart-like papules resulting from damage to the lymphatic tissue [60]. The papules may be superimposed on lichenified tissue due to chronic scratching.
Urological effects
Damage to the urethra can result from any form of cutting. Slow, painful micturition, dribbling urinar y incontinence, urinary retention and recurrent urinary tract infections are common sequelae of infibulation [44,45].
Menstrual health & hygiene
Women who have undergone infibulation suffer high rates of dysmenorrhea due to congestion from obstructed menstrual flow (hematocolpos) [24,46]. Often women do not understand the cause of their symptoms, unless they learn about the health complications of FGC through educational efforts or discover relief from symptoms after undergoing defibulation by a healthcare professional [37].
Limited research exists on menstrual hygiene in these populations. A prospective, examiner-blind clinical trial of disposable sanitary napkins was performed in Abuja, Nigeria among 283 women aged 18–45 years, 20% of whom had undergone Type I FGC [61]. The study compared a locally produced disposable pad and an imported pad designed to trap and keep fluid away from the skin. Mean number of pad changes during the menstrual period ranged from 1.20 to 3.30 per day, depending on flow levels. The imported pad was preferred for lack of soreness or tenderness and for not feeling wet during wear. Neither product was associated with adverse effects.
A hospital-based, case–control study of cervical cancer in Mali, which examined women who had undergone FGC (95.1% of cases and 92.8% of controls), found that lack of care in cleaning the genitalia was associated with a 5.6-fold increased risk of invasive cervical cancer [34]. Use of commercial sanitary napkins or tampons was virtually nonexistent in the population. Reusing homemade sanitary napkins was almost exclusively restricted to cancer cases, resulting in a 46-fold odds ratio for cervical cancer associated with this practice when adjusted for age, availability of a toilet inside the home, parity and human papillomavirus serostatus [34]. Malian women often report repeated use of menstrual pads that are not always clean, possibly due to lack of access to tap water. Whether FGC contributes to the excess cervical cancer risk in Malian women by impeding adequate menstrual hygiene cannot be ascertained from this study. Poor menstrual hygiene and the rewashing of rags for menstrual protection have been linked to genital infections in other resource-poor countries [62]. For example, poor genital hygiene was associated with cervical cancer in rural China, while sanitary napkin use was protective [63].
Obstetric & perinatal complications
FGC is associated with adverse obstetric and perinatal outcomes and the excess risk depends on the severity of cutting. A large, prospective collaborative study sponsored by the WHO in 2006 examined 28,393 patients at 28 obstetric centers in Burkina Faso, Ghana, Kenya, Nigeria, Senegal and Sudan [48]. Cut women were at higher risk for caesarian section, postpartum hemorrhage, extended maternal hospital stay, infant resuscitation, stillbirth or early neonatal death and low birth weight. The excess risk rose with the extent of cutting: women with Type III FGC had a 69% higher risk of postpartum hemorrhage, a 98% higher risk of extended hospital stay, a 66% excess risk of requiring infant resuscitation and a 55% excess risk of stillbirth or early neonatal death [48]. Parity did not significantly affect these relative risks. FGC was estimated to lead to an extra one to two perinatal deaths per 100 deliveries.
Numerous studies have been performed in various locations and utilizing different approaches (case series, case–control studies and cross-sectional surveys, among others) A recent meta-analysis of 28 comparative studies, involving almost 3 million women, provides considerable supporting but not conclusive evidence that FGC is associated with obstetric complications [49]. The analysis found that cut women were 3.3-times more likely to experience difficult or prolonged labor and twice as likely to experience obstetric hemorrhage. Vaginal stenosis and obstruction around the introitus associated with more invasive forms of FGC could contribute to prolonged labor; the inelasticity of vulvovaginal scar tissue could contribute to the increased risk of perineal tears and hemorrhage.
Rates of maternal morbidity and mortality are higher in countries that practice FGC compared with more developed regions, with hemorrhage being the leading cause of maternal mortality [64]. Countries in which the majority of women undergo the most extensive forms of FGC, such as Somalia and Djibouti, have a higher maternal death rate (>700 per 100,000 live births) than countries with a much lower prevalence of FGC but similar midwifery practices, such a Kenya and Tanzania (<500 per 100,000 live births) [14].
