
Abstract
Despite efforts to reduce morbidity and mortality in breast cancer, Latinas continue to have lower 5-year survival rates than their non-Latina white counterparts. All along the cancer continuum from screening to follow-up of abnormal screening to diagnosis and treatment to survivorship, Latinas fare poorer than non-Latina whites. To close this gap, a number of research projects across the continuum have attempted to improve breast cancer outcomes. In this review, we examine studies that have been carried out in breast cancer along the cancer continuum. We focus not only on randomized, controlled trials, but also on quasi-experimental, and pre- and post-test studies that provided interventions for positive breast cancer outcomes. We examine not only the intervention outcomes, but also the type of intervention targets and type of intervention implementation. In future breast cancer research among Latinas, more emphasis should be placed on the steps in detection and treatment that occur after screening.
 Medical Education Online
Medical Education Online
This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Medscape, LLC and Future Medicine Ltd. Medscape, LLC is accredited by the ACCME to provide continuing medical education for physicians.
Medscape, LLC designates this Journal-based CME activity for a maximum of
All other clinicians completing this activity will be issued a certificate of participation. To participate in this journal CME activity: (1) review the learning objectives and author disclosures; (2) study the education content; (3) take the post-test with a 70% minimum passing score and complete the evaluation at www.medscape.org/journal/wh; (4) view/print certificate.
Learning objectives
Upon completion of this activity, participants should be able to:
Analyze the epidemiology and impact of breast cancer among Latinas
Distinguish disparities in the detection and management of breast cancer faced by Latinas
Evaluate interventions to improve breast cancer detection among Latinas
Compare cultural and systematic interventions to improve breast cancer outcomes among Latinas
Financial & competing interests disclosure
Elisa Manzotti, Publisher, Future Science Group
Breast cancer in Latinas in the USA presents a complicated picture. On the one hand, a lower incidence of breast cancer exists for Latinas compared with non-Latino whites (NLWs) [1], although highly acculturated Latinas are likely to have breast cancer rates that are consistent with those of NLWs [2]. On the other hand, breast cancer is the most common cancer among Latinas [101]; Latinas have lower 5-year survival rates than NLWs [1,3,102]. Furthermore, unlike NLWs who are experiencing a drop in mortality rates, Latina mortality rates are remaining stable [103]. Finally, Latinas experience lower rates of 5-year cancer-specific survival [104].
Ethnically-based disparities between the US NLWs and Latinas in breast cancer prevention and control have been documented at every stage of the cancer continuum: screening, follow-up of abnormal screening results, cancer diagnosis/treatment, survivorship and end of life. Multiple biophysiological factors contribute to differences in breast cancer between Latina and NLW women. For example, Latinas are at higher risk for the BRCA gene; furthermore, Latinas are at greater risk for estrogen- and progesterone-negative tumors, for which there are fewer treatment options, a higher chance of recurrence and lower odds of survival [4,5]. Moreover, Latinas are more likely to present with breast cancer that has metastasized at younger ages [6]. Comorbidities additionally influence breast cancer risk: Latinas are also at greater risk for obesity relative to NLW [7], which has been associated with increased breast cancer risk of various tumor types [8] and mortality [9]. Finally, disparities in behavioral, communication and psychosocial factors have been thought to contribute to an overall negative breast cancer involvement among Latinas, culminating with the observed difference in rates of breast cancer mortality between Latinas and NLWs [10,101]. The majority of interventions dedicated to improve the breast health of US-based Latinas have focused on the latter components. Consequently, this review focuses on these aspects of breast cancer. Figure 1 demonstrates the disparities in these aspects of cancer across multiple stages of the continuum that are described below.
