
Abstract
Contrast-enhanced dual-energy mammography (CEDM) is a promising new breast imaging tool for breast cancer detection. In CEDM, an iodine-based contrast agent is intravenously administered and subsequently, dual-energy mammography is performed. This results in a set of images containing both a regular mammogram and an image that contains contrast enhancement information. Preliminary studies have indicated that CEDM is superior to conventional mammography and might even match the diagnostic performance of breast MRI. In this review, the imaging technique, protocol and patient handling of CEDM is presented. Furthermore, an overview of current results on CEDM and potential future indications are outlined.
Background
Breast cancer is an important cancer-related cause of death in women [1]. In breast cancer, mammography plays a pivotal role in cancer detection and follow-up, despite the availability of various other breast imaging modalities, such as ultrasound and breast MRI.
One of the most important limitations of mammography is that its diagnostic performance depends heavily on breast density [2]. To overcome this limitation, new techniques are being developed that were not feasible in the analogue era. One of these techniques is the use of iodinated contrast agents in (contrast-enhanced) mammography. Several approaches in contrast-enhanced mammography have been studied in the past few years [3], and all of these showed promising feasibility results for breast cancer detection. Of these various techniques, contrast-enhanced spectral mammography, also known as contrast-enhanced dual-energy mammography (CEDM), became commercially available some years ago and seems to be the most promising approach for routine clinical use.
The use of contrast agents in cancer detection is based on the phenomenon that neoplasms induce angiogenesis for further tumor growth. However, these new vessels are rapidly formed and as a result, they are ‘leaky’. Contrast agents can pass through these vessel walls into the (tumor) interstitium, causing enhancement. For breast cancer, this principle is well-known in breast MRI and has helped to increase sensitivity and specificity for breast cancer detection [4].
In this review, the imaging technique, protocol and patient handling of CEDM is presented. Furthermore, an overview of current results on CEDM and potential future indications are outlined.
Imaging protocol
CEDM image acquisition
In CEDM, two images are obtained per breast: a low-energy and a high-energy image. The low-energy image is acquired by using a molybdenum (Mo) and rhodium (Rh) target and Mo and Rh filters at a peak kV in the range of 26–31 kV. Since the k-edge of iodine is 33.2 KeV, the used spectrum is below this point. Consequently, the low-energy images provide maximal soft tissue contrast and are in fact comparable to a regular mammogram. Subsequently, the high-energy image is acquired by using a Mo target and double layer filter of aluminum (Al) and copper (Cu) with a peak kV ranging from 45–49 kV. Since this spectrum is above the k-edge of iodine, the obtained image contains information on iodine presence (enhancement). The high-energy image is not diagnostic and is used for postprocessing purposes. In this postprocessing step, these two images are combined to create a ‘recombined’ image that displays areas of contrast enhancement (Figure 1).

In contrast to previous suggested contrast-enhanced mammography techniques, CEDM is able to image both breasts in mediolateral oblique (MLO) and craniocaudal (CC) views with a single contrast administration. The additional high-energy image is acquired in an additional 4 s and breast compression is relieved between views. Although dependent on breast thickness, the estimated combined radiation dose from the low- and high-energy images is approximately 1.2-times the dose delivered in a standard single-view digital mammography [5].
Patient handling
In our institution, patients undergoing CEDM receive 1.5 ml iodinated contrast per kilogram of bodyweight intravenously, using an automated power injector at a rate of 3 m per second, followed by a saline flush. The optimal dose and concentration of iodine contrast agent is unknown, and the current protocol is based on experiences in pilot studies. However, it is to be expected that the imaging protocol can be optimized further, not only regarding contrast dose, but also its timing. Future comparative studies are needed to further optimize the imaging protocol. Nonetheless, the current protocol enables CEDM users to easily reproduce findings of previous studies without risk of altering the diagnostic accuracy. Two minutes after contrast administration, a CC view of the breast without a suspicious abnormality is acquired, followed by a CC and MLO view of the other breast, followed by a MLO view of the first breast. Total imaging time is approximately 7 min; the total time of examination (including contrast injection) is approximately 20 min. At the end of the exam, patients are monitored for an additional 15 min to rule out adverse contrast reactions.
