
Abstract
Endometriosis is a complex gynecologic condition affecting 6–10% of reproductive aged women and is a major cause of chronic pain and infertility. Mechanisms of disease pathogenesis are poorly understood. Considerable evidence supports the existence of a stem cell population in the endometrium which provides a physiologic source of regenerative endometrial cells, and multiple lines of evidence now support a key role for stem cells in the pathogenesis of endometriosis. In addition, new blood vessel formation is critical for the establishment and maintenance of endometriotic implants, a process in which endothelial progenitor cells may play an integral role. These new insights into disease pathogenesis present exciting opportunities to develop targeted and more effective therapeutic options in the management of this common and challenging disease.
Keywords
Endometriosis is a benign gynecologic condition defined by the presence of endometrial glands and stroma outside of the uterus. The disease is most commonly found in the pelvis on the ovaries, anterior and posterior cul-de-sac peritoneum, uterosacral ligaments, uterine serosa, posterior broad ligaments and rectovaginal septum. Less common sites include the intestine, bladder, pelvic lymph nodes and rarely the cervix, vagina, abdominal wall, skin, pleura and brain [1–4].
In the USA, endometriosis affects 6–10% of reproductive aged women, and is estimated to affect 176 million women worldwide [5,6]. The prevalence of the disease is even higher (up to 50%) in women with pain and infertility [7]. The disease is therefore a major public health burden, causing disability, reduced quality of life and, since women comprise 50% of the US workforce, massive loss of productivity. Estimated annual costs in the USA for diagnosing and treating endometriosis was estimated at US$22 billion in 2002 [8].
Despite the wide prevalence and great public health significance of endometriosis, mechanisms of disease pathogenesis remain poorly understood. Mounting evidence over the last decade supports the existence of a stem cell population in the endometrium that provides a source of regenerative endometrial cells, and more recent data now demonstrate a role for stem cells in the pathogenesis of endometriosis. The purpose of this review is to provide an update on the current evidence for a role for stem cells in endometrial function and in endometriosis.
Risk factors
Multiple risk factors for endometriosis have been identified. There is clearly a higher prevalence of disease in women with obstruction of menstrual flow, as seen, for example, in obstructive Müllerian anomalies [9]. Since the disease is estrogen-dependent, prolonged exposure to endogenous estrogens (as occurs with early menarche, late menopause and obesity) is associated with a higher risk of endometriosis [7]. Specific reproductive characteristics including nulliparity, longer duration of menses, short menstrual cycles and menorrhagia also increase the risk for endometriosis [10]. Genetics plays a role as well, with a seven-fold higher risk of endometriosis in women with affected first-degree relatives [11]. The specific genetic factors that predispose women to endometriosis are not well understood; the disease is likely polygenic, and multiple lines of evidence suggest that various epigenetic modifications contribute to disease (reviewed in [12]). Other risk factors identified include exposure to diethylstilbestrol in utero [13], exposure to other endocrine-disrupting chemicals (e.g., phthalates) [14], dietary consumption of red meat and trans fat [15] and lean body habitus [4]. Negative risk factors include multiparity, prolonged lactation and dietary modifications (e.g., increased intake of fresh fruits, green vegetables, long-chain omega-3 fatty acids) [15,16]. Interestingly, race/ethnicity plays a role; the prevalence of endometriosis is 40% lower in African-American and Hispanic women than in Caucasian and Asian women [17].
Clinical manifestations
Endometriosis is an inflammatory process that often manifests as chronic pain described as dull, throbbing, sharp or burning. Pain symptoms present as dysmenorrhea, dyspareunia, noncyclic lower abdominal/pelvic pain, back pain and/or pain at ovulation [3,18–20]. Chronic fatigue and irregular uterine bleeding are other associated symptoms [18]. Bowel and bladder involvement may result in cyclic dyschezia and dysuria, respectively [18]. In addition, endometriosis has a significant impact on fertility [21], but the mechanism(s) by which early-stage disease contributes to infertility are not well understood. The contributions of endometriosis to infertility are likely multifactorial, including impaired tubo-ovarian function, ovarian endometrioma, pelvic inflammation and adhesive disease impairing access of oocyte to fallopian tube, reduced oocyte quality and reduced endometrial receptivity to implantation [22–25]. Endometriosis is also associated with an increased prevalence of concurrent autoimmune diseases, including hypothyroidism, systemic lupus erythematous, rheumatoid arthritis and multiple sclerosis, as well as an increased risk for specific ovarian cancer subtypes (i.e., endometrioid and clear cell) and melanoma [26–28].
Theories regarding pathogenesis of endometriosis
Despite the prevalence of and public health burden attributable to endometriosis, the pathogenesis of this disease remains poorly understood. Multiple processes are likely responsible for the establishment and maintenance of endometriotic implants and for the associated symptomatology of the disease. These processes include angiogenesis (the formation of new blood vessels, supporting growth of ectopic endometrial tissue), cellular invasion, adhesion formation, fibrosis, neuronal infiltration and abnormal cell growth [19]. While current treatments aim at reducing symptomatology, elucidating the pathogenesis of endometriosis will allow for the development of more targeted therapy in the future. Several theories have been postulated to explain the pathogenesis of this disease. However, each individual theory fails to account for all types of endometriotic lesions, and are not mutually exclusive – therefore, multiple mechanisms are likely to be involved.
