
Abstract
Background:
Dysmenorrhea (painful menstrual cramps) is one of the most common gynecological complaints in women and girls. Dysmenorrhea may be a condition itself or a result of another medical condition, including endometriosis and chronic pelvic pain. Research examining the relationship between menstrual pain ratings and catastrophizing has produced mixed results.
Objective:
To review and meta-analyze the relationship between catastrophizing and pain ratings of chronic cyclical pelvic pain.
Design:
Cross-sectional, longitudinal, and intervention studies that reported the relationship between menstrual/pelvic pain and catastrophizing were included. Study populations had to include healthy menstruating persons or persons with a condition associated with cyclical pelvic pain including primary dysmenorrhea, endometriosis, and/or chronic pelvic pain.
Data sources and methods:
A systematic search of articles published since 2012 on PubMed, PsychInfo, CINHAL, and Medline was conducted in January and rerun in November of 2022. Search terms included cyclical pelvic pain, dysmenorrhea, endometriosis, pelvic pain, and catastrophizing. Data extraction was completed independently by two extractors and cross-checked for errors. A random-effects meta-regression was used to synthesize the data using restricted maximum likelihood.
Results:
Twenty-five studies examining 4,540 participants were included. A random effects model found a meta-correlation between catastrophizing and pain of r = .31 (95% confidence interval: .23–.40) p < .001. Heterogeneity was large and significant (I2 = 84.5%, Q(24) = 155.16, p < .001). Studies that measured general pelvic pain rather than cyclical pelvic pain specifically and those that used multi-item rather than single-item measures of pain had significantly higher correlations. Age and depression did not moderate the relationship between catastrophizing and pain.
Conclusion:
A systematic review and meta-analysis found that catastrophizing had a small but significant positive association with pain ratings. Patients experiencing cyclical pelvic pain may benefit from interventions targeting the psychological management of pain.
Registration:
This meta-analysis was registered in PROSPERO on 14 January 2022. Registration number: CRD42022295328.
Plain Language Summary
Severity of period pain is associated with catastrophic thinking
Dysmenorrhea, known as menstrual cramps or period pain, is a common symptom and condition for women of reproductive age. Medical and surgical treatments often do not effectively reduce dysmenorrhea. Understanding the psychological processes that reinforce dysmenorrhea may help in developing better treatments. One important psychological process is catastrophizing, a thinking style in which people “catastrophize” or engage in negative thinking about how bad pain is or might become. In this study, we reviewed 25 studies of women with menstrual pain and statistically combined their results. We found that pain severity was significantly associated with higher catastrophizing. We also found that the association between pain and catastrophizing was higher in the studies that assessed general pelvic pain rather than cyclical pelvic pain specifically and those that used multi-item rather than single-item measures of pain. The relationship between pain and catastrophizing was not affected by diagnoses, age, or level of depression. Our results suggest a significant association between catastrophizing and menstrual pain ratings. Patients experiencing dysmenorrhea may benefit from interventions targeted at addressing catastrophizing.
Introduction
Dysmenorrhea (painful menstrual cramps) is one of the most common gynecological complaints in women and girls.1 –3 Among women of reproductive age, rates of dysmenorrhea range from 16% to 92%, whereas the prevalence of severe dysmenorrhea ranges from 2% to 29%. 4 Primary dysmenorrhea (PD) occurs in the absence of an identified organic disease, whereas secondary dysmenorrhea (SD) refers to cramps/pain attributed to an identifiable condition. 1 One common cause of SD is endometriosis, a chronic condition affecting 6% of women in the United States, over half of whom report struggling with menstrual pelvic pain/cramping. 5 Other conditions associated with SD include uterine fibroids (leiomyomas), adenomyosis, interstitial cystitis, chronic pelvic pain (CPP), and pelvic floor myalgia. 6 While dysmenorrhea is often associated with (and confused with) CPP, CPP is a broad chronic pain diagnosis that refers to both noncyclical pain (i.e. pain that is not dependent on the menstrual cycle) and persistent cyclical pelvic pain (i.e. pain due to endometriosis or dysmenorrhea). 7 As the primary aim of this meta-analysis is to examine the role of catastrophizing in chronic cyclical pelvic pain (CCPP), and given inconsistent definitions used in prior research, we included studies of individuals with primary and secondary dysmenorrhea and CPP (unless it was stated that individuals with dysmenorrhea or cyclical pain were excluded). Furthermore, for simplicity of reading, we refer to these studies as including individuals with CCPP.
