
Abstract
The study compared ultrasound and ambulatorial hysteroscopy as diagnostic methods detecting endometrial polyps in postmenopause women. 281 women aged 41–82 years who underwent ambulatorial hysteroscopy were analyzed for presence of uterine bleeding and/or altered transvaginal ultrasound (endometrial thickness ≥5 mm). Ultrasonography detected endometrial polyps in 22.8% of patients and endometrial thickening in the other 59.8%. Hysteroscopy diagnosed endometrial polyps in 80.8%. Ultrasonography showed sensitivity of 88.7%, specificity of 25.4%, positive predictive value of 81.7%, negative predictive value of 37.5% and accuracy of 75.4% in diagnosing endometrial polyps. Hysteroscopy showed 96.4% sensitivity, 74.6% specificity, 93.4% positive predictive value, 84.6% negative predictive value and 91.8% accuracy. Hysteroscopy demonstrated more accuracy than ultrasonography, which is not sufficient for accurate diagnosis.
A progressive increase in the incidence of endometrial polyps has been observed with advancing age, being more common among postmenopausal women [1,2]. Other risk factors have also been identified such as late menopause, obesity, hypertension and the use of hormones [3].
Currently, the most appropriate investigative method available for evaluating the uterine cavity in women with endometrial thickening, either asymptomatic or with vaginal bleeding, is the hysteroscopy [4], considered by many authors as the ‘gold standard’ for evaluation of the endometrium.
Ambulatorial hysteroscopy is a procedure to evaluate abnormalities of the endometrial cavity and has a high success rate. It is advisable to always perform with a biopsy if the endometrial cavity measured by ultrasonography is greater than 5 mm, and also in the case of any suspected malignancy, even when there is a normal uterine cavity in hysteroscopy [5].
When comparing hysteroscopy and transvaginal ultrasonography with pathological findings, it is conclusive that they are both complimentary methods in the diagnosis of uterine intracavitary lesions.
In conclusion, this study aims to evaluate the accuracy of transvaginal ultrasonography and ambulatorial hysteroscopy in the diagnosis of endometrial polyps in postmenopausal women.
Methods
Into a retrospective study, data were obtained through the consultation records of 323 postmenopausal women undergoing ultrasonography and hysteroscopy (Bettocchi) with endometrial biopsy (directed by hysteroscopy). The study included 281 postmenopausal women, characterized by the presence of at least 1 year of amenorrhea and follicle-stimulating hormonal levels of at least 30 mU/ml, aged 41–82 years old, who had undergone ambulatorial hysteroscopy for submitting uterine bleeding and/or transvaginal ultrasound (endometrial echo greater than or equal to 5 mm), and for these reasons, were referred to the outpatient hysteroscopy. Some of these women are users of combined hormone therapy or tamoxifen (treatment for breast cancer). The transvaginal ultrasound was performed using the Toshiba model SAL 38B with a 5 MHz transducer and image-type mechanical sector. The measurement of endometrial thickness was taken in the longitudinal plane at its thickest point. It encompassed both layers of the endometrium and myometrium was taken from the inner edge of the anterior and posterior walls of the uterus including the uterine cavity. In our country, ultrasonography is routinely performed on women approximately once a year. 42 women were excluded because they had already had records with missing or incomplete reports of transvaginal ultrasonography and diagnostic hysteroscopy, and the absence of anatomopathological results. Demographic data, clinical characteristics, justifications for hysteroscopy and sonographic, hysteroscopic and anatomopathologic finds, were reported as mean, standard deviation, absolute (n) and relative (%) frequency. The performance of tests (ultrasonography and hysteroscopy) was assessed by sensitivity, specificity, positive predictive value, negative predictive value and accuracy, as well as confidence intervals of 95%. Comparison of tests in terms of sensitivity and specificity was carried out by the comparison of percentages by chi-square (χ2) test, and accuracy through the Z-test for proportions. The significance level was 5%. The software used for analysis was SAS version 9.1.
Results
The mean age of patients was 61.3 with a standard deviation of 7.6 years. Out of these patients, 27.6% had diabetes mellitus Type 2, 70.5% had hypertensions and 5.7% were smokers. The average BMI was 31.6 with a standard deviation of 5.8 kg/m2 (minimum of 22.51 kg/m2 and maximum of 54.10 kg/m2). Out of these patients, a further 73% were multiparous (with three or more births). The average time after menopause was 10.7 with a standard deviation of 7.7 years (minimum of 1 year and a maximum of 37 years) with 15.3% of the patients being users of combined hormone therapy. It was also observed that 6.8% were in treatment for breast cancer with tamoxifen. Table 1 shows the reasons for performing a hysteroscopy and the ultrasonographic findings that were obtained. It was observed that via ultrasound, an endometrial polyp was detected in 22.8% of patients. The ultrasonographic diagnoses showed endometrial thickening (EE) in 59.8% of the patients, being an average of 10.5 mm with a standard deviation of 5.5 mm (minimum of 1 mm and a maximum of 32 mm).