Sampson's theory of retrograde menstruation
The most widely accepted theory is Sampson's theory of retrograde menstruation, first described in 1922 [29,30]. This theory is supported by the finding that 75–90% of women with patent fallopian tubes have blood in the peritoneal cavity when undergoing laparoscopy at the time of menses [31]. In addition, women with congenital outflow tract obstruction, cervical stenosis or a uterine septum have a higher prevalence of endometriosis [9,32–34], lending further support for Sampson's theory. The propensity for implantation of ectopic endometrium in the posterior cul de sac [34] also supports retrograde menstruation as a plausible mechanism for establishment of disease. However, while most women have some degree of retrograde menstruation, only a small subset has endometriosis. This is likely because additional factors are required for the establishment and maintenance of endometriotic implants, such as cellular attachment, invasion and establishment of new blood vessels. Furthermore, retrograde menstruation cannot account for the observation of endometriotic lesions in sites distal from the pelvis, such as lung and brain [1], and therefore other mechanisms must play a role.
Coelomic metaplasia (metaplasia of peritoneal cells)
Meyer's theory of coelomic metaplasia postulates that cells of the visceral and parietal peritoneum undergo metaplastic change into endometriotic lesions [35]. Factors influencing this cellular transformation are not well understood. This theory is supported by a common embryonic lineage for both endometrium and peritoneum (i.e., coelomic wall). Although this theory is difficult to prove, it may at least in part account for rare cases of endometriosis in men, prepubescent girls, females lacking Müllerian structures and distant implantation sites [2].
Hematogenous/lymphatic dissemination of endometrial cells
Sampson also described the presence of disseminated endometriosis in which endometrial tissue, via hematogenous and/or lymphatic spread, implants in locations distal from the pelvis, including upper abdomen, brain, bone and pleura [1,36]. Evidence for lymphatic dissemination is supported by the finding of lymph node involvement in women with intestinal endometriosis undergoing rectosigmoid resection [37]. The demonstration of endometrial stromal cells within lymph nodes in a baboon model of endometriosis lends further support to this mechanism [38]. Evidence for hematogenous spread has been documented by the presence of endometrial cells in uterine vessels in patients with endometriosis [36]. Animal studies have shown injection of endometrial cells intravenously in rabbits resulted in distant pulmonary disease, further supporting hematogenous dissemination as a possible mechanism for disease pathogenesis [39]. However, although the theory of hematogenous/lymphatic spread may explain the presence of distally disseminated disease, it is likely not to be the primary mechanism of disease, given that distant lesions are rare.
Mullerianosis
The theory of Müllerianosis postulates that cells of Müllerian origin may be misplaced during organogenesis and induced by specific stimuli (e.g., estrogen, in utero diethylstilbestrol exposure) to form endometrial tissue in the peritoneal cavity [40,41]. Autopsy performed on five of 36 fetuses ranging from 14 weeks gestation to newborn have identified endometrial tissue in multiple extrauterine sites in the pelvis, suggesting that primitive endometrial cells may dislocate from the migrating fetal uterus during development [42]. The Müllerianosis theory accounts for endometriosis along the migration pathway of the embryonic Müllerian system as well as endometriosis in men, since initial female embryonic structures regress during male development [2]. This theory, however, is largely hypothetical and remains to be proven.
Immune
Multiple studies provide evidence for altered immune function in the pathogenesis of endometriosis. Increased survival and decreased clearance of ectopic endometrial cells has been attributed to a decrease in natural killer cell activity as well as to partial resistance of endometriotic cells to the action of natural killer cells [43]. Endometriotic cells may further thrive by recruitment of macrophages and other leukocytes to the peritoneum; these inflammatory cells produce cytokines and growth factors that facilitate proliferation of ectopic endometrial cells [44]. In vivo macrophage depletion studies by Bacci et al. [45] demonstrated that alternatively activated peritoneal macrophages (favoring a phenotype ‘permissive’ of disease) were required for growth and vascularization of ectopic endometrial lesions in a mouse model. A role for altered immune function in disease pathogenesis is also supported by the finding that autoimmune diseases are significantly more common in women with endometriosis than in the general population [26].