Current medical and surgical management of CCPP is limited by side effects and nonresponse.8 –10 For example, a systematic review of clinical trials for the treatment of CCPP due to endometriosis found that 17%–34% of women experienced pain recurrence at follow-up time points. 8 Experiencing CCPP in adolescence and early adulthood is associated with developing chronic pain later in life; this, combined with existing treatment limitations, further underscores the necessity of developing effective treatments for the management of CCPP.11,12
One reason for the limited success of medical or surgical management of CCPP may be due to the failure of these treatments to address psychological factors that contribute to and maintain cyclical pelvic pain. Like many chronic pain conditions, there is a high comorbidity of CCPP and psychopathology, specifically depression.10,13,14 For instance, almost a third of women with CCPP due to endometriosis also meet the criteria for depression. 14 Despite this significant comorbidity and the existence of effective psychotherapy for many forms of chronic pain, 15 research examining psychological interventions for CCPP is lacking in quantity and quality.16,17 A systematic review of 11 studies of psychological interventions for CCPP due to endometriosis found that interventions containing mindfulness, psychoeducation, or cognitive behavioral therapy appear to be effective at improving both coping with pain and symptoms of depression and anxiety, but findings are limited by the small number of studies included and methodological concerns. 17 Another systematic review found only four studies of psychological or behavioral interventions for women with CCPP of unknown etiology, and the results of these interventions were inconclusive. 16 In one small open trial for patients with CCPP due to PD, Payne et al. implemented five sessions of mind-body and cognitive-behavioral group therapy (including one session on “automatic pain thoughts and de-catastrophizing”); patients showed significant reductions in menstrual pain and catastrophizing, suggesting that catastrophizing may be a mechanism for reducing CCPP. 18
Catastrophizing is defined as the tendency to “overestimate the likelihood of a negative event, and also believe that the negative event will be catastrophic.” 19 A form of negative repetitive thinking, catastrophizing is linked to rumination, magnification, and helplessness/hopelessness in response to negative stimuli. 20 Originally introduced as one of the cognitive distortions associated with depression, catastrophizing is significantly associated with perceived pain intensity and pain-related disability.21,22 Catastrophizing is one of the major mechanisms in psychological models of chronic pain. For example, the fear-avoidance model of chronic pain posits that maladaptive beliefs about pain, including catastrophizing, trap patients in a cycle of fear and avoidance that ultimately increases pain intensity and disability. 23 Alternatively, Petrini and Arendt-Nielsen hypothesize that catastrophizing may be understood as an inhibitory emotional regulatory process as defined under the Behavioral Inhibition and Activation Systems (BIS/BAS) model. 24 In this way, individuals engage in catastrophic thinking to avoid experiencing or managing pain. 24 Intervention research suggests that reductions in catastrophizing may precede reductions in pain and disability, further highlighting the clinical utility of addressing catastrophizing in chronic pain populations.25,26
Because CCPP involves repeated, unavoidable, and predictable pain, women with CCPP may engage in anticipatory catastrophic thinking as they approach their period; during their period, women may also catastrophize menstrual pain itself. Both anticipatory and concurrent catastrophizing likely lead to increased pain from menstrual cramps. Over a third (35%) of women with CCPP due to PD and 58% of women with CCPP due to endometriosis have clinical levels of catastrophizing (defined as a score of 30 or above on the Pain Catastrophizing Scale), suggesting that catastrophizing is a common maladaptive cognitive process in this population. 27 Some researchers, supported by neuroimaging and pain threshold findings, posit that repeated exposure to severe cyclical pelvic pain each month may lead to changes in the brain systems that process and cope with pain.28 –31 For example, women with CCPP due to dysmenorrhea compared to healthy controls showed altered central pain processing as evidenced by more sensitivity to thermal pain and increased activation of the entorhinal cortex, a region associated with the anticipation of pain.32,33 Evidence also suggests that engaging in catastrophic thinking may inhibit successful pain modulation, possibly by triggering anticipatory anxiety or increasing attention to painful stimuli.34,35 In further support of this anticipatory effect, women with severe CCPP have a stronger emotional reaction to menstrual-related words in a modified version of the Stroop task during the late luteal (premenstrual) phase compared to during the mid-follicular phase (after menstruation). 36 Thus, catastrophizing represents a critical mechanism through which women’s anticipation, expectation, attention, and worry about menstrual pain may be increased, potentially leading to increased experiences of pain.