Contraindications for the intravenous administration of an iodine-based contrast agent have to be considered before any CEDM exam, such as (prior) allergic reaction to iodine-based contrast agents or known renal function impairment. The current generation of iodine-based contrast agents is well tolerated and considered safe. In patients that receive a low-osmolality agent, adverse reactions can occur in 1–3% [6]. The majority of these reactions are mild and often self-limiting. In some events, intravenous medication can result in resolvement of the adverse reaction. However, more severe reactions occur in approximately 0.2–0.7% of the cases, and may consist of bronchospasms, hypotension or hypertension, laryngeal edema, tachycardia or bradycardia, seizures or pulmonary edema [7,8]. Fatalities as a result of contrast administration are considered to be rare [9].
Any administration of an iodine-based contrast agent could result in contrast-induced nephropathy (CIN), which is defined as ‘a condition in which an impairment of renal function (i.e., an increase of serum creatinine by more than 25% or 44 μmol/l) occurs within 3 days following intravascular administration of contrast medium in the absence of an alternative etiology’ [10]. To assess the risk of developing CIN, the Contrast Media Safety Committee of the European Society of Urology provided several guidelines for the safe use of contrast agents, which were recently updated [10]. With the aid of these guidelines, patients who are at risk of developing CIN can be identified using a questionnaire. Patients at risk according to this questionnaire should have their renal function checked by a blood sample prior to the examination. If necessary, precautionary prehydration and monitoring of renal function should be considered. According to the European Society of Urogenital Radiology (ESUR) guidelines [10] an eGFR <45 ml/min/1.73 m2 is considered a risk factor in developing CIN.
There is a large variation regarding the policy on preparative fasting before the administration of an iodine-based contrast agent. Although many institutions still have a protocol on fasting before these exams, Lee et al. showed that there is no evidence that fasting prior to an examination results in a significant reduction of aspiration-related complications [11]. Consequently, preparative fasting prior to CEDM is not necessary.
Current results of CEDM
In 2003, Lewin et al. published a feasibility study on CEDM [12]. In this study, 13 invasive breast cancers in 26 patients were studied using this technique. Unlike current CEDM protocols, their protocol consisted of the imaging of a single breast in a single view. Eleven breast cancers showed strong enhancement after contrast administration. One breast cancer showed moderate enhancement, and one weak enhancement. In benign cases, they observed diffuse enhancement in two cases, and weak focal enhancement in two others. Despite a very small study population, their pilot results warranted further research. A major limitation of their protocol was that the exam consisted of one breast in a single view. With this approach, the contralateral breast could not be evaluated, and ultrasound-guided localization of the abnormality might be difficult in single view exams.
The next step in the development of CEDM consisted of CEDM of a single breast in a single view, but at different time points. The aim of this approach was to investigate signal intensity time curves of various breast lesions, similar to the curves known from breast MRI [13]. Diekmann et al. studied 21 patients with 26 breast lesions (ten benign, 15 malignant, one borderline type of adenomyoepithelioma) [14]. In their study, all malignant lesions showed enhancement. One low-grade ductal carcinoma in situ failed to show enhancement. They demonstrated that half of the benign lesions did not show enhancement. However, their study failed to demonstrate any resemblance in enhancement kinetic analysis to breast MRI.
Dromain et al. studied 20 patients with a similar approach [15]. In their study, 16 out of 20 breast cancers showed enhancement. The malignant cases that did not show any enhancement were all invasive breast cancers. They observed a good correlation between tumor diameter assessed with contrast-enhanced mammography and histopathological specimens: r2 = 0.743. Unfortunately, no information on agreement was provided, and good correlation does not automatically imply good agreement [16]. In addition, a poor correlation was found between mammography results and intratumoral microvessel density. A major limitation of this study was that owing to the analysis of solely breast cancer cases, no information on specificity could be calculated.
Diekmann et al. published a second study on CEDM in 2011, in which 80 breast lesions in 70 patients were evaluated (50 benign, 30 malignant) [17]. In this study, multiple readers evaluated the images, and all readers detected more breast cancers in absolute terms using this technique. On average, 5.7 more malignant lesions were detected with CEDM, but they still used different image acquisitions at different time points to evaluate enhancement kinetics. Unfortunately, the kinetic analysis information showed a large variation and the authors concluded that kinetic analysis with this technique remained challenging.