Stem cells
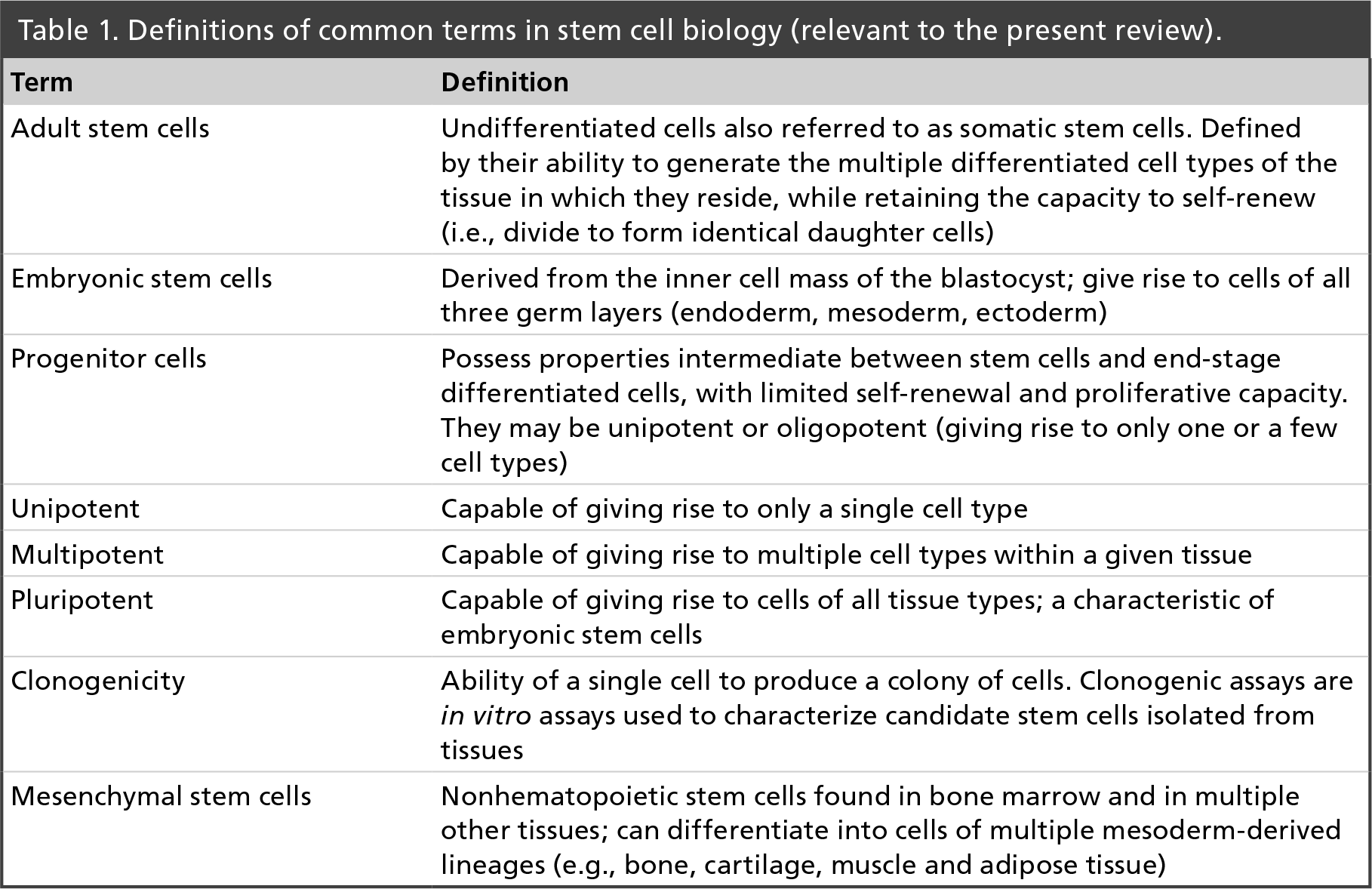
Mounting evidence over the course of the last decade supports the existence of an adult stem cell population in the endometrium [reviewed in 46–50] that provides a source of regenerative endometrial cells. These data have generated considerable interest in the potential role of adult stem cells in the pathogenesis of endometriosis. Adult stem cells are undifferentiated cells, defined by their ability to generate the multiple differentiated cell types of the tissue in which they reside, while retaining the capacity to self-renew [51–53]. Distinct from embryonic stem cells, which give rise to cells of all three germ layers (endoderm, mesoderm, ectoderm), adult stem cells are either unipotent (i.e., capable of giving rise to only a single cell type) or multipotent (i.e., capable of giving rise to multiple cell types within a given tissue) [49,54,55]. The differentiation potential (i.e., potency) of adult stem cells occurs along a continuum, and the ability to self-renew decreases with increasingly differentiated function, as a stem cell gives rise to tissue-specific, lineage-committed cells also referred to as ‘progenitor’ cells [49]. In general, the role of adult stem/progenitor cells is to maintain tissue homeostasis, providing replacement cells lost through cellular turnover and/or following tissue damage. Definitions of common terms used in stem cell biology that are relevant to this review are provided in Table 1.
Definitions of common terms in stem cell biology (relevant to the present review).
Now that an adult stem cell population has been identified in the endometrium, a more recent focus has turned to the possibility that endometriosis may be initiated by retrograde menstruation, or hematogenous/lymphatic spread, of this stem cell population. The concepts that endometriotic lesions may be clonal in origin [56–58], and that stem cells appear to be shed during menstruation [50,59,60], lend further support to the hypothesis that endometrial stem cells play a key role in initiating endometriotic lesions. Stem cells originating from the bone marrow also appear to play a role in disease pathogenesis [61,62]. A stem cell origin of endometriosis may be the common thread between multiple existing theories of pathogenesis, since endometriosis could arise from: retrograde menstruation of endometrial stem cells, hematogenous/lymphatic dissemination of endometrial or bone marrow-derived stem cells and/or stem cells persisting in Müllerian rests. However, the factors that regulate stem cell recruitment to ectopic sites, and/or survival and propagation of stem cells in endometriosis, remain to be determined.
Role for stem cells in regeneration of the endometrium
Endometrial regenerative function
The human endometrium is a remarkable tissue with vast regenerative capacity. It is comprised of two major zones:
The basalis, which remains intact, and is comprised of the basal region of the glands, stroma, supporting vasculature and lymphoid aggregates;
The functionalis, a transient layer containing glands extending from the surface epithelium as well as the supportive stroma.
