
Abstract
Most women with Turner syndrome (TS) are infertile due to primary ovarian failure. However, approximately 5% experience spontaneous pregnancy, and recently, more women with TS have used assisted reproductive technology with donated oocytes (ART-OD) to become pregnant. The first generation of Turner patients undergoing ART-OD demonstrated a high rate of fatal aortic dissection in late pregnancy or postpartum. More recent observations, particularly from Nordic countries, suggest a lesser risk of dissection, but confirm a high rate of pre-eclampsia in ART-OD pregnancies. This article reviews publications since 2000 concerning maternal outcomes for pregnancies in women with TS to determine if specific risk factors such as type of pregnancy, age, or presence of underlying congenital cardiovascular disease may identify women at special risk.
Keywords
Genetic origins
Turner syndrome (TS) is a relatively common genetic disorder affecting 1/2500 live-born females [1]. The diagnosis may be made as a result of cardiovascular defects including hypoplastic left heart, aortic coarctation or aortic valve disease presenting during gestation or in the early postnatal period. More commonly, TS is diagnosed during evaluation for short stature often with primary amenorrhea in girls aged 10–16 years [2]. It is caused by complete or partial monosomy for an X chromosome, which occurs most commonly as a result of sex chromosome nondisjunction or fragmentation during gametogenesis. The most prevalent Turner karyotype is 45,X (Figure 1), resulting from union of a gamete with a single normal X and another missing a sex chromosome altogether (monosomy for a Y chromosome in nonviable). The most common Turner karyotype containing a fragmentary X chromosome is 46,X,iso(X). The isoX chromosome results from faulty meiotic recombination events involving pericentromeric repetitive sequences, leading to deletion of most of the short arm and duplication of the long arm. Other meiotic errors may result in deletion of the X chromosome short arm with preservation of Xq (46,X,del[X]p) or deletion of terminal portions of both Xp and Xq, with fusion of the broken ends to form a ring X chromosome (46,X,r[X]). In all these cases, significant portions of the X