Clinical indications of ambulatorial hysteroscopy and ultrasonographic findings for the group of women in the study.

Considered as endometrial polyps for the performance valuation of ultrasonography
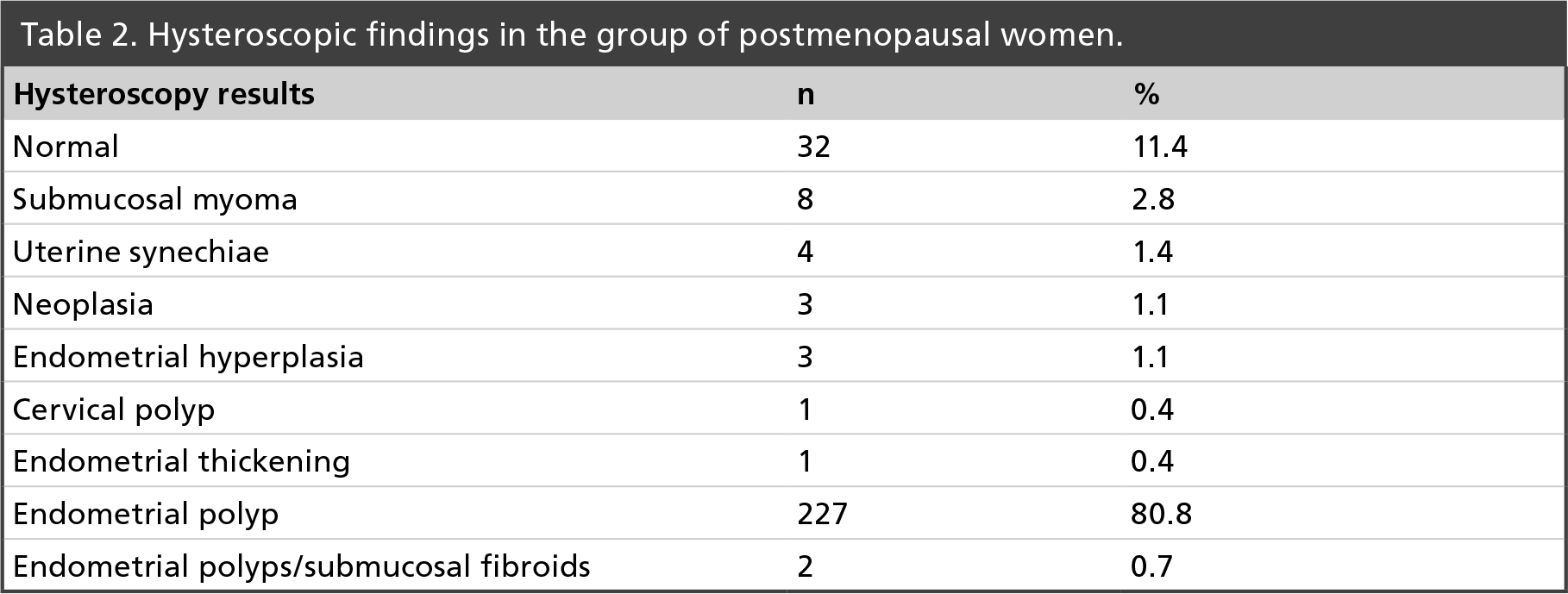
The hysteroscopy diagnosed endometrial polyps in 80.8% of patients. Other hysteroscopy diagnostics are described in Table 2.
Hysteroscopic findings in the group of postmenopausal women.
Histopathological examinations confirmed the presence of 79% of endometrial polyps and 21% of nonendometrial polyps (other findings) Table 3.
Pathological diagnosis in the study group.

Accuracy of ultrasonography and hysteroscopy in the diagnosis of endometrial polyps of postmenopausal patients.

HSC: Hysteroscopy; NPV: Negative predictive value; PPV: Positive predictive value; USG: Ultrasonography
Ultrasonography showed high sensitivity and low specificity, with an accuracy of 75.4%, whereas hysteroscopy showed high sensitivity and high specificity, with an accuracy of 91.8%. The results of the diagnostic tests are shown in Tab l e 4. The difference in sensitivity, specificity and accuracy of the values observed in ultrasonography and hysteroscopy was statistically significant (p < 0.0022, p < 0.0001, p < 0.0001, respectively).