The endometrium is absolutely unique in its ability to undergo the cyclic processes of cellular proliferation, differentiation, shedding and regeneration of the functionalis layer some 300–400-times during a woman's reproductive years. The endometrium has immense proliferative potential, amounting to as much as 7 mm of tissue growth in less than 14 days [63]. Cyclic regeneration of the functionalis requires repeated replenishment of all of its cellular compartments, including stromal cells, glandular and luminal epithelial cells and vascular endothelium. Given the requirement for rapid, repeated regeneration of the endometrium, it is not surprising that a resident stem/progenitor cell population has been demonstrated in human endometrium, which may provide a potential source of regenerative endometrial cells [46–50].
Evidence for the existence of stem cells in the endometrium
The demand for rapid, repeated tissue regeneration in the endometrium is similar to the cellular turnover required in other highly regenerative tissue types (skin, blood and intestinal epithelium), in which adult stem cell populations are crucial for physiologic tissue renewal and regeneration after injury [64–68]. In human endometrium, the basalis layer has been hypothesized to be the cellular source of the new functionalis layer produced in the subsequent cycle, harboring a resident stem/progenitor cell population responsible for the endometrium's regenerative capacity. The earliest evidence to support this hypothesis was provided by the studies of Padykula et al. [69,70], who demonstrated that the primate endometrium possessed a germinal cellular compartment localized to the lower basalis, in which high epithelial cell mitotic activity persisted after ovulation and menses. Of note, these studies were performed in a rhesus monkey model that has menstrual cycles identical to that of the human.
In general, the lack of distinguishing morphologic features and specific cell surface or cytoplasmic markers of adult stem cells makes it difficult to identify their location in a given tissue [49,51,55,71], and this holds true for endometrium. Thus, adult stem cells are classically defined by their characteristic functional properties of clonogenicity, proliferative potential, the capacity for unilineage and/or multilineage differentiation, and their ability to regenerate the tissue from which the stem cells are isolated [49,53,72,73]. To this end, the accumulating evidence which has provided indirect evidence for the existence of endometrial stem cells has done so by characterizing cell populations in the endometrium which exhibit the functional properties of stem cells.
Clonogenicity, defined as the ability of a single cell to produce a colony, was first demonstrated in human endometrium in 2004 [54], when Chan et al. isolated small populations of endometrial epithelial (0.22%) and stromal cells (1.25%) that possessed clonogenic activity. Later studies evaluated the in vitro capacity for uni- or multilineage differentiation, done by culturing candidate endometrial stem cells in differentiation-induction media, then analyzing the cells for phenotypic differentiation markers. Using this approach, multiple investigators demonstrated the capacity for candidate stem cells isolated from the endometrium to differentiate in vitro into multiple mature endometrial cell types [74–76], as well as the capacity to differentiate in vitro into cells of multiple mesoderm-derived lineages [76–78].
The most rigorous proof for the existence of stem cells in human endometrium is derived from in vivo xenotransplantation studies to determine whether candidate human endometrial stem cells can reconstitute mature, functional endometrial tissue when transplanted into immunodeficient mice [75,79–81]. Several investigators isolated candidate stem cells from human endometrium based on the expression of the ‘side population’ phenotype, an approach widely used to isolate adult stem cells from various mammalian tissues. Side population cells are defined by their ability to exclude the DNA-binding dye Hoechst 33342 via the expression of ATP-binding cassette transporter proteins [82]. Side population cells exhibit multiple properties of adult stem cells, including long-term proliferative potential and differentiation into mature tissue-specific cell types. After injecting human endometrial side population cells (i.e., candidate endometrial stem cells) into the subcutaneous tissue [79] or kidney capsule [75,80,81] of immunodeficient mice, these investigators demonstrated that human endometrial side population cells reconstituted mature, organized endometrial tissue, including stromal and glandular cells as well as mature blood vessels [75]. These in vivo studies provided strong support for adult stem cells in human endometrium that contribute to endometrial regeneration.
Source of endometrial stem cells: intrauterine versus extrauterine
A number of possibilities exist as to the origin of endometrial stem cells [2,48,83]: Endometrial stem cells may be derived from fetal stem cells, which arrive during embryonic development and remain in adult endometrium, continuing to replicate in adulthood; resident endometrial stem cells may arise from a circulating source such as bone marrow that seeds the endometrium periodically or in response to injury; or a combination of the above. It is now well recognized that bone marrow stem cells circulate and even give rise to mature, nonhematopoietic cell types of various mammalian tissues, including lung, liver, GI tract, skin, CNS and vascular endothelium [84–86]. Therefore, a number of investigators have sought to determine whether the bone marrow is a cellular source of endometrial cell types, thereby contributing to mechanisms of endometrial regeneration.
Four independent investigators have identified human endometrial stromal, glandular epithelial and/or endothelial cells of bone marrow origin in a total of 13 female recipients of bone marrow transplant from either HLA-mismatched [87] or male [88–90] donors. These very provocative studies support the ability of human bone marrow-derived stem cells to generate endometrial cells de novo. In addition, human bone marrow-derived mesenchymal stem cells (one of the two main bone marrow stem cell types) have the capacity to differentiate into endometrial decidual cells when exposed to 8-bromo-cyclic adenosine monophosphate, a potent decidualizing agent of human endometrial stromal cells [91]. This in vitro human data further support the concept of the bone marrow as a potential precursor of endometrial cells.