The imaging protocol so far, which consisted of CEDM of a single breast in a single view, had some important limitations: it did not provide any information on the contralateral breast, while it is known that contralateral breast cancer can occur in 3% of the cases [18]; image acquisition is rather long, while the breast remains compressed, resulting in patient discomfort; the lack of a second projection view hampers the detection of the lesion with additional imaging, for example targeted ultrasound for biopsy guidance. Also, the studies so far failed to reproduce the enhancement kinetics analysis that is so useful in breast MRI. As a result, the image protocol changed and the different time points were substituted for CEDM exams of both breasts in two views (CC and MLO) [19].
With this new approach, Dromain et al. studied 142 breast lesions (62 benign, 80 malignant). Sensitivity for CEDM (93%) was significantly higher than conventional mammography (78%), at no loss of specificity. All multifocal breast cancers were correctly identified by CEDM [20]. Shortly thereafter Dromain et al. published a second paper with largely the same study population, studying 148 breast lesions in a multireader study [5]. The clinical performance (as expressed by the area under the receiver operating characteristic curve) increased for all readers for CEDM and ultrasound (0.87) as compared to conventional mammography and ultrasound (0.83).
Jochelson et al. compared CEDM to conventional mammography and breast MRI in 52 breast cancers [21]. Sensitivity was an equal 96% for both CEDM and breast MRI, and superior to conventional mammography: 81%. CEDM resulted in less false-positive findings as compared with breast MRI, but breast MRI was more accurate in detecting multifocal breast cancers. However, their sample size was rather limited, but the results showed that CEDM has the potential to replace breast MRI for some indications.
Most recently, Fallenberg et al. showed in 80 patients that breast cancer detection improved in CEDM as compared to conventional mammography. In addition, tumor size measurement between CEDM and breast MRI were compared, showing that there was no significant difference between lesion measurements on MRI and CEDM compared with histopathology [22]. In their study, Pearson's correlation coefficients for CEDM versus histopathology and MRI versus histopathology were 0.773 and 0.654, respectively.
In summary, several studies have confirmed that CEDM has promising potential as a breast imaging tool. Current studies show that CEDM is superior to regular mammography and might even match the diagnostic performance of breast MRI. The number of false-positive findings could even be less in CEDM compared to breast MRI, but this has not been studied extensively. A major limitation of the studies published so far is their limited number of included patients and populations having a rather high breast cancer prevalence, which does not reflect the population of routine clinical practice. If, for example, CEDM would result in many false-positive findings in populations with lower breast cancer prevalence, the technique would still be regarded as useless. Consequently, future studies are needed to evaluate the diagnostic performance of CEDM in populations with much lower disease prevalence.
Potential indications
Because the principle of tumor enhancement used in CEDM and contrast-enhanced breast MRI are similar, it is to be expected that CEDM indications could also be similar to those of breast MRI. Current accepted breast MRI indications are assessment of preoperative disease extent, response monitoring in patients receiving neoadjuvant chemotherapy, evaluation of the breast after breast-conservative therapy, inconclusive findings, screening of high-risk patients and unknown primary cancers [23]. Although image-guided interventions and implant imaging are also accepted breast MRI indications, these indications are not (yet) feasible with CEDM.
Preoperative assessment of disease extent
In breast cancer detection and disease extent evaluation, CEDM has been shown to be superior when compared to mammography, and similar or even better than breast MRI (Figure 2) [21,22]. Ductal carcinoma in situ (DCIS) is most commonly associated with the presence of microcalcifications. Although DCIS can be detected with breast MRI [13], low-grade or some intermediate-grade DCIS might not show enhancement and might be misinterpreted on breast MRI. Besides visualizing enhancing masses and lesions, CEDM has the added benefit of being able to evaluate microcalcifications using the low-dose images, which is not possible with MRI. Breast MRI is the most accurate technique to analyze disease extent [24], showing a good correlation with tumor extent assessed by pathology specimens. In a recent study, CEDM has been shown to have an excellent correlation with respect to the evaluation of disease extent [22]. Although promising, current study results are still based on limited sample sizes. Nonetheless, they showed CEDM's potential to assess disease extent as well as breast MRI. Multifocality might be a problem, since Jochelson et al. showed that breast MRI remains superior to CEDM in the evaluation of multifocal tumors [21]. However, there were only very few cases of multifocal cancers in this population, and no scientific conclusions can be drawn from this study with respect to the assessment of multifocal breast cancers. More studies are needed to evaluate the potential of disease extent evaluation with CEDM, but CEDM might already provide a suitable alternative for assessing disease extent in patients with contraindications for MRI or claustrophobia.