Catastrophizing may also be a mechanism that explains the association between sexual trauma and dysmenorrhea. Women with a history of sexual assault are 1.60 times more likely to have pelvic pain and 1.20 times more likely to have dysmenorrhea compared to women with no history of sexual assault. 37 Sexual trauma may intensify the experience of cyclical pelvic pain because pain is localized to the pelvic and genital region, and this pain could serve as a reminder of the past traumatic experience.38,39 Women with a history of sexual trauma may catastrophize both their menstrual pain and their negative emotional reactions to and/or memories of trauma, creating a negative feedback loop that increases pain. 38
In addition to the role that it plays in exacerbating pain ratings, catastrophizing is also associated with the maintenance and exacerbation of depression, which, as previously mentioned, is common in patients with CCPP.10,13,14 In both nonpelvic chronic pain and CCPP samples, symptoms of depression are related to higher levels of catastrophizing, suggesting that the relationship between pain ratings and catastrophizing may be stronger in individuals experiencing depression.22,27
The present meta-analysis
While both theory and available data suggest a significant positive correlation between catastrophizing and CCPP, the magnitude of this relationship is unclear. A study of women with CCPP due to endometriosis found a correlation of r = .67, 40 whereas another study of women with CCPP due to CPP more broadly found a correlation of r = .52. 41 Other studies reported correlations closer to r = .30.42 –44 It is unclear if this variability in effect size is due to differences in study design, medical diagnosis examined, levels of depression, or other methodological differences such as the instrument used to assess pain or measure catastrophizing. Because CCPP is both a condition and a symptom of a wide variety of gynecological conditions, identifying which subpopulations have a stronger relationship between catastrophizing and pain ratings may improve recommendations for which patients would benefit from an intervention to address catastrophizing.6,45
Consequently, the present analysis is the first to directly examine the unique effects of catastrophizing on pain ratings in patients with CCPP. We also examine the extent to which this relationship is impacted by study methodology, medical diagnosis, age, depression, or history of sexual trauma.
Objectives
To calculate the meta-correlation between catastrophizing and pain severity ratings in women with CCPP. Hypothesis 1: We hypothesized that catastrophizing and pain severity would be significantly, positively related.
To examine if the relationship between catastrophizing and pain ratings was moderated by the instrument used to measure catastrophizing, measure of pain severity, medical diagnosis, and age. Hypothesis 2: We hypothesized that the relationship between catastrophizing and pain ratings would not be moderated by assessment instrument, pain, medical diagnosis, or age.
To test if the relationship between catastrophizing and pain severity ratings was moderated by levels of depression or history of sexual trauma. Hypothesis 3: We hypothesized that levels of depression and prior exposure to sexual trauma would moderate the relationship between catastrophizing and pain severity such that catastrophizing would be more strongly correlated with pain ratings in individuals with higher levels of depression and in those with a sexual trauma history.
Method
The following procedures were preregistered on PROSPERO in January 2022 (CRD42022295328) and follow PRISMA and MOOSE reporting guidelines.46,47 The PRISMA and MOOSE checklists can be found in supplemental materials.
Search strategy
A search of articles published after 2011 was conducted on PubMed, CINHAL, Medline, and PsychInfo in January and rerun in November of 2022. We used the following search terms to broadly capture articles addressing catastrophizing and CCPP: cyclical pelvic pain, dysmenorrhea, endometriosis, pelvic pain, and catastrophizing. A similar search strategy was used in a systematic review of treatments for CCPP. 48 Consistent with prior reviews and the age range for the prevalence of dysmenorrhea and CPP, we used an age range of 6–64.4,49 While there has yet to be a meta-analysis specifically evaluating catastrophizing and cyclical pelvic pain, a large systematic review published in 2006 identified psychosocial factors as important correlates of pelvic pain. 50 Later, review papers published in 2010–2011 identified psychological variables including catastrophizing as key mechanisms of pelvic pain.7,51,52 In addition, a prior meta-analysis of the association between PD and psychopathology indicated that only a minority of studies on PD were published prior to 2012. 13 Due to increasing emphasis on psychosocial factors in CPP after 2011, and the large literature captured in our search of reproductive health conditions, we limited our search to articles published in the last 10 years (2012 and later).
Study selection
Articles retrieved from the initial searches of all databases were compiled into Covidence, a web-based platform that streamlines the production of systematic reviews. 53 Two blind reviewers completed title/abstract and full-text reviews of articles to determine eligibility according to criteria. Disagreements were resolved by article discussion. Exclusion reasons were documented in Covidence.