chromosome short arm (Xp) are deleted. Structurally abnormal chromosomes are often lost during mitotic cell divisions during fetal development, so that many individuals with TS have a mosaic karyotype including cells with the original fragmentary X chromosomal together with 45,X cells resulting in a karyotype denoted 46,X, i(X)/45,X, in the case of an iso-X chromosome. The Turner phenotype is not ameliorated by this type of mosaicism, since all cells are haploinsufficient for major parts or all of the second sex chromosome.
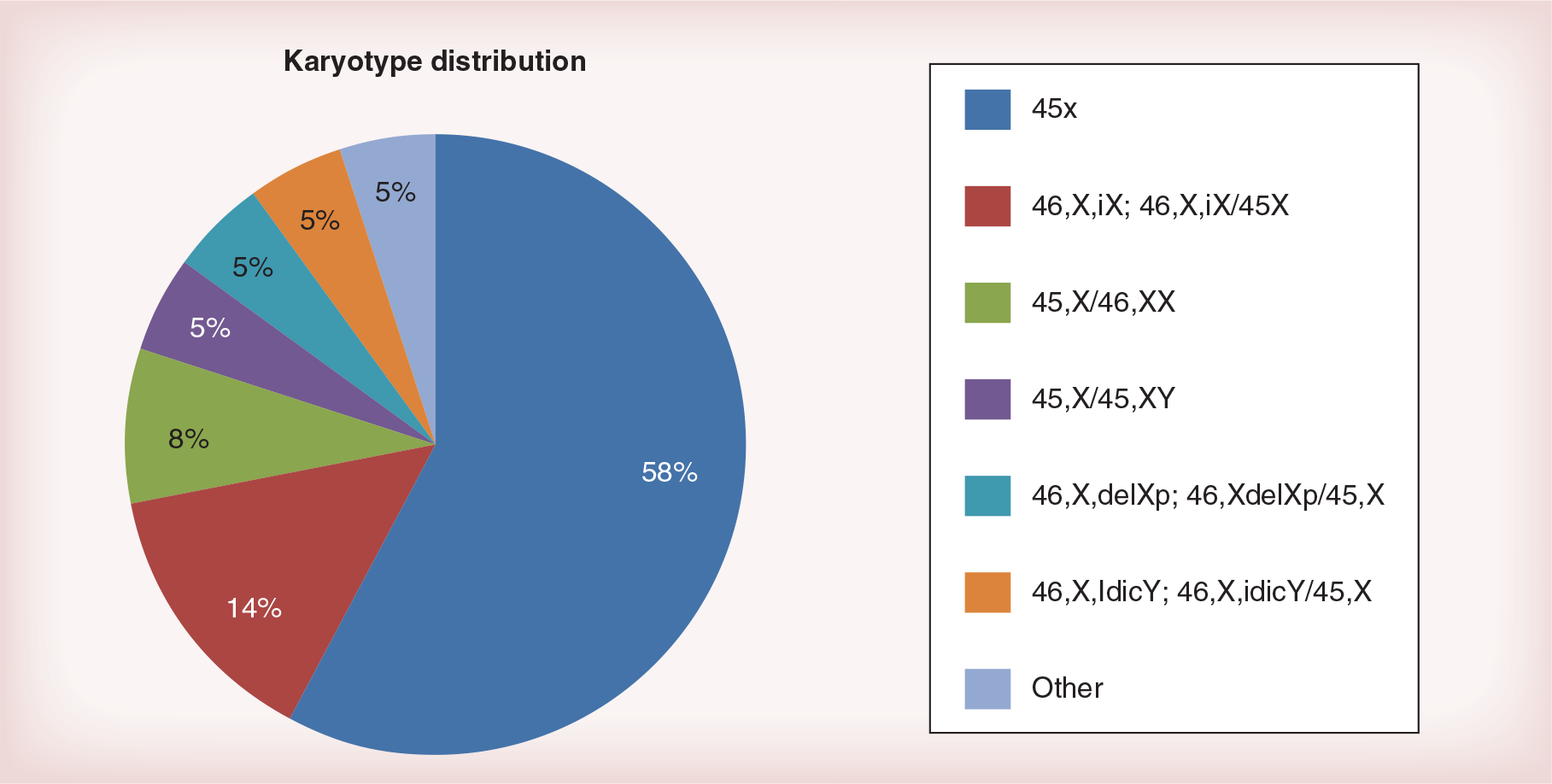
Major karyotype groups found among 400 girls and women with Turner syndrome participating in the NIH natural history study.
Loss of a sex chromosome in the developing embryo due to mitotic nondisjunction may also cause TS, with 45,X cells associated with variable proportions of 46,XX,47,XXX or 46,XY cell lines (Figure 1). Mosaicism for 46,XX, 47,XXX and 46,XY cells will ameliorate the phenotype depending on the relative abundance and tissue-specific expression of the different cell lines.
The short stature, congenital cardiovascular defects and neurocognitive traits seen in TS are all linked to deletion of X or Y chromosome short arms [3–5]. The short arm terminal regions of both X and Y chromosomes contain a series of homologous genes that escape X-inactivation, and allow meiotic pairing and recombination between the sex chromosomes, termed pseudoautosomal regions. Haploinsufficiency for the pseudoautosomal gene termed SHOX is responsible for the short stature characteristic of TS. The genes related to cardiovascular and cognitive effects also map to the sex chromosome short arms, but have not been identified. By contrast, the X chromosome locus responsible for primary ovarian insufficiency in TS remains elusive. Ovarian failure occurs with high frequency in women missing the entire second sex chromosome and in women missing only the short arm with normal Xq complement (46,X,delXp) or extra copies of Xq (46,X,isoXq), suggesting an ovary critical locus on Xp. However, women with Xq deletions in the presence of normal Xp complement also have infertility, suggesting that it is not haploinsufficiency for any specific X chromosome locus that determines ovarian insufficiency [6].