Response monitoring of neoadjuvant chemotherapy
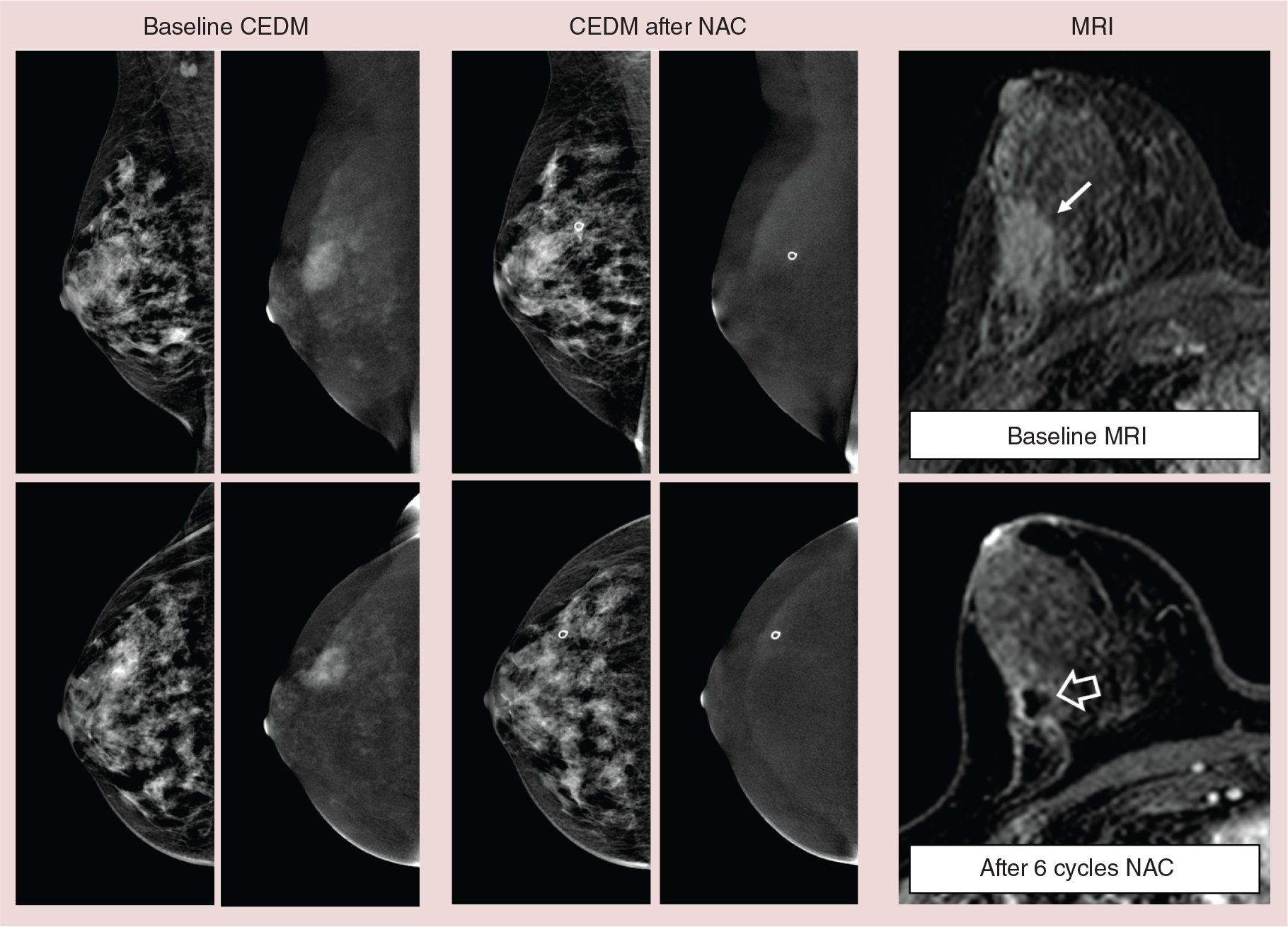
In response monitoring of patients receiving neoadjuvant chemotherapy (NAC), breast MRI has been shown to be the most accurate modality [25]. For this purpose, breast MRI sequences can be used for either early response monitoring (i.e., after several cycles of chemotherapy), or after completion of the therapy to assess the presence of residual disease [26,27]. The accuracy of breast MRI in response monitoring is dependent on breast cancer subtypes and therapy regimen and is currently a topic of extensive research. We were able to test the hypothesis that CEDM can assess response to NAC in several volunteers who underwent CEDM as part of their preoperative evaluation. In these proof-of-concept exams, we were able to demonstrate that it is feasible (Figure 3), and it is currently being studied in multiple centers.