Some excess risk of prolonged labor or postpartum hemorrhage may persist among immigrants to developed countries. Studies dating to the initial time period of Somali immigration to the USA and Europe suggested that immigrant women were at higher risk for perineal laceration and postpartum hemorrhage [65–67], perhaps due to challenges in communicating effectively with immigrant patients and their resistance to western obstetrical interventions [31]. However, other investigations of immigrant women with FGC receiving modern obstetric care in Saudi Arabia, Israel and Western Europe have found no difference in rates of prolonged labor or other perinatal complications [68–70]. In developed countries, it has become more common to offer the patient anterior episiotomy during labor and not reinfibulate after delivery.
Obstetric fistulas, a potential complication of FGC, result from necrosis of urogenital structures when compressed between the fetal head and the mother's pelvis during obstructed labor. Urinary incontinence results from sloughing of the posterior wall of the bladder or urethra and fecal incontinence from pressure necrosis of the posterior vaginal wall and neighboring rectum. These consequences are devastating to the woman, both physically and socially. Several case reports involve women who have undergone Type III FGC or caustic narrowing of the vagina [50,51]. However, a recent study in Ethiopia found that Types I and II FGC were not independent causative factors in development of vesicovaginal fistula from obstructed labor [52]. The high rate of obstetric fistulas in countries where FGC is prevalent could also be related to risk factors such as early marriage when pelvic growth is incompletely coupled with the lack of emergency care.
Sexual health
Studies of the sexual health of women who have undergone FGC vary in location, methodology, quality and in the types of cutting represented, making broad conclusions difficult. A systematic meta-analysis of 17 comparative surveys of cut and uncut women, comprising a total of 12,755 participants, concluded that the evidence base was insufficient to draw conclusions about the psychological and social consequences of FGC [47]. The analysis suggested that cut women are more likely to experience pain during intercourse, reduced sexual satisfaction and reduced sexual desire, but the quality of the evidence was judged too low to conclude a causal relationship to FGC.
Blood-borne & sexually transmitted infections
Wound infections and sepsis can develop due to unsterile conditions employed when girls are cut, and group cutting with the same instrument may increase the risk of transmitting blood-borne diseases such as hepatitis B and HIV. Among pregnant women in Yemen, for example, being cut was significantly associated with seropositivity for hepatitis B antigen [71]. Cut women with Type II FGC in rural Gambia had a 66% higher risk of bacterial vaginosis, which the investigators speculated might be related to removal of the labia minora [33]. Cut women also had a 4.7-fold higher prevalence of herpes simplex-2 infection [33], an epidemiologic risk factor for HIV throughout Africa [53]. Analysis of demographic variables among 3167 Kenyan women aged 15–49 suggests that FGC is indirectly associated with HIV risk through associated practices in adulthood [54]. Specifically, cut women are 1.72-times more likely than uncut women to have older partners (perhaps through arranged marriage) and women with older partners are 2.65-times more likely than women with younger partners to test positive for HIV; moreover, cut women have 1.94-times higher odds than uncut women of initiating sexual intercourse before they are 20, and women who experience their sexual debut before age 20 have 1.73-times higher odds of testing positive for HIV. However, a study of 379 clinic patients in Tanzania found no association of FGC with hepatitis B, HIV or reproductive tract infections [6].
Psychological impact
Human rights advocacy groups and women's health centers that serve immigrant women affected by FGC obtain poignant testimony of the psychological trauma they endure [37,72,73]. Evidence of post-traumatic stress disorder has been observed in subsets of women in their home countries and among immigrants to the West [55,74]. Not all women process their experience in the same way; it is colored by the meaning they create of this tradition and their own adaptive styles.
Postmenopausal health
Vulvovaginal atrophy is a natural consequence of hypoestrogenism following the menopausal transition (reviewed in [75]). It is a growing women's health concern as the population of the industrialized world ages. In the intact woman, the labia atrophy and lose elasticity, the introitus narrows and the clitoral hood may become phimotic. The vagina becomes shorter and narrower and loses the typical folds (rugae); the vaginal epithelium is more friable and prone to friction-induced bleeding. Vaginal pH rises above 4.5, increasing susceptibility to infection. Atrophic symptoms in the intact woman include vaginal dryness, itching or burning, painful intercourse, increased urinary frequency, dysuria and nocturia.