Primary ovarian insufficiency
Early studies of ovarian pathology in women with TS described fibrous streaks devoid of oocytes and follicles and thus initially it seemed that gonads failed to develop or were ‘dysgenetic’. Subsequent studies in 45,X fetuses revealed that early stages of ovarian development appeared normal, with expected numbers of oocytes and primordial follicles at 14–16 weeks of gestation [7]. However, at later stages of development, Turner ovaries were relatively depleted of oocytes and have few developing follicles, suggesting an accelerated rate of oocyte demise and follicular atresia [8,9] although follicles in various stages of development are detected in some teenage girls with TS [10]. The cause(s) for the high rate of oocyte attrition in most girls with TS is unknown. It has been suggested that aneuploidy per se contributes to oocyte demise due to meiotic mishaps [11].
A large, multicenter Italian study including more than 500 girls with TS reported that spontaneous puberty occurs in about 15% of those with pure 45,X and in 30% of girls with a second cell line with more than one X chromosome (i.e., 45X/46XX; 45X/47XXX)b [12]. Puberty fails to progress to menarche in some girls, and menarche may be followed by oligomenorrhea and/or anovulatory cycles in others, so that only about 5% of young women with TS maintain normal menstrual cycles by 20 years of age. Potential for spontaneous puberty and fertility may be difficult to assess among girls with TS. An important Swedish study using ovarian biopsy has shown similar results to the Italian findings above, that a karyotype with mosaicism for 45,X and 46,XX or 47,XXX cell lines is the most significant positive predictive factor for the presence of ovarian follicles, while karyotypes indicating nonmosaic 45,X or structural that defects of one X chromosome predict the absence of viable ovarian follicles [13]. Clinical factors such as normal FSH and AMH levels and spontaneous start of puberty were also significant positive predictors of follicle presence, although less robust than the blood karyotype [13].
Aortic disease in TS
While short stature and ovarian insufficiency are the best known features of TS, complications of congenital cardiovascular disease are the leading cause of morbidity and premature mortality [14–16]. The aortic valve is congenitally abnormal in approximately 33% of girls with TS, but is not detected in many individuals until complications occur due to inadequate screening [17–19]. Structural aortic valve abnormality and aortic coarctation are linked to aortic pathology, or aortopathy, with increased risk for aortic dilation, dissection and rupture [19–26]. The degree of dilation is greatest in patients with abnormal aortic valve function [18,24], but may be present in individuals with normal valve function as well and in some Turner patients that have an apparently normal aortic valve and normal blood pressure [18,24]. Thus it remains unclear whether Turner women without apparent congenital cardiovascular anomaly may be at risk for aortic disease during pregnancy.
The risk for aortic aneurysm formation, dissection and rupture is increased by 100-fold among women with TS compared with the general female population. Moreover, the typical age of dissection in TS is 35, compared with 75 for the female population [23]. Aortic valve abnormalities and aortic coarctation, with or without surgical repair, are an important predisposing factor. Hypertension is a risk factor for aortic disease in the general population as well as in TS. The presence of aortic dilation is a clear risk factor for aortic dissection in TS, and thus direct measurements of aortic root and ascending aortic diameters should be normalized to body surface area and monitored over time [27]. Pregnancy imposes increased stress on the aorta, and even normal multiparous women have dilated ascending aorta compared with age-matched controls that have not borne children [28]. Moreover, pregnancy-related hypertension such as pre-eclampsia may directly promote vascular damage, aneurysm formation and, if not controlled, lead to aortic rupture. Thus it seems quite likely that pregnancy may pose exceptional risks for women with TS. The remainder of this article reviews data published since the year 2000 relevant to this concern.