Eligibility criteria
Inclusion and exclusion criteria are specified in Supplemental Document 1. Briefly, included studies had (1) samples of menstruating persons with CCPP or a condition known to cause cyclical menstrual pain (dysmenorrhea, endometriosis, adenomyosis, leiomyomata (fibroids), interstitial cystitis, CPP, and pelvic floor myalgia) and (2) measurement of both catastrophizing and pain. Conditions known to cause CCPP were taken from current guidelines for the differential diagnosis of secondary dysmenorrhea. 6 Because we planned to measure the impact of pain measurement and specific CCPP conditions on the relationship between catastrophizing and pain, we included studies that measured both specific cyclical pelvic pain and those that measured broader pelvic or urogenital pain. Healthy samples were included if they measured dysmenorrhea specifically.
Data extraction
Two independent reviewers double-entered study data regarding study design, location, participant demographics, methodology, and effect size estimates into a customized Qualtrics form. 54 Whenever possible, an article’s original sample descriptions were used (i.e. “women with Primary Dysmenorrhea” was coded as PD); if reviewers were unclear of the conditions specified, they also examined study descriptive data to determine if additional conditions were included in the sample. If articles reported on a longitudinal study, the correlation coefficient from the first timepoint was used. In case-control designs, the correlation within the cases relevant to the study was used. Whenever possible, the correlation between dysmenorrhea and catastrophizing was extracted. When not available, data from other pain measures were used (such as ratings of CPP). If multiple pain indices were reported, we used the scale with the highest reliability and validity (e.g. the Brief Pain Inventory compared to a single item VAS). If necessary, correlations for the catastrophizing subscales were averaged to create an effect size estimate for the total scale. If a study used only the pain subscale of a health-related quality of life (HRQOL) instrument, the sign of the correlation was inverted such that higher catastrophizing was related to worse pain-related HRQOL. Effect sizes were converted to Pearson’s r correlations using standard formulas for Spearman’s rho, 55 chi-square, 56 and odds ratios. 57 If an included study did not provide sufficient information for an effect size estimate, the corresponding author was contacted. If the author did not provide the necessary information prior to the completion of the review, the study was excluded due to lack of data availability.
Assessment of risk of bias
The Appraisal tool for Cross-Sectional Studies (AXIS), a 20-item critical appraisal tool, was used to evaluate the quality of each study. 58 Each study was evaluated by independent raters, and disagreements were processed identically to data extraction. Because current guidelines caution against using summary scores to rate study quality, we reported the ratings for each study on each of the 20 items. 59
Meta-analysis
Data analysis was conducted using the “meta” and “metafor” packages in RStudio (https://www.r-project.org). Meta-regressions used mixed effects models to estimate the meta-correlation between catastrophizing and pain rating.60,61 Our review used Pearson’s r correlation coefficient because it is the recommended approach for meta-analysis.60,61 Heterogeneity between the studies’ effect sizes was assessed using the Q and I statistics as well as by examining the forest plot. 62 We also created a funnel plot to evaluate for publication bias. For the meta-regressions with categorical moderators (i.e. medical condition, study design), a minimum of 10 studies per category was required.61,63 When less than 10 studies existed, a narrative review was conducted.
To conduct the moderation analyses on depression, the sample symptom mean was extracted from each study. However, because there was significant variability in instruments used for symptom measurement, mean values were converted to standardized scores using a common metric derived from an item response theory analysis. 64 A standardized metric is available for 11 depression instruments including the Beck Depression Inventory (BDI), Center for Epidemiologic Studies Depression Scale (CES-D), and Hospital Anxiety and Depression Scale (HADS). 64 Studies that used an instrument not included in the standardized metric were not included; a total of 10 studies were needed to conduct the meta-regression. As part of our narrative review, we documented if studies assessed anxiety symptoms to explore other potential moderators.
Results
A systematic search using PubMed, PsychInfo, CINHAL, and Medline yielded 9,294 studies. After removing duplicates, 4,838 studies were screened at title-abstract review, 947 were screened in full-text review, and 25 were included in the final analysis (see Figure 1 for PRISMA Diagram). Of the studies excluded at full-text review, 92% (N = 852) were excluded for not measuring catastrophizing, 3.6% (N = 33) were excluded for nonoriginal data (i.e. post hoc analyses of data already in the review), and 3% (N = 28) reported to measure both catastrophizing and pain but did not report sufficient data or respond to data inquiries. Finally, 0.7% (N = 6) of studies were excluded because their study population did not meet inclusion criteria, and 0.3% (N = 3) of studies were excluded for not measuring pain.

PRISMA flow diagram showing inclusion and exclusion of relevant studies.