However, in the less developed countries of Africa, the risks of HIV infection, maternal mortality and limited access to healthcare reduce life expectancies to some of the lowest levels globally. Life expectancy for women in Tanzania, for example, is 53 years, and FGC is a risk factor for early death [76]. African immigrants to the USA are less likely to be over age 65 years than the native or foreign born population; two-thirds of African-born immigrants are under age 45 years [28,30]. No systematic studies are available on postmenopausal urogenital health in women who have undergone FGC and their needs are unad-dressed. Health professionals in the developed world who serve immigrant communities must examine the sequelae of aging in cut women, raise awareness and address the impact of FGC on postmenopausal health and quality of life.
Efforts to end FGC
Over the last three decades, the international community has mounted efforts to end the practice of FGC, spearheaded by organizations within the United Nations, the WHO, the legislatures of affected countries and nongovernmental organizations. In numerous international and regional declarations, FGC is acknowledged to be a violation of human rights and bodily integrity, as the practice has no therapeutic benefits, is known to cause physical and psychological harm and is often carried out on children too young to give informed consent [1]. Although the practice remains deeply rooted, slow progress has been made. Prevalence remains high in Somalia, Djibouti and Egypt [77], but change is underway. In Somalia, for example, the adverse consequences of Type III cutting have become more broadly acknowledged; however, some religious leaders defend milder forms of the practice, leading to the erroneous perception that the Sunna form is benign and fulfills religious obligations [37,78]. Prevalence has dropped most dramatically in Burkina Faso, Mauritania and Senegal [7,77]. In Burkina Faso and Mauritania, authorities employ a multi-pronged approach: They initiate educational programs to change perceptions, enlist prominent groups to champion eradication, gain support from practitioners such as midwives and traditional healers, promote alternative symbolic rites of passage and enforce legislation [7]. Tostan, an nongovernmental organization working in rural areas of Djibouti, Guinea, Guinea-Bisau, Mali, Mauritania, Senegal, Somalia and the Gambia, fosters respectful and inclusive community-led training for broad-scale development and social change [17]. A 3-year community empowerment program with trained facilitators provides villagers with information on human rights, as well as practical skills in the areas of hygiene, health, democracy, literacy, math and project management. Community members then determine a collective vision for their future, consider which practices in their villages do not lead to well-being, and make celebratory public declarations committing to end harmful ones such as FGC. UNICEF reports that although in Mali, Guinea, Sierra Leone, Somalia, Gambia and Egypt more than half of the female population think the practice should continue, in 19 of 29 African countries where FGC is practiced, most girls and women now think that it should end [79].
Ending the practice among immigrant communities in the West also presents a challenge. Attitudes among immigrant women vary from region to region, depending on evolving norms. Some women see migration as an opportunity to reassess the practice, but obstacles to change do exist. FGC-affected communities encounter an alien culture: promoting traditional norms maintains social cohesion against intrusive foreign ideas [36]. Some communities are deeply threatened by the sexual liberalism in western society. The emphasis on individual rights over group identity is seen as discriminatory and in conflict with religious beliefs [38]. To protect their daughters, women themselves keep the practice alive. The illegality of FGC in host countries drives the practice underground; it persists by enlisting the help of traditional circumcisers within the immigrant community or by sending girls to relatives in the home country for vacation cutting [73].
Women from FGC-affected societies face a culture of silent endurance; some are unaware of the prevalence of complications, and may attribute their personal suffering to shameful behavior or unclean spirits. Because western notions of individual rights do not always resonate, changes in perception require interventions that are respectful and sensitive to the culture. An example from Norway illustrates the challenges of cross-cultural intervention [72]. When a foreign speaker addressed a group of Gambian immigrants about the health consequences of FGC, the information was rejected as not credible. However, when a female Gambian doctor presented slides of little Gambian girls with scars, cysts and fstulas caused by FGC, the information, although shocking, was believable; as the doctor hummed the secret songs from the initiation ceremony, the audience was galvanized by the realization that she too had been cut. Such discoveries are psychologically painful, however, prompting a deep sense of loss [72]. Time and emotional healing are needed to process this new understanding. Consequently, educational efforts require great sensitivity, the cooperation of families and influential leaders and access to culturally competent support groups. The power of social norms cannot be overemphasized. Only when communities feel it is not detrimental to do so, will they change.