Spontaneous pregnancies
Spontaneous pregnancy occurs in 2–8% of women with TS [12,29–31]. There have been 138 such pregnancies reported in the medical literature since 1960. Spontaneous pregnancies are more common in women mosaic for cell lines containing two of more X chromosomes in addition to 45,X, but there are several well-documented cases of pure 45,X women having multiple natural pregnancies [30,32,33]. Women with TS may form some normal oocytes containing their single normal X and some abnormal oocytes missing the X chromosome, or containing a fragmentary X in the case of women with karyotypes such as 46,X,iXq. Thus there is a fairly significant chance that a mother with TS will conceive a child with TS, and given that most TS gestations do not survive, spontaneous abortions occur with increased frequency in spontaneous Turner pregnancies. There have been occasional reports of newborns with cerebral palsy, cleft palate and club foot, although these features are not associated with TS. A large, population-based study performed in Sweden examined 202 infants born to TS women and found the prevalence of birth defects was similar to the reference population [34].
No maternal fatalities have been reported in spontaneous pregnancies among women with TS. There was one well-documented aortic dissection that occurred during the second natural pregnancy of a Swedish woman not known to have TS prior to her pregnancy [35]; fortunately the dissection was treated surgically and a healthy child delivered by C-section. She later had a surgical resection of aortic coarctation and associated aneurysm. To this reviewer's knowledge, there have been no other cases of aortic dissection in spontaneous Turner pregnancy. Severe pregnancy-associated hypertension does not seem to be increased in spontaneous pregnancies [30,36]. The characteristics of spontaneous pregnancies are compared with those of assisted reproductive technology with donated oocytes (ART-OD) in Table 1.
Overview of pregnancies among women with Turner syndrome.
These data represent the total number of pregnancies described in case reports and case series since 1960. Where patients initially reports as case reports were later reported as part of a series, they were only counted once.
This dissection is the same case reported in the ‘Spontaneous’ series.
AoDis; Aortic dissection or rupture; ART-OD: Assisted reproductive technology with donated oocytes; HTN: Severe hypertension associated with pre-eclampsia.
Assisted reproductive technology pregnancies with oocyte donation
Case reports of Turner women experiencing catastrophic aortic complications in ART-OD pregnancies began appearing in the late 1990s (reviewed in [37,43]). More recently, several case series of ART-OD outcomes in women with TS have been published including a total of 240 patients (Table 2). These studies report an extraordinary high rate of pregnancy-related hypertension associated with preterm delivery and low-birth weight babies [30,38,39,41]. There were two maternal deaths resulting from aortic dissection (both in the French series) and one nonfatal dissection in the Nordic series. Thus, the frequency of aortic dissection during an ART-OD pregnancy in TS is estimated at 1.25% or one case per 125 full-term pregnancies. The frequency of maternal deaths based on these series is approximately 0.8% (two per 240 pregnancies).
Series reporting oocyte donation pregnancy maternal outcomes.
AoDis; Aortic dissection or rupture; HTN: Severe hypertension associated with pre-eclampsia.
It appears from these data that severe HTN is significantly more prevalent among Turner women undergoing ART-OD compared with those with spontaneous pregnancy. There are several potential explanations for the disparity, which is also seen in ART-OD pregnancies in non-Turner women [43]. Women with spontaneous pregnancies are typically younger (less than 30 years of age) and may be less severely affected by TS; mosaicism for normal 46XX cell lines may contribute to fertility and to healthy vascular physiology. It is also possible that the high dose hormonal treatments necessary to prepare the womb for successful implantation/gestation trigger adverse vascular responses in women with TS that have intrinsic vascular dysfunction and a high prevalence of idiopathic HTN. Finally, it is possible that complications of spontaneous TS pregnancies are under-reported, with unrecognized women ‘flying under the radar’ in community clinics.
It has been widely quoted over the past decade that Turner women undergoing ART-OD face a 2% risk of death from aortic dissection. This estimate originated from a survey conducted by Karnis et al. in 2001 [44] that queried 258 donor egg programs in the USA regarding their experience with donated oocyte (OD) pregnancies in women with TS. Approximately a half the programs responded, reporting 101 pregnancies and 94 live births [44]. There were no deaths or dissections among treated TS patients; although one Turner patient died from aortic rupture while awaiting treatment. The authors assumed that the TS pregnancy rate was similar in clinics that did not respond to the survey and thus that there were approximately 200 ART-OD pregnancies among women with TS treated in the USA during this period [44]. Since there were case reports of four deaths from aortic dissection occurring in Turner ART-OD pregnancies published 1997–2001 in the USA, the authors used these four cases as the numerator over their estimated 200 TS OD pregnancies over this period (4/200 = 2%).