Study characteristics
Descriptive information for each study is presented in Table 1 and summarized in Table 2. Most studies were observational (N = 16), followed by intervention (N = 8) and case-control designs (N = 1). Thirteen studies assessed general pelvic pain (using instruments such as the Brief Pain Inventory), whereas 12 studies specifically assessed cyclical pelvic pain (e.g. ratings of menstrual pain/cramps). Thus, we conducted two meta-analyses: 1) an overall correlation with all 25 studies and 2) a meta-correlation including studies of cyclical pelvic pain specifically. There was also significant heterogeneity in the diagnoses included in the samples of the studies; only five studies had a sample solely comprised of participants with PD; thus, we were unable to conduct a separate meta-correlation for these studies. However, 11 studies included participants with endometriosis, allowing for additional examination of this condition.
Summary of included studies.

CPP: chronic pelvic pain; N/A: not available; PD: primary dysmenorrhea; SD: standard deviation; BPI: Brief Pain Inventory; PCQ: Pain Catastrophizing Questionnaire; PCS: Pain Catastrophizing Scale; MPQ: McGill Pain Questionnaire; SF-Short Form; CSQ-C: Coping Strategies Questionnaire- Catastrophizing Subscale; NRS: Numeric Rating Scale; VAS: Visual Analogue Scale.
Study reported information for timing of assessment in relation to the menstrual cycle phase.
Study characteristics.

N = 25.
There was considerable variability regarding what measurement tools assessed pain ratings. Among the studies that used multi-item instruments, the most common was the Brief Pain Inventory (Table 2). Yosef et al. 43 described using a VAS CPP rating that participants “were asked to specifically differentiate from dysmenorrhea, deep or superficial dyspareunia, dyschezia, or back pain.” The data for dysmenorrhea specifically were not available. Excluding the above paper did not significantly impact the overall meta-correlation (r = .31 (95% confidence interval (CI): .22–.40), p < .001) I2 = 85.2%, Γ = .17, Tau 2 = .03, H = 2.60, Q(23) = 154.92, p < .001), thus we kept it in the analysis. Catastrophizing was most frequently measured by the pain catastrophizing scale (PCS, N = 19, Table 2).
Analysis of heterogeneity
A fixed-effects model demonstrated that there was considerable heterogeneity across all studies, I2 = 84.5%, Q(24) = 155.16, p < .0001, and H = 2.54. The forest plot (Figure 2) also demonstrated significant heterogeneity across studies. Thus, we conducted a random-effects model to estimate the meta-correlation and to account for this heterogeneity. 63 Significant heterogeneity was also observed in the fixed-effects model of the studies of cyclical pelvic pain (N = 12): I2 = 89.3%, Q(11) = 102.90, p < .0001, and H = 3.06.

Forest plot of all studies.
Meta-correlation
A random effects model found that the overall meta-correlation was r = .31 (95% CI: .23–.40), p < .001. The variance of the true effect size (Γ) 2 was. 03 and Γ was estimated to be .16, I2 = 84.5% and H = 2.54, Q(24) = 155.16, p < .001. Among those studies that specifically evaluated cyclical pelvic pain (N = 12), the meta-correlation was r = .21 (95% CI: .09–.33), p = .003. The variance of the true effect size (Γ) 2 was .03 and Γ was estimated to be .16, I2 = 89.3% and H = 3.06, Q(11) = 102.90, p < .001 (see Supplemental Figure 1 for a forest plot of this meta-correlation).
Moderation analyses
We first explored if the relationship between catastrophizing and pain ratings was moderated by differences in the measurement of pain and/or measurement of catastrophizing. Because 76% of studies used the PCS, there was not enough variability in measures to test whether the instrument for assessing catastrophizing moderated the relationship between catastrophizing and pain ratings. Eleven studies used multi-item scales to measure pain and fourteen used a single-item instrument. Studies that used multi-item instruments had a higher correlation between pain and catastrophizing (r = .44) than studies that used a single-item instrument measure of pain (r = .24, Qm(1,23) = 8.19, p = .01; Table 3). Measurement differences accounted for 31% of the variance in effect sizes. All the studies that evaluated ratings of cyclical pelvic pain specifically (and all of the studies that examined specifically PD) used single-item measures. Studies that measured general pelvic pain had higher correlations between pain and catastrophizing (r = .43) than those that measured cyclical pelvic pain specifically (r = .22, Qm(1,23) = 11.05, p < 01; Table 3). Measurement of cyclical pelvic pain versus general CPP accounted for 34% of the variance in effect size, and the cyclical pelvic pain-specific correlation was significant (p = .003).