Conclusion
FGC is a deeply rooted social norm among women from several countries in Africa, the Middle East and Asia. Growing numbers of immigrants from FGC-affected societies now reside in North America, the EU, Australia and New Zealand. To provide optimal care, healthcare providers in developed nations need training to better understand both the cultural context of this practice and its complications. The African Women's Center located at the Brigham and Women's Hospital in Boston is the first and only African health practice in the United States that focuses on issues related to FGC. Founded by Nawal Nour, a native of Sudan, its mission is to holistically improve the health of refugee and immigrant women affected by the tradition and is a resource for culturally sensitive information for patients and healthcare providers [80]. The WHO offers numerous resources, including a manual on prevention and management of female genital mutilation for nursing and midwifery students [81].
Future perspective
While work continues to eradicate FGC in indigenous societies, we envision a future in which FGC-affected immigrant communities in the developed world receive holistic support. In the authors’ opinion, the ideal situation would be one in which formal training on FGC was developed for healthcare providers, school personnel and social service workers. Pediatric care providers would learn about this cultural norm to facilitate early intervention. They would be trained on how to address the practice and its complications in a factual yet sensitive manner. Training for school counselors and nurses would cover the cultural context of FGC, the urinary and menstrual complications that affect these girls and their potential need for information on adequate menstrual hygiene. Obstetricians, gynecologists, nurses and midwives would be formally trained on how to care for these patients, how to provide information on obstetric interventions and gynecological complications, and how to interact with their spouses in a culturally competent way. Moreover, virtually nothing is known about the postmenopausal experience of these women. Prospective research should be initiated in immigrant communities as emphasis shifts to aging populations and geriatric care. Psychological and sociological research should explore how affected girls, women and families process the information that cutting is not universal and how this influences their integration into the host country at various life stages, from school to marriage and beyond. Community centers could be established to facilitate culturally competent collaboration between women's health advocates, healthcare providers, immigrant thought leaders, families, individuals and social welfare organizations, to build trust and encourage positive change over the long term.
Executive summary
Female genital cutting (FGC) comprises all procedures that involve partial or total removal of the external female genitalia, or injury to the female genital organs, for cultural or nontherapeutic reasons.
The WHO defines four major categories:
– Type I: clitoridectomy;
– Type II: clitoridectomy and/or partial or complete removal of the labia;
– Type III: infibulation, in other words, excision of part or all of the external genitalia and narrowing and covering the vaginal opening by joining and fusing the raw edges of the labia, leaving a small opening for the flow of urine and menses;
– Type IV: any other alteration of the external female genitalia for nontherapeutic reasons.
FGC is prevalent in 28 African countries and in some communities in the Middle East and Asia. Over 140 million women and girls worldwide have undergone FGC. Up to 500,000 women living in the EU have been subjected to FGC; 340,000 girls and young women in the USA may be affected or at risk.
FGC is performed on girls as a social norm. Depending on the society, midwives, traditional circumcisers, respected elders in society, older female family members or medical practitioners, may perform cutting.
Short-term complications include severe pain (no anesthesia); hemorrhage; infections (including tetanus, sepsis or blood-borne illnesses); shock and death.
Dermatological complications include vulvar pain; keloid scars; clitoral or vulvar inclusion cysts; neuroma; and vulvar lymphangiactases.
Urogenital complications include slow and painful micturition; urinary retention; urinary incontinence; and recurrent urinary tract infections, dysmenorrhea, pelvic congestion and infection.
Women with FGC are 3.3-times more likely to experience difficult or prolonged labor and twice as likely to experience obstetric hemorrhage, depending on severity of cutting.
Little is known about postmenopausal urogenital health in women who have undergone FGC.
Although the practice remains deeply rooted in some traditional societies, attitudes are changing. In 19 of 29 African countries where FGC is practiced, most girls and women now think that it should end.
The long-term health issues of cut women must be examined.
A holistic approach to the needs of refugee and immigrant women will build trust and empowerment in underserved communities.
Footnotes
MA Farage, KW Miller, GE Tzeghai and CE Azuka are employees of P&G. WJ Ledger and JD Sobel are expert advisors.
The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
The authors acknowledge Barbara Swift for assistance with the literature search and Deborah Hutchins of Hutchins & Associates LLC (Cincinnati, OH, USA) for technical and editorial assistance (funded by the Procter & Gamble Company).