This estimate was born out in a multicenter retrospective analysis of the French experience with OD pregnancies in TS [38]. Chevalier et al. analyzed the materno-fetal outcomes for 93 pregnancies among patients with TS treated between 1991 and 2009 (Table 2). They reported two patients that died during the 38th week of pregnancy due to aortic dissection or rupture [38]. Most recently, a relatively large Nordic cohort study evaluated obstetric and neonatal outcomes among 106 women with TS who delivered after OD [39]. While the prevalence of pregnancy related hypertension was very high and similar to earlier studies (Table 2), there were no maternal deaths and fewer neonatal complications such as preterm delivery or low birth weight compared with the French experience. The authors describe several potentially life-threatening maternal complications, including a nonfatal aortic dissection occurring in the context of severe pre-eclampsia, a patient who developed mild tricuspid and mitral valve regurgitation, and patients with HELLP syndrome and postpartum hemorrhage necessitating hysterectomy [39].
The more favorable results for mothers and offspring in this most recent study may be due to advent of better cardiovascular screening for older girls and young women with TS [45]. The overall, averaged mortality rate for all published series is less than 1% (Table 2), and this risk may be further reduced in the future as women are more rigorously screened for cardiovascular disease prior to pregnancy, and are protected by continued cardiac surveillance during pregnancy and aggressive treatment of HTN.
Parenting choices & outcomes among women with TS
Two recent studies have investigated parenting choices made by women with TS. A total of 432 women attending Swedish University based Turner Clinics were investigated concerning obstetric histories; 57 [12%] had experienced one or more pregnancies with a live-born rate of 54% in 124 pregnancies [36]. Spontaneous pregnancies occurred in 40%, mostly in women with mosaicism for 46,XX cells. ART-OD pregnancy was achieved by 60%. The miscarriage rate for the spontaneous group was 45%, approximately twofold higher than in the OD group. There were no maternal deaths in either group. Obstetric history was also examined in 276 women older than 25 years participating in the NIH natural history study [30]. Ten women had a total 14 live births; 50% were spontaneous conceptions and 50% via OD. Only one patient experienced significant complications; she had a twin pregnancy via OD with pre-eclampsia necessitating preterm delivery. She demonstrated marked dilation of the ascending aorta a few years after delivery when first evaluated at NIH. She had no prepregnancy aortic assessment, so we could only speculate that the twin pregnancy may have caused the aneurysm. She declined surgery to repair the aneurysm, but fortunately her ascending aortic diameter has remained rock stable for nearly 15 years of follow-up. This case serves to direct attention to potential delayed adverse consequences for Turner women that have experienced pregnancy.
Morbidity & mortality years after childbirth
There has been only one study to-date addressing the impact of pregnancy on morbidity and mortality in the years after childbirth [42]. This population-based registry study compared health statistics for 124 women with TS who gave birth between 1973 and 2010 to a group of age-matched Turner women that had never given birth (n = 378). There were no deaths recorded for the childbirth group while 14 (3.7%) of the no-childbirth group had died, over a median 10-year follow-up. Five of these women died of aortic dissection at ages 25–37 years. The prevalence of aortic aneurysm was similar in the two groups; HTN and ischemic heart disease were actually more common in the nonchildbearing group. The authors point out as a caveat that the women in the child-bearing group were likely healthier than those without childbirth to start with, and that longer duration of follow-up is necessary to capture differences in rare events [42]. However, these observations are somewhat reassuring that pregnancy and childbirth do not have dramatic adverse effects on the cardiovascular health of women with TS. They also remind us that young women with TS are at high risk for aortic catastrophe quite independently of pregnancy.