Tests of moderation.

CI: confidence interval; b: meta-regression coefficient for continuous moderators; k: # of studies; r: meta correlation.
As expected, many studies assessed women with a variety of medical conditions including PD, urologic CPP syndrome, and endometriosis (see Table 1). Because endometriosis is a leading cause of CCPP, we examined whether the correlation between catastrophizing and pain was different for samples that included individuals with endometriosis compared to those that did not; the moderation analysis was not significant (Qm(1,23) = 1.76, p = .20, Table 3). There was also no significant effect of the average age of the sample on the relationship between pain ratings and catastrophizing (b = .01, SE = .01; Qm(1,21) = 2.30, p = .14; Table 3).
Nine studies had sufficient data to convert average depression levels to a standardized metric and examine the impact of depression on the relationship between catastrophizing and CCPP (Supplemental Table 1). Although analyses required ten studies for adequate power, we conducted exploratory moderation analyses to see whether existent studies suggested a need to control for depression; the moderation was not significant (b = −.003, SE = .02; Qm (1,7) = .04, p = .85; Table 3).
History of sexual trauma was assessed in only three studies, all of which used different definitions of sexual trauma.41,43,80 Although not enough studies existed for analysis, our narrative review found that the presence of childhood and adult sexual trauma was positively associated with pain severity in two studies,43,80 and that those with “major” childhood sexual abuse had significantly higher pain catastrophizing levels than those with no abuse or “mild” abuse history. 41
Finally, while many studies assessed anxiety (Supplemental Table 2), they used noncomparable measures, thus preventing a moderation analysis using anxiety scores. In our narrative review, we observed that higher anxiety scores were significantly associated with both higher catastrophizing and pain ratings in nearly all studies (Supplemental Table 2). In addition, as shown in Table 1, only 44% of articles (11/25) reported data on participants’ use of contraceptives, with many of the 11 studies simply limiting their samples to participants not on contraceptives.
Publication bias and study quality assessment
Examination of the funnel plot (Figure 3) indicated a relatively symmetrical distribution of the effect sizes, and Egger’s regression test of asymmetry was not significant (t = .19, df(22), p = .85), suggesting that the results of this meta-analysis were not substantially impacted by publication bias.
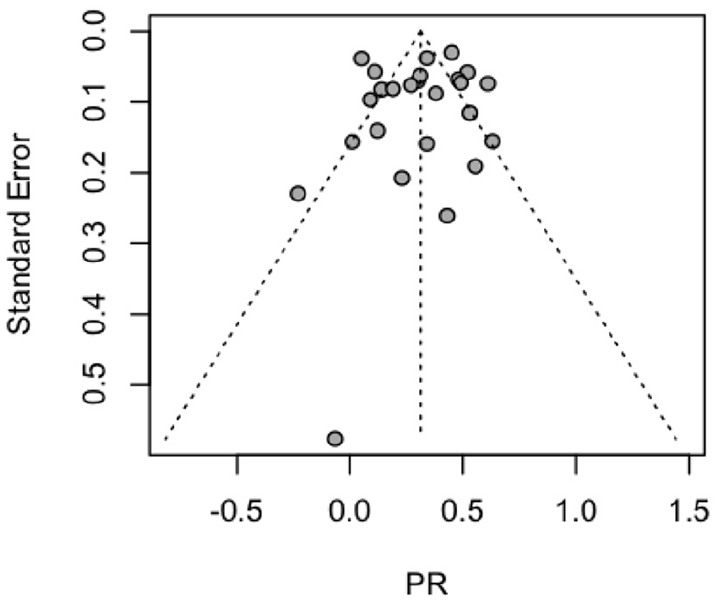
Funnel plot.
AXIS ratings for each study are presented in Supplemental Table 3. Very few studies conducted either an a priori or post hoc power analysis. Furthermore, as can be seen in Table 1, many studies had small sample sizes which are susceptible to bias. Most studies were also conducted in English-speaking countries and findings may differ in other regions. Furthermore, few studies characterized participant refusals or missing data which may pose a risk of bias. Some studies were missing basic data including demographics and descriptive statistics, limiting the utility and generalizability of those studies. Finally, most studies recruited convenience samples receiving outpatient gynecological services which may limit the generalizability of results to populations who are unable to obtain specialized medical care. However, the predominance of heterogeneous clinical samples suggests that these results would be relevant to gynecologists and other providers in outpatient settings.