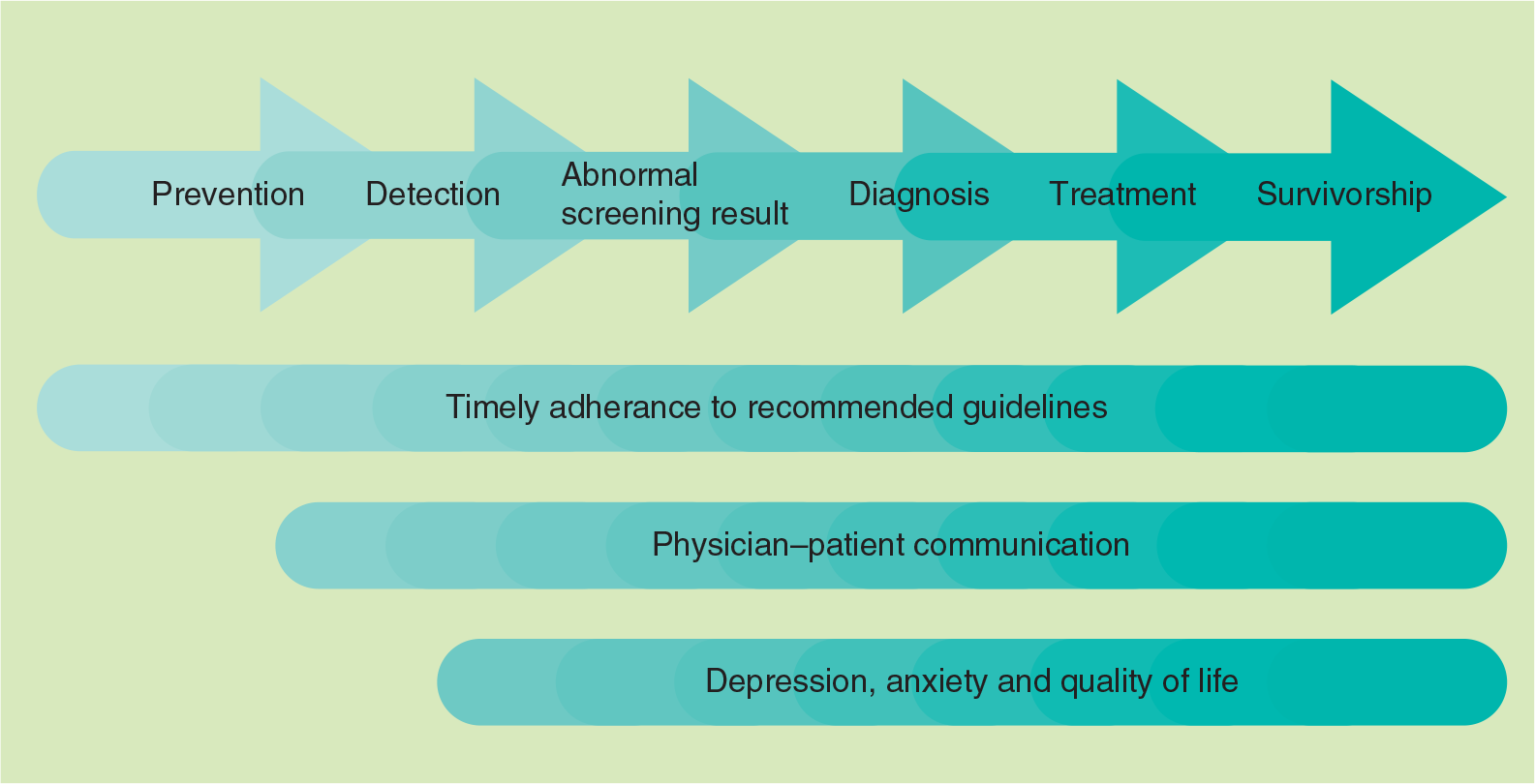
Outcomes of interest across the cancer continuum for interventions improving Latinas’ breast health.
Behavioral factors and timely adherence to recommended guidelines in particular, may serve as an important contributor to differences in breast cancer survival. In terms of prevention, diet and physical activity have been linked to breast cancer risk and differences exist between Latina and NLW women [11]. Timely adherence to recommended screening guidelines is an important disparity that has been thought to be integral to early-stage detection and survival. Specifically, there are higher rates of nonadherence to screening recommendations for clinical breast examinations (CBEs) and mammograms for Latinas relative to NLWs [12]. There are also lower rates of adherence to follow-up for abnormal screening, and greater times to diagnostic resolution [13,14], which have been linked to disparities in late-stage detection [15,105]. In addition, Latinas experience greater delays in initiation of treatment [16,17]. Disparities also exist among breast cancer survivors, in which their Latina breast cancer survivors have been documented to be less adherent to adjuvant therapy than their NLW counterparts.
Communication inequalities may also contribute to negative experiences across the breast cancer continuum and potentially breast cancer mortality. A growing body of research has documented communication inequalities across multiple stages. With regard to screening, providers appear to be less likely to recommend mammography screening to Latinas compared with NLWs [18]. Simultaneously, Latinas are less likely to comprehend recommended follow-up care, as well as being less likely to accurately report the follow-up care they have received after receipt of an abnormal mammogram result, potentially owing to linguistic barriers and health literacy levels [19–22]. During diagnosis and treatment, Latinas experience elevated levels of dissatisfaction concerning treatment decisions [23,24], and report more patient–physician communication problems, partially as a consequence of linguistic barriers and acculturation [25]. Inadequate interactions with providers may be related to subsequent reliance on family and social networks in the decision-making process for Latinas with regard to treatment [25]. Communication problems may be particularly relevant for less acculturated Latinas, who report more unmet information and care support needs than other women [26]. Such communication issues may contribute to inequalities in treatment options; for example, Latinas are more likely to experience ‘substandard’ treatment options [3,27–29]. Communication inequalities have also been documented to continue following treatment; for example, some research has indicated that Latinas have less information regarding reconstruction and express greater decisional dissatisfaction regarding breast reconstruction surgery after a mastectomy [30].