Breast evaluation after breast-conservative therapy
In this setting, CEDM might be used for evaluation of residual disease after positive tumor margins, or as a method to detect local recurrence. Scar tissue is an important factor in every imaging modality that is used for evaluation after breast-conservative therapy. The traction of the scar tissue itself results in irregular or spiculated morphology, which makes early detection of local recurrence difficult. In our institution, we were able to detect one local recurrence with CEDM, showing an enhancing mass within the scar tissue. Even more important, it showed disease extent adequately despite the underlying distortions of the scar tissue (Figure 4). However, since these cases are rare owing to improvements in breast cancer therapy, we need to collect more of them. From breast MRI experiences, it is known that detection of residual disease after recent surgery with tumor positive margins is hampered due to aspecific enhancement caused by the healing processes. Owing to the similarity in principle of enhancement in CEDM, similar limitations can be expected. However, no case reports or studies have published findings on these kinds of patients.

Screening of high-risk patients
For screening purposes, contrast administration and its potential side effects will hamper the use of CEDM in a general population. Several patient populations with increased risk of developing breast cancer, such as BRCA1 and 2 gene mutation carriers, Cowden and Li Fraumeni syndrome and their first degree relatives, or women that underwent chest radiotherapy early in life have been shown to benefit from annual screening with breast MRI. In The Netherlands, these women receive annual breast MRI from the age of 25 years, which is combined with annual mammography (to detect microcalcifications) from the age of 30 [28,29]. These women have to visit our department twice for these exams. However, these (young) women are more sensitive to the effect of ionizing radiation of their (dense) breasts, so dose will be an issue particularly in these women. Dose measurements reported so far were equal to conventional mammography [22], or slightly higher: +20% [5]. To compensate for minor additional dose in CEDM, these women might be considered to only undergo CEDM in MLO views, with additional views performed only when indicated. However, current reports on CEDM dose were part of a subanalysis in a larger study, and no objective standardized dose measurements have been performed thus far. These are needed to clarify the additional dose that is associated with CEDM and should be weighed against the potential benefit of screening high-risk women with CEDM.
Inconclusive findings
A frequently occurring indication for breast MRI is an inconclusive finding on conventional mammography. Because of the high negative predictive value of breast MRI, underlying breast cancer can be ruled out if breast MRI is negative. For MRI the positive predictive value and negative predicted value is reported to be 72 and 85%, respectively [30]. In this study, patients with negative needle biopsies that did not yield specific benign diagnoses (e.g., fibroadenoma, papilloma) and who did not undergo subsequent excisional biopsy underwent clinical and mammographic follow-up after 1 year to ensure stability of the suspicious lesion.
In our institution CEDM is used for the evaluation of women referred from breast cancer screening. Although some cancers are obvious on conventional mammography, the majority of these referrals can be considered as ‘inconclusive findings’. Preliminary results of the first 80 women in this study also demonstrated a negative predictive value of CEDM of 100%, suggesting that (similar to breast MRI) breast cancer could be virtually ruled out if CEDM is negative. However, this study is currently ongoing to include a larger number of patients.