Discussion
The meta-correlation between catastrophizing and pain ratings was r = .31 (p < .001), although there was significant heterogeneity across studies; 84.5% of the variability in the effect sizes was due to between-study variability, which is considered a high level of heterogeneity. 84 There were higher correlations between pain and catastrophizing among studies that measured general pelvic pain (r = .43) versus cyclical pelvic pain specifically (r = .22), and those that used multi-item (r = .43) rather than single-item measures of pain (r = .24). Average age and depression scores did not moderate the relationship between catastrophizing and pain.
Despite the prevalence of cyclical pelvic pain as a primary complaint and symptom across many reproductive health conditions, only 12 studies (48%) measured cyclical pelvic (i.e. menstrual) pain specifically, and only five studies had samples composed solely of participants with PD. While the heterogeneity of conditions in the studies reviewed is not surprising given that CCPP is both a condition itself and a common symptom of many gynecological, urological, and gastrointestinal conditions,6,45 our review indicates a substantial need for more research into the relationship between catastrophizing and cyclical pelvic pain. The correlation between catastrophizing and cyclical pelvic pain (r = .21) was lower than the correlation between catastrophizing and pain in studies that assessed general pelvic pain (r = .43), perhaps suggesting that the cyclical pelvic pain samples lowered the overall meta-correlation (r = .31). While the magnitude of our correlations is small, it is consistent a prior meta-analysis of 49 studies which found that the correlation between general chronic pain intensity and catastrophizing was r = .29 (95% CI: .25–.32). 22 While some studies reported when (in the menstrual cycle) the assessment was conducted, we were not able to explore this as a possible moderator; it is likely that women who were menstruating during the time of assessment may have rated pain and catastrophizing differently than participants who were retrospectively responding. Despite these limitations, the correlation between catastrophizing and cyclical pelvic pain was still significant, providing justification for future investigation of this topic with better methodology.
The observed correlation between pain ratings and catastrophizing was significant and consistent in magnitude with other meta-analyses of adults experiencing pain. 22 However, the relatively small correlation may be explained by a number of variables including measurement variability, the use of single-item pain measurements, and potential conceptual overlap of pain and catastrophizing scales. Measurement variability accounted for the largest percentage in effect size variability and may have affected the overall correlation The relationship between catastrophizing and pain was significantly lower in studies with single-item assessments than studies that used multi-item indices. The Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) recommends single-item numerical rating scales for the measurement of pain intensity while more comprehensive measures are recommended for assessing “pain interference” 85 ; for this reason, pain catastrophizing may have a stronger relationship to pain interference than pain intensity. However, five of the 11 multi-item studies used the pain severity subscale of the Brief Pain Inventory which is an average rating of pain severity at its worst, least, average, and current level, a subscale that may produce similar results as single-item measures of pain.86,87 It is also possible that the difference between single- and multi-item correlations is a statistical artifact rather than a reflection of true differences in the relationship between catastrophizing and pain because single-item pain ratings produce less variability than multi-item scales. 88 Alternatively, there is conceptual overlap between measures of pain interference and catastrophizing which may have inflated the correlation for some studies. For example, the total score of the McGill Pain Questionnaire used in three studies included four questions assessing the “affective” component of pain where individuals rate the extent to which their pain is “fearful,” “punishing-cruel,” “tiring-exhausting,” or “sickening.” 89 These items are likely highly related to catastrophizing due to their similarity to anxiety, hopelessness, and helplessness. Nevertheless, we found that both the single- and multi-item pain scales were significantly correlated with catastrophizing, which suggests a robust association.
Unexpectedly, depression did not moderate the relationship between catastrophizing and pain ratings. This may be due to small sample size or range restriction; the standardized values of average depression scores ranged from 57.1 to 67.8 units, which limited the ability to detect moderation. However, the average depression scores included in our analyses are above the standardized population average for this metric (M = 50, SD = 10). 64 Therefore, our nonsignificant interaction term indicates that catastrophizing impacts pain ratings similarly for populations at varying levels of moderate-to-severe depression. Our findings further suggest that catastrophizing is a useful treatment target even in patients with higher levels of depression.13,14
The current review found only three studies that met our inclusion criteria and evaluated trauma history. Two studies reported that sexual trauma was associated with increased pain severity and one study found that child sexual abuse was linked to higher catastrophizing levels, suggesting that those with a sexual trauma history may have a stronger relationship between catastrophizing and pain.41,43,80 Given the increasing calls for trauma-informed reproductive health care and the impact that trauma has on psychological mechanisms of pain, this review highlights a major absence of trauma-informed research on CCPP.38,90
Strengths and limitations
To our knowledge, this is the first meta-analysis of the relationship between catastrophizing and CCPP. Our review searched four large databases, used a comprehensive definition of CCPP, and examined critical moderators. While there is a significant range in the observed effect sizes, this is likely reflective of the heterogeneous clinical population with CCPP.6,45 In addition, small sample sizes for the moderation analyses may have limited statistical power to detect effects. Future research would benefit from the inclusion of instruments to measure psychopathology and trauma exposure to examine these factors in more depth. Furthermore, we were unable to account for the effects of contraceptive use because the majority of studies did not provide information on contraceptive use in their samples. Also, because the majority (75%) of studies used the PCS, we were unable to explore if the instrument used to measure catastrophizing was a significant moderator. While the PCS remains a common and clinically relevant instrument in chronic pain research and practice, theoretical and empirical work has begun to question the extent to which the PCS accurately captures catastrophic thinking processes as well as the construct validity of catastrophizing in general.20,24,91,92 Future research would benefit from improved measurement of catastrophizing and other cognitive distortions.