Finally, breast cancer disparities exist in relation to psychosocial experiences associated with cancer, including depression, anxiety and quality of life. Differences have been well documented with regard to later stages of the cancer continuum. For example, Latinas appear to experience particularly high levels of anxiety following receipt of an abnormal mammogram, which has been linked to diagnostic delays [19,31]. After a breast cancer diagnosis, Latinas experience poorer quality of life as patients and as breast cancer survivors [32]. In particular, studies have documented that lower acculturated Latinas express a lower quality of life and elevated levels of worry of recurrence [33,34].
In an effort to reduce cancer health disparities, intervention studies have been conducted at each stage of the cancer continuum. Many studies have been conducted with the aim of increasing timely adherence and to increase breast cancer screening in Latinas in particular. Other studies have examined discrepancies in follow-up to abnormal screening and treatment, while others attempted interventions to enhance initiation of treatment. Interventions have additionally sought to address communication inequalities and disparities in quality of life, as well as psychosocial experiences to a lesser extent. As a group, there are at least two modes of intervention, systemic or cultural, that have been used to improve breast cancer outcomes in Latinas.
Systemic barriers include the obstacles that exist in the US healthcare system, where healthcare is closely tied to insurance status. Latinas have lower rates of any kind of insurance (public or private) than NLWs [35]. Furthermore, many government-funded insurance programs pose additional problems for Latinas (e.g., being undocumented). A second systemic barrier is the thoroughness or quality of care that is available to Latinas. For example, Latinas who are monolingual Spanish speakers are less likely to navigate the complexities of the US healthcare system than English-speaking women [36,37]. As a result, they may not receive all the services to which they are entitled [38–40].
Cultural barriers may account for some of the individual reluctance to seek screening or treatment. These factors may underlie the heightened disadvantage unacculturated Latinas experience if diagnosed with breast cancer, in terms of communication difficulties and quality of life [30,33,34,41]. Indeed, a woman's health needs and decisions may depend on her self-perception relative to the needs and interests of others (e.g., children and spouses) as a matter of cultural socialization. This is particularly relevant for Latina populations, in which there is a strong emphasis on warm, interpersonal relationships (e.g., personalismo and familismo), and norms may correspond to taking care of one's family first and themselves second (e.g., marianismo [42]). Other cultural values and practices relevant to breast health prevention and treatment include views of fatalism [43–46], and the belief that a woman requires symptoms before seeing a physician [47]. All of these factors may contribute to timely adherence of recommended guidelines. For example, Latinas may be more likely to delay screening mammography since they prioritize healthcare for family members over themselves. Furthermore, cultural competence in care may also prevent Latinas from receiving adequate screening and treatment. This is likely to occur when providers view a woman as more able to understand and follow through on recommendations than is actually the case, resulting in communication barriers and misunderstanding concerning recommended guidelines [48]. Indeed, communication efforts to increase adherence may be best framed in the context of warmth between providers and patients, as well as the perceived benefits of decisions to a woman's family and social network.
A number of interventions have attempted to address the various systemic and cultural factors that provide barriers for Latinas in breast cancer screening and treatment, with fewer focusing on cancer survivorship and mortality. These interventions appear to address cultural barriers to screening through the use of lay health educators (promotores) and community-wide activities [49–51]. Promotores are often used as bridges between communities and their health systems, given their in-depth understanding of cultural values, norms and behaviors. They may be better conduits to deliver and disseminate health knowledge. Activities held in communal areas, such as churches, health fairs and community centers, have have been shown to be effective in improving health promotion outcomes, but have often been used in tandem with peer and lay health educators.
By contrast, interventions addressing the systemic aspect of Latina breast cancer care have primarily focused on enhancing access and navigation of care [52]. For instance, several studies have addressed financial and transportation barriers, whereas others have employed patient navigators to assist with the coordination of care [28,53].
Existing reviews concerning Latina breast cancer interventions, however, have focused primarily on one stage of the continuum (i.e., mammography [49]), assessed one type of study design (i.e., randomized controlled trials [RCT]) [2] or have not focused specifically on Latinas [51,52]. Furthermore, no review to date has assessed the scope of interventions in terms of the nature of the intervention target (cultural vs systemic).
The purpose of this review is to gain a perspective on the entire scope of interventions that attempted to increase positive breast health outcomes among Latinas across the cancer continuum. Unlike a systematic review that may include meta-analysis, the authors examined and classified interventions of all types, from a RCT to one sample pre- and post-tests. Our goal in gathering such an all-encompassing list of studies was to develop an understanding of the type of breast cancer research that has been conducted in Latinas across the breast cancer continuum. This approach offers the opportunity to identify gaps, strengths and weaknesses in this body of literature. In addition to this goal, in this review, we sought to characterize the interventions by their emphases: cultural, systemic or both. Our work provides a springboard from which we may gain insight into heterogeneities in methodology and thereby better understand the implications of existing interventions to addressing cancer health disparities among US Latinas with breast cancer.
Methods
The authors conducted literature searches using Google Scholar, PubMed, Medline, Science-Direct and Web of Knowledge to identify breast cancer interventions for Latina women. In order to be considered for this review, articles