Evidence for a bone marrow origin of endometrial cells is also derived from murine bone marrow transplant studies. Our laboratory used a well-established murine bone marrow transplant model to test the hypothesis that the bone marrow is a source of precursors which give rise to murine endometrial cells [92]. This model uses bone marrow donors which ubiquitously express green fluorescent protein in all cells, allowing for clear-cut detection of endometrial cells of bone marrow origin in recipients of bone marrow transplant. Our studies provided definitive evidence that the bone marrow is a source of endometrial stromal compartment cells as early as 3 months post-transplant, and remains a long-term source of nonhematopoietic cells (negative for CD45, a panleukocyte marker) in the epithelial and stromal compartments at 12 months post-transplant, thereby supporting a role for the bone marrow in the long-term regeneration of endometrial stromal and epithelial cells. The eloquent studies of the Taylor laboratory further support a bone marrow origin for endometrial cells, demonstrating Y chromosome-positive endometrial epithelial and stromal cells in female recipients of bone marrow transplant from male donors [61,93,94]. Interestingly, these investigators also demonstrated that migration of bone marrow-derived stem cells to the murine endometrium in response to injury occurred to the same degree in the presence or absence of estrous cycles, suggesting that sex steroids are not required for the recruitment of bone marrow cells to the endometrium [94]. Further studies are required to elucidate the mechanisms regulating engraftment of the endometrium with bone marrow cells. In addition, whether or not the bone marrow contributes to the resident endometrial stem cell population remains unknown.
Stem cells & endometriosis
Identification of stem cell markers in human endometriotic tissues
A number of studies have sought to determine a role for stem cells in endometriosis by investigating whether any cells in the eutopic or ectopic endometrium of women with endometriosis express well-established markers of undifferentiated cells. One of the most widely studied stem cell markers, Oct-4, is a key transcription factor which regulates self-renewal and maintenance of an undifferentiated state in embryonic stem cells [95]. In addition to embryonic stem cells, there is increasing evidence that Oct-4 is expressed by rare populations of adult stem cells in various adult tissues, including human endometrium [96–100], further supporting the hypothesis that resident undifferentiated cells in the endometrium may provide a long-term source of tissue renewal. Several investigators have therefore evaluated expression of Oct-4 in human endometriotic tissues. Forte et al. [101] demonstrated Oct-4 expression in ectopic endometrial samples obtained from women with endometriosis, but a quantitative comparison of Oct-4 expression between eutopic and ectopic endometrial tissues from the women with disease, or with endometrium from women without disease, was not performed. Pacchiarotti et al. [102] compared Oct-4 expression in the eutopic and ectopic endometrium of women with severe endometriosis to expression in the endometrium of disease-free controls. The percentage of endometrial epithelial cells expressing Oct-4 was significantly higher in ectopic endometrial tissues (32.3%) than in eutopic endometrium from women with endometriosis (3.5%) or eutopic endometrium from disease-free controls (3.2%), supporting the concept that a population of undifferentiated, self-renewing cells play a role in the maintenance and survival of endometriotic lesions. Similarly, Chang et al. [103] demonstrated significantly higher Oct-4 mRNA expression in ectopic endometrial tissues than in eutopic endometrium and normal endometrium from disease-free controls. Interestingly, the same investigators demonstrated that higher Oct-4 mRNA expression levels in endometriotic tissues were positively correlated with several cellular migration-associated genes [103]. When manipulated to overexpress Oct-4, several human endometrial cell lines demonstrated significantly greater migration capacity in vitro, thereby suggesting a novel role for Oct-4 in the pathophysiology of ectopic endometrial growth by promoting endometrial cell migration [103].
Given that the exclusive expression of Oct-4 in stem cells has been challenged [104], the role of multiple other stem cell markers in endometriosis has been explored. Sox-2, another transcription factor responsible for maintaining pluripotency of undifferentiated embryonic stem cells, is expressed by a greater percentage of stromal cells in ectopic endometrial tissues than in secretory phase (but not proliferative phase) endometrium from disease-free controls [105]. Similarly, increased expression of Musashi-1 (RNA-binding protein associated with maintenance and asymmetric cell division of neural and epithelial progenitor cells) was demonstrated in endometriotic implants when compared with expression in secretory endometrium of normal subjects, but proliferative phase endometrium was not assessed in this comparison [106]. Expression of c-kit, a proto-oncogene and adult stem cell marker, is significantly higher in ectopic endometrial tissue than in either the eutopic endometrium of women with endometriosis or endometrium of healthy controls [102]. Expression of NANOG and SALL4, transcription factors involved in self-renewal of embryonic and hematopoietic stem cells, respectively, is higher in ectopic endometrium than in the endometrium of disease-free controls [101,103]. In summary, the work of multiple independent investigators demonstrates preferential expression of a number of well-established stem cell markers in ectopic lesions relative to eutopic endometrium. Collectively, these studies provide indirect evidence for a role for stem cells in the pathogenesis of endometriosis. They are limited, however, since the mechanism(s) by which any of these factors play a role in the disease process has not been determined.
Evidence for a functional role of stem cells in endometriosis
The identification of cells expressing phenotypic stem cell markers is not sufficient to demonstrate a functional role of stem cells in the pathophysiology of endometriosis. Stronger evidence is provided by the identification of cells within endometriotic tissues that exhibit the functional properties of stem cells.