Current guidelines for OD in TS
The American Society for Reproductive Medicine currently views TS as relative contraindication for OD pregnancy [46]. Prior to considering pregnancy, the patient with TS needs a comprehensive cardiovascular evaluation with MRI visualizing the entire thoracic aorta and aortic valve, supervised by a cardiologist familiar with congenital heart disease. Several French Academic Medical Societies led by the French College of Obstetricians and Gynecologists have issued similar practice guidelines [47]. The French have also clearly shown that evaluation by community cardiologists unfamiliar with TS is frequently inadequate and may miss important defects that would preclude OD pregnancy. According to the American Society for Reproductive Medicine, any aortic valve abnormality, aortic dilation/aneurysm or coarctation constitutes an absolute contraindication. Even if the cardiovascular system appears normal, women with TS still have excess risk for gestational diabetes and pre-eclampsia due to underlying, preexisting glucose intolerance and prehypertension, and should be classified as high-risk pregnancies. Finally, all authorities agree that careful ongoing monitoring is required during pregnancy for women with TS, including cardiac ultrasound or MRI to monitor aortic diameter [43,46,47].
Conclusion
Women with TS are at risk for aortic disease including aneurysm, rupture or dissection occurring during young adult years. This risk is greatest in women with defective cardiovascular development signaled by bicuspid aortic valve, aortic dilation and/or coarctation. Pregnancy exerts significant stress on the heart and aorta, and thus women with cardiovascular anomalies associated with TS should be advised to avoid pregnancy and to consider adoption or surrogacy. Older girls and young women with potential fertility need cardiovascular screening and counseling about the risks of unintended pregnancy. Women with potential fertility have the right to pursue natural reproduction, but need close medical supervision and monitoring of the aorta during pregnancy. ART with OD should be restricted to women with normal cardiovascular system. Only one embryo should be transferred, and continued cardiologic follow-up is required throughout pregnancy.
Future perspective
It is essential to educate the medical community on the need to use more advanced screening methods to detect asymptomatic congenital cardiovascular defects in women with TS contemplating pregnancy. Concomitant efforts are needed to educate women about risks associated with natural and ART-OD pregnancies in TS. All nations need to keep registries on the outcomes of natural and ART-OD pregnancies, with specific regard to the presence of pre-existing cardiovascular defects related to outcome. Absent in this information, at present we do not know if Turner women who have completely normal cardiovascular evaluation may safely proceed with natural or assisted pregnancy. We also need longitudinal follow-up of Turner women who have undergone spontaneous or ART-OD pregnancies in comparison to a control group of Turner women who have not been pregnant, which will resolve the question of ultimate safety of pregnancy for women with TS that appear free for congenital cardiovascular disease. Finally, new therapies aimed to prevent pre-eclampsia hold promise for improving outcomes for high-risk patients [48].
Financial & competing interests disclosure
C Bondy is retired and holds volunteer status as scientist emeritus at NICHD. The author has no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Executive summary
Premature ovarian insufficiency: over 90% of women with Turner syndrome (TS) experience early depletion of ovarian follicles resulting in infertility.
Aortic disease: approximately 50% of women with TS have congenital aortic valve defects, aortic dilation or coarctation that put them at high risk of aortic catastrophe during pregnancy. These defects are often not detected by clinical exam or routine echocardiography so that comprehensive cardiovascular screening requires MRI.
Spontaneous pregnancies may occur in approximately 10% of women with TS. While more common in women with mosaicism for cells with more than one X chromosome, it may also occur in apparently pure 45,X patients.
The risk for aortic dissection in assisted reproductive technology with donated oocyte pregnancies among Turner women has been estimated at 2%, but may be decreasing due to screening out patients with preexisting aortic defects, and restriction to single embryo transfers.
It remains to be determined whether women with no evidence of cardiovascular defect after comprehensive evaluation have any increased risk for vascular complications of pregnancy.