Discussion
Studies have demonstrated prevalence greater than 40% of polyps in women with postmenopausal bleeding [6,7]. Ben Arie et al. found endometrial polyps in 54.9% of asymptomatic patients, and uterine bleeding in 45.1% [8]. Accordingly, we observed the prevalence of endometrial polyps in 79% of postmenopausal women. In the Orvieto study [9], 65% of women were diagnosed with endometrial polyps after routine ultrasonographic examinations, while 23% demonstrated an image suggestive of endometrial polyps, and 75% were presented with an irregular/thick endometrium. In our study, there were patients with uterine bleeding and asymptomatic ones, being that 22.8% of them had an image suggestive of endometrial polyps, and 59.8% had endometrial thickening.
It was observed that ambulatorial hysteroscopy was sufficient in diagnosing 96.4% of endometrial polyps. Other authors, in studies of a smaller sample using the same technique, diagnosed 42.1% (n = 51) of endometrial polyps [4]. Cacciatore et al. [10] while studying post-menopausal women with uterine bleeding (n = 45) diagnosed 42.2% (n = 19). The difference can be explained by the higher number of women included in our study.
There was evidence of endometrial polyps in 222 patients in the anatomopathologic exam. In turn, the hysteroscopy method showed a suggestive image of polyps in 229 patients. In this sense, the disagreement between the hysteroscopic image and the anatomopathological result shows that even when hysteroscopy is done by an expert, there was the possibility of a diagnostic error. In the Campaner et al. study [4] which evaluated 51 women with endometrial polyp by hysteroscopy, histological confirmation occurred in 30 cases, which partially corroborates with our results.
In a retrospective study covering 223 post-menopausal women, Kelekci [11] observed sensitivity in the ultrasonography for the diagnosis of endometrial polyps in 72% of patients, with specificity in 50.8%, while in the hysteroscopy the sensitivity was 94.4% and the specificity was 58.6%. Towbin et al. [12] observed a sensitivity of 54 and 79% as well as a specificity of 90 and 93% for ultrasonography and hysteroscopy, respectively.
In our study, ultrasonography had a sensitivity of 88.7% and specificity of 25.4%. With hysteroscopy, we obtained a sensitivity of 96.4% and a specificity of 74.6%. This difference is most likely due to ultrasonography and hysteroscopy being performed by different professionals. The diagnosis of endometrial polyps is strongly influenced by the diagnostic method used and the experience of the operating professional [8].
Yela et al. [13] demonstrated that ultrasonography and hysteroscopy showed an accuracy of 61.2 and 73.1% for the diagnosis of endometrial polyps, respectively. Arbozi et al. showed 60% accuracy with ultrasonography, [14] and Kelekci et al. [11] demonstrated 65.8% accuracy with ultrasonography and 95% with hysteroscopy. Accordingly, our results also showed that diagnostic accuracy of ultrasonography was worse in comparison with hysteroscopy for the diagnosis of endometrial polyps. We never use ultrasonography as a single diagnostic method for endometrial polyps; we always perform an ambulatorial hysteroscopy to assure proper diagnosis.
In summary, the higher accuracy rate for hysteroscopy, when compared with ultrasonography in the diagnosis of endometrial polyps in postmenopausal women, shows that sonographic evaluation may fail to identify the endometrial lesion. The cavity evaluation through direct viewing is still a predominant element in the diagnosis of endometrial polyps. On the other hand, it is not possible to ensure the precise diagnosis of endometrial polyps by only using the ultrasonographic image.
Future perspective
With new ultrasound techniques, such as the 3D ultrasonography and the hysterosonography, they will be able to distinguish the conditions that lead to the thickening of the endometrium specifically polyps. This will aggregate even more information for the conventional ultrasonography.
Executive summary
Endometrial polyps are common in postmenopausal women, and are often described as a thickening of the endometrium during routine transvaginal ultrasonography.
Since most polyps are benign, a surgical approach is not always necessary. Given this, ultrasonography has the potential to be an important tool in the accurate diagnosis of endometrial polyps, and thus avoids the need of surgical procedures (i.e., hysteroscopy) for confirmation.
Ultrasonography fails to predict the diagnosis of endometrial polyps in postmenopausal women. Its use does not exempt the role of the hysteroscopy in confirming this pathological condition.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending or royalties.
No writing assistance was utilized in the production of this manuscript.
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or anima experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.