In the endometrium, a specific population of stem cells, mesenchymal stem-like cells (MSCs), has been implicated to play a role in normal endometrial regeneration [76,107]. Mesenchymal stem cells are multipotent cells found in bone marrow and in multiple other tissues and have the ability to differentiate into cells of multiple mesoderm-derived lineages, such as bone, cartilage, muscle and adipose tissue [108]. Multipotent MSC-like cells which express the phenotypic (cell surface markers) and functional properties of bone marrow MSCs have been identified in human endometrium [76,109]. Thus, a functional role for these cells in the pathogenesis of endometriosis is now being explored. Kao et al. successfully isolated and characterized human endometrial MSCs from both eutopic endometrium and endometriotic implants [110]. Isolated MSCs from both compartments demonstrated multiple hallmark stem cell properties in vitro, including clonogenicity, proliferative capacity and the ability to differentiate into multiple mesodermal lineages. However, MSCs isolated from ectopic endometrium demonstrated higher in vitro migration capacity than those isolated from eutopic endometrium. In vivo mouse xenograft studies were then performed to compare properties of the human MSCs isolated from eutopic and ectopic endometrial tissues; endometriotic, but not eutopic, MSCs displayed extensive angiogenic and invasive properties after implantation into immunodeficient mice. Similarly, Moggio et al. [111] isolated MSCs from ovarian and peritoneal endometriotic implants and demonstrated increased proliferation, migration and angiogenic properties relative to MSCs from eutopic endometrium. These studies not only demonstrated the presence of MSCs in both endometriosis and eutopic endometrium, but also demonstrated characteristics unique to endometriotic MSCs that may contribute to abnormal cell migration, invasion and angiogenesis, key properties of endometriosis.
Chan et al. [112] also investigated stem cell function in human endometriosis, and identified a subset of epithelial and stromal cells isolated from human ovarian endometriomas that exhibited the stem cell properties of clonogenicity, self-renewal and multilineage differentiation, thus supporting a functional role for stem/progenitor cells in endometriosis.
Functional evidence for endometrial stem cells as a source of ectopic endometriotic lesions is further provided by the xenotransplantation studies described earlier in this review. Human endometrial stem cells (isolated on the basis of their ‘side population’ phenotype) have demonstrated the ability to reconstitute mature, organized endometrial stromal, glandular and vascular structures when injected into the kidney capsule or subcutaneous tissue of immunodeficient mice [75,79–81]. Elegant xenograft studies by Masuda et al. [113] demonstrated regeneration of a functional endometrium, including well-delineated stroma, glands and extensive neovascularization, from singly dispersed human endometrial cells transplanted under the kidney capsule of immunodeficient mice. These ectopic implants underwent hormone-dependent changes, including proliferation, differentiation and tissue breakdown in response to cyclic treatment with estrogen and progesterone. Since rodents do not develop spontaneous endometriosis, these xenograft studies represent artificial models of disease; nevertheless, such in vivo studies support the concept of an endometrial stem cell origin for endometriosis.
While the above studies provide compelling evidence for a functional role of stem cells in endometriosis, whether the contribution of stem cells differs with varying manifestations of disease remains unknown. For example, endometriosis can manifest clinically as peritoneal lesions that are red and cystic, black and puckered, or white and fibrotic in appearance. While some of the above-mentioned studies indicated the location of endometriotic lesion obtained (e.g., peritoneal, ovary) [101–113], the appearance and depth of lesions were not specified. In addition, though stem cells may provide a source of endometriotic cells, no studies to date have determined whether women with severe disease exhibit a higher stem cell burden within lesions, and/or a microenvironment within lesions which favors proliferation and differentiation of stem cells, to a greater extent than those with mild disease. Whether differences in disease manifestation and severity are in any way attributable to differences in stem cell number, function, location and/or microenvironment remains unknown.
Bone marrow stem cells as a source of endometriosis
Resident endometrial stem cells may be transported to ectopic extrauterine sites via retrograde menstruation, lymphatic/hematologic dissemination or a combination of both. Alternatively, stem cells contributing to endometriotic lesions may arise from an extrauterine source. Du et al. [61] tested this hypothesis in a novel murine model of endometriosis, in which wild-type murine endometrium was implanted into the peritoneal cavity of either hysterectomized transgenic LacZ mice, or hysterectomized wild-type recipient mice as controls. The finding of LacZ-positive cells in the ectopic endometrium of LacZ recipient mice indicated engraftment of endometriosis lesions with stem cells from an extrauterine source, since these cells could not have originated from wild-type transplanted uterine tissue.
What is a potential extrauterine source of stem cells engrafting endometriotic lesions? Since it is now established that: bone marrow-derived stem cells circulate and give rise to mature, differentiated nonhematopoietic cell types of various tissues [85,86], and bone marrow stem cells have the capacity to seed the endometrium and differentiate into mature endometrial cell types [61,87–90,92–94], the possibility that bone marrow stem cells can differentiate into ectopic endometrium has been explored in a murine model [62]. Sakr et al. [62] performed male-to-female murine bone marrow transplants, and implanted murine endometrium into the peritoneal cavity of the bone marrow recipients to create an experimental murine model of endometriosis. The investigators demonstrated engraftment of ectopic endometriotic implants with nonhematopoietic (CD45-negative), Y chromosome-positive bone marrow-derived cells, implicating the bone marrow as a source of nonhematopoietic stem cells contributing to endometriotic lesions.