Unknown primary cancers
In these patients, metastases elsewhere have been found, but a primary tumor site is still unidentified. It is known from breast MRI, that it is abnormal in 50% of the cases where a conventional mammogram was negative. These numbers even increase to 75–85% if the metastases were found in the axilla. Consequently, it is recommended to perform breast MRI in cases with unknown primary cancers when the initial mammogram was negative. However, this implies an additional exam in patients who already are undergoing extensive evaluation for this problem. Although no case examples have been reported so far to confirm the use of CEDM in these cases, it might be considered since principles behind CEDM and breast MRI are comparable.
CEDM-guided interventions & implant imaging
CEDM-guided interventions are not yet available, but are a topic of technical developments. Although most enhancing lesions on CEDM can, to some extent, be visualized on the low-energy image, some enhancing structures might remain occult even when compared to the low-energy images. It is mandatory that a ‘CEDM-guided stereotactic’ biopsy becomes available when its technical issues are resolved. However, chances are very high that this structure will enhance on breast MRI too, making it accessible for MRI-guided biopsy. This latter approach is especially difficult for institutions with limited access to MRI and inability to perform breast MRI-guided biopsies themselves. Thus, a CEDM-guided biopsy technique is essential for CEDM to become a clinical success in many hospitals worldwide.
The integrity of breast implants cannot be assessed using CEDM. Breast MRI, using dedicated sequence protocols, remains essential for this evaluation. Also, CEDM is more challenging in breast implants, since exposure times will be increased owing to implant presence. As a result, the x-ray tube will generate more heat and needs to cool down longer, hampering the CEDM imaging protocol.
Conclusion
In summary, CEDM is a potentially important imaging tool in detecting and diagnosing breast cancer. Several studies have already shown its superiority when compared to conventional mammography. In addition, recent studies have shown that its diagnostic performance might match that of the most accurate breast imaging modality available to date: breast MRI. However, to further validate the strengths and weaknesses of CEDM more studies are needed in order to define proper CEDM indications.
Future perspective
Although preliminary CEDM studies have shown promising results, the study sample sizes were limited and populations consisted of a high prevalence of breast cancer. This is suitable for feasibility studies, but it does not reflect true clinical populations, in which most women do not have breast cancer. Future studies should also evaluate the diagnostic performance of CEDM in populations with low disease prevalence. If CEDM would result in a high number of false-positive findings, the technique would still be useless in everyday clinical practice.
An interesting development in the area of contrast-enhanced mammography is contrast-enhanced dual-energy tomosynthesis (CEDT). In tomosynthesis, the compressed breast is imaged in multiple planes, resulting in 3D imaging volumes through which the user can scroll, usually in 1 mm slices [31]. Several prototype machines are currently under investigation. Recently, Froeling et al. demonstrated that with this technique, signal intensity time curves might be evaluated with mammography, similar to breast MRI. In their study, they showed a significant correlation between contrast kinetics in the signal intensity time curves between contrast-enhanced dual-energy tomosynthesis and breast MRI, which might further aid in breast lesion evaluation [32].
Finally, since the principles of tumor enhancement are similar in CEDM and breast MRI, similar indications might also be expected. Preliminary studies have shown potential for CEDM as a replacement for breast MRI in preoperative evaluation of disease extent and its ability to solve inconclusive findings on conventional imaging, but the number of cases studied is still rather limited. In addition, other potential indications, such as response monitoring after NAC, evaluation of the breast after conservative therapy, screening of high-risk patients, and evaluation of patients with unknown primary malignancies are topics of ongoing studies, but the proof of principle has been shown in pilot data and case examples.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Executive summary
Contrast-enhanced dual-energy mammography (CEDM) is a promising new breast imaging modality that is superior to conventional mammography.
Preliminary studies have shown that diagnostic performance of CEDM might be equal to that of breast MRI.
Although preliminary studies are promising regarding breast cancer detection and evaluation of disease extent, CEDM has not yet been performed in populations with low disease prevalence, resulting in insufficient knowledge regarding false-positive findings in CEDM.
CEDM might be an alternative or replacement for breast MRI in several indications, including evaluation of disease extent in the postoperative breast, response monitoring in patients receiving neoadjuvant chemotherapy, inconclusive findings, and breast evaluation in patients with unknown primary cancers.