Conclusion
In summary, we found that, among women with CCPP, the overall correlation between pain ratings and catastrophizing was r = .31 and this relationship was consistent across differences in medical diagnosis, age, and level of depression. Because CCPP may be a risk factor for the development of future chronic pain disorders, addressing the link between catastrophizing and CCPP may not only reduce menstrual pain but also the likelihood of a chronic pain condition later in life.12,93
Future research would benefit from improved assessment of catastrophizing, pain, history of sexual trauma, and psychopathology. In addition, research could examine the feasibility, efficacy, and scalability of mental health interventions that address catastrophizing and may reduce CCPP such as psychoeducation classes 94 or brief smart-phone-delivered interventions. 95 Overall, our results reiterate the impact that mental health variables have on CCPP, adding to the growing evidence for integrated behavioral and reproductive health care. 96
Supplemental Material
sj-doc-1-whe-10.1177_17455057231199949 – Supplemental material for The role of catastrophizing in chronic cyclical pelvic pain: A systematic review and meta-analysis
Supplemental material, sj-doc-1-whe-10.1177_17455057231199949 for The role of catastrophizing in chronic cyclical pelvic pain: A systematic review and meta-analysis by Emily P Rabinowitz, MacKenzie A Sayer and Douglas L Delahanty in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231199949 – Supplemental material for The role of catastrophizing in chronic cyclical pelvic pain: A systematic review and meta-analysis
Supplemental material, sj-docx-2-whe-10.1177_17455057231199949 for The role of catastrophizing in chronic cyclical pelvic pain: A systematic review and meta-analysis by Emily P Rabinowitz, MacKenzie A Sayer and Douglas L Delahanty in Women’s Health
Supplemental Material
sj-docx-4-whe-10.1177_17455057231199949 – Supplemental material for The role of catastrophizing in chronic cyclical pelvic pain: A systematic review and meta-analysis
Supplemental material, sj-docx-4-whe-10.1177_17455057231199949 for The role of catastrophizing in chronic cyclical pelvic pain: A systematic review and meta-analysis by Emily P Rabinowitz, MacKenzie A Sayer and Douglas L Delahanty in Women’s Health
Supplemental Material
sj-docx-5-whe-10.1177_17455057231199949 – Supplemental material for The role of catastrophizing in chronic cyclical pelvic pain: A systematic review and meta-analysis
Supplemental material, sj-docx-5-whe-10.1177_17455057231199949 for The role of catastrophizing in chronic cyclical pelvic pain: A systematic review and meta-analysis by Emily P Rabinowitz, MacKenzie A Sayer and Douglas L Delahanty in Women’s Health
Supplemental Material
sj-docx-6-whe-10.1177_17455057231199949 – Supplemental material for The role of catastrophizing in chronic cyclical pelvic pain: A systematic review and meta-analysis
Supplemental material, sj-docx-6-whe-10.1177_17455057231199949 for The role of catastrophizing in chronic cyclical pelvic pain: A systematic review and meta-analysis by Emily P Rabinowitz, MacKenzie A Sayer and Douglas L Delahanty in Women’s Health
Supplemental Material
sj-jpg-3-whe-10.1177_17455057231199949 – Supplemental material for The role of catastrophizing in chronic cyclical pelvic pain: A systematic review and meta-analysis
Supplemental material, sj-jpg-3-whe-10.1177_17455057231199949 for The role of catastrophizing in chronic cyclical pelvic pain: A systematic review and meta-analysis by Emily P Rabinowitz, MacKenzie A Sayer and Douglas L Delahanty in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.