The role of endothelial progenitor cells & vasculogenesis in endometriosis
While endometrial stem cells may be involved in the initial establishment of endometriotic lesions, maintenance of lesions is crucially dependent on the establishment of an adequate blood supply [114]. The creation of blood vessels occurs by two distinct processes: angiogenesis (the formation of microvessels from pre-existing ones) and vasculogenesis (de novo blood vessel formation via recruitment of endothelial progenitor cells [EPCs]) [115]. EPCs originate from multiple precursors, including hematopoietic stem cells, myeloid cells and multipotent bone marrow progenitors [116,117], and have been shown to contribute to the vascularization of endometriotic lesions [116,118]. Several factors regulate the mobilization of EPCs from the bone marrow, including VEGF, FGF-2 and estradiol [115]. Interestingly, VEGF and FGF-2 are upregulated in endometriosis, and the disease is known to be estrogen-dependent [119,120]. Mobilized EPCs, in turn, secrete angiogenic growth factors (e.g., VEGF and IL-8) to recruit mature endothelial cells, stimulate EPC proliferation and incorporate into newly forming microvessels [115,121]. Becker et al. demonstrated in an experimental murine endometriosis model that mice with endometriosis have elevated levels of peripheral blood EPCs compared with control mice, and that endothelial cells derived from the bone marrow were incorporated into the vasculature of ectopic endometrial lesions [118]. Furthermore, treatment with an angiogenesis inhibitor decreased circulating EPC levels and suppressed endometriotic growth [118]. This work further highlights an important role for stem/progenitor cells, specifically endothelial progenitors, in the establishment and maintenance of endometriosis, and supports the potential clinical use of antiangiogenic agents as a novel treatment option.
Conclusion
Endometriosis is a complex gynecologic condition affecting 6–10% of reproductive aged women. The pathogenesis of this disease is poorly understood and is likely multifactorial. Considerable evidence supports the existence of an adult stem cell population in the endometrium which provides a physiologic source of regenerative endometrial cells, and which may originate at least in part from the bone marrow. Multiple recent lines of evidence now suggest that stem cells of both uterine and extrauterine (bone marrow) origin contribute to the development of endometriosis. A stem cell origin of endometriosis may be the common thread between multiple existing theories of pathogenesis, since endometriosis could arise from: retrograde menstruation of endometrial stem cells, hematogenous/lymphatic dissemination of endometrial or extrauterine stem cells and/or stem cells in persistent Müllerian structures (Müllerian rests). In addition, it is well established that vascularization is required for the establishment and maintenance of endometriotic implants, a process in which endothelial progenitor cells may play an integral role. Thus, refining our understanding of the role stem/progenitor cells play in endometriosis, including the specific role of endothelial progenitors, may allow for a targeted and potentially more effective therapeutic approach to the management of this common and poorly understood disease.
Future perspective
Current medical management of endometriosis targets the disease's dependence on estrogen, and therefore relies on hormonal suppression. Unfortunately, medical treatment may fail to completely eliminate the disease, as not all endometriotic implants are sensitive to estrogen deprivation. This may, in part, be due to an insensitivity of the stem cells in endometriotic implants to hormonal deprivation [111]. Surgical management of endometriosis is also a mainstay of treatment but may also fail to identify and/or remove all lesions. The persistence of disease and/or recurrence of symptoms place a significant clinical burden on patients and on the healthcare system.
Mesenchymal stem cells isolated from normal endometrium and from endometriotic lesions lack estrogen receptor expression and therefore may not be targeted by therapies involving hormonal suppression [111]. Therefore, the development of novel agents to specifically target stem cells in endometriosis represents an exciting opportunity to address possible upstream mediators involved in the pathogenesis of this disease. However, additional research to elucidate the mechanisms by which stem cells contribute to endometriosis will be required. Targeting the stem cell population that establishes and/or sustains endometriotic implants may achieve eradication of endometriotic cells that are unresponsive to hormonal suppression.
Others have focused on targeting angiogenesis, since it is well established that the survival and invasive properties of endometriosis require angiogenesis, and that disruption of angiogenesis leads to necrosis of endometriotic lesions [110,122,123]. VEGF is an important pro-angiogenic factor in endometriosis and a target for novel therapies [124]. Treatment with sorafenib (BAY 43-9006), a VEGF receptor tyrosine kinase inhibitor, resulted in decreased proliferation and cell migration of MSCs isolated from ectopic endometrium, as well as a decrease in the size of endometriotic implants in rats with surgically-induced endometriosis [111,125]. Reduction in endometriotic lesions has similarly been observed in animal models with the use of bevacizumab (an anti-VEGF monoclonal antibody), SU6668 and SU5416 (tyrosine kinase inhibitors of VEGF receptor 2 [VEGF-R2]), overexpression of the angiogenesis inhibitor angiostatin and with cabergoline (dopamine agonist inhibiting VEGF-R2 phosphorylation) [125–129]. Given the critically important role of angiogenesis in endometriosis, more studies are needed to determine the safety and efficacy of treatment with antiangiogenic agents in humans for improved management of endometriosis. Since the majority of affected women are of reproductive age, a major challenge in the future development of antiangiogenic therapies will be to evaluate any potential long-term side effects on reproductive function (since reproduction requires physiologic angiogenesis at the level of the ovary and endometrium), and the risk of teratogenicity in case of pregnancy. The ability to target pathologic angiogenesis specific to endometriotic lesions would be ideal.
In addition to angiogenesis (i.e., development of new blood vessels from pre-existing ones), Laschke et al. [115,116] provide data that de novo generation of endothelial cells from endothelial progenitor cells (i.e., vasculogenesis) may be an important mechanism in the pathogenesis of endometriosis. Therefore, in addition to novel antiangiogenic therapies, the development of agents to target endothelial progenitor cell recruitment may be another effective way to block establishment of endometriosis. Further investigation to delineate the mechanisms that regulate recruitment of EPCs to endometriotic lesions will be required. Ultimately, the most effective therapeutic regimens will likely require a combination of therapies that eradicate hormonally responsive cells within existing lesions, and that target upstream mediators (including stem cells, endothelial progenitor cells and/or angiogenic factors) in the pathogenesis of disease (Figure 1).

Executive summary
Endometriosis affects 6–10% of reproductive aged women and up to 50% of women with pain and infertility.
The estimated healthcare costs for diagnosing and treating endometriosis in the USA was US$22 billion in 2002.
Endometriosis is an inflammatory disease that can manifest as dysmenorrhea, dyspareunia, noncyclic lower abdominal/pelvic pain, back pain, pain at ovulation, dyschezia, dysuria and/or infertility.
Multiple theories regarding the pathogenesis of endometriosis exist. These theories are not mutually exclusive, and multiple mechanisms likely play a role.
Sampson's theory of retrograde menstruation is the most widely accepted, but does not account for distant lesions, nor the fact that only a small percentage of women with retrograde menstruation will develop endometriosis.
Meyer's theory of coelomic metaplasia postulates that cells of the visceral and parietal peritoneum undergo metaplastic change into endometriotic lesions.
The theory of hematogenous/lymphatic spread of endometrial cells to ectopic locations may account for distant lesions.
The Müllerianosis theory postulates that misplaced cells of Müllerian origin may be induced by specific stimuli to form endometrial tissue in the peritoneal cavity.
Adult stem cells are undifferentiated cells, defined by their ability to generate the multiple differentiated cell types of the tissue in which they reside, while retaining the capacity to self-renew. In general, the role of adult stem/progenitor cells is to provide replacement cells lost through cellular turnover and/or following tissue damage.
Mounting evidence over the course of the last decade supports the existence of an adult stem cell population in the endometrium. Endometriosis may be initiated by retrograde menstruation, or hematogenous/lymphatic spread, of this stem cell population.
A stem cell origin of endometriosis could account for the observations that support multiple existing theories of pathogenesis.
Given the requirement for rapid, cyclic regeneration of the endometrium, it is not surprising that a resident stem/progenitor cell population has been demonstrated in human endometrium, which is a likely source of regenerative endometrial cells.
Evidence for the existence of endometrial stem cells is derived from the characterization of cells isolated from endometrium which exhibit the classic functional properties of stem cells: clonogenicity, proliferative capacity and unilineage and/or multilineage differentiation.
The most rigorous evidence supporting the existence of stem cells in human endometrium is derived from xenograft studies demonstrating that candidate human endometrial stem cells can reconstitute mature, functional endometrial tissue when transplanted into immunodeficient mice.
Adult stem cells in the endometrium may arise from an intrauterine or an extrauterine source, such as the bone marrow. Multiple human and murine studies have demonstrated the bone marrow as a source of precursors that give rise to multiple mature endometrial cell types.
Multiple well-established markers of undifferentiated cells, including Oct-4, Sox-2, Musashi-1, c-kit, NANOG and SALL4, are expressed to a greater degree in endometriotic lesions than in eutopic endometrium, thereby suggesting a role for stem cells in pathogenesis of the disease.
Mesenchymal stem cells isolated from human endometriotic lesions display extensive migration, angiogenic and invasive properties relative to those isolated from eutopic endometrium. These properties may at least in part underlie the pathogenesis of ectopic endometrial implants.
Xenograft studies demonstrating the ability of singly dispersed human endometrial cells to form organized, hormonally responsive ectopic endometrial implants in mice strongly support the concept of an endometrial stem cell origin for endometriosis.
Recent murine studies demonstrate that bone marrow-derived cells engraft endometriotic lesions; therefore the bone marrow may also be a source of stem cells that contribute to endometriosis.
While endometrial stem cells may contribute to the initiation of endometriotic lesions, the maintenance of lesions is crucially dependent on the establishment of an adequate blood supply. Endothelial progenitor cells (EPCs), which originate from hematopoietic stem cells, myeloid cells and multipotent bone marrow progenitors, have been shown to contribute to the vascularization of endometriotic lesions.
Current medical management of endometriosis involves hormonal suppression, but not all endometriotic cells are sensitive to estrogen deprivation. The development of novel agents to specifically target stem cells in endometriosis represents an exciting opportunity to address upstream mediators involved in the pathogenesis of this disease.
In addition, since establishment and survival of endometriotic lesions is critically dependent on angiogenesis, recent studies have tested multiple antiangiogenic agents in the treatment of endometriosis, and have demonstrated reduction of endometriotic implants in animal models.
The development of agents to target EPC recruitment may be another effective way to block establishment of endometriosis, but further studies to determine regulation of recruitment of EPCs to endometriotic lesions will first be required.
Ultimately, the most effective therapeutic regimens will likely require a combination of therapies that eradicate hormonally responsive cells within existing lesions, and that target upstream mediators (including stem cells, endothelial progenitor cells and/or angiogenic factors) in the pathogenesis of disease.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending or royalties.
No writing assistance was utilized in the production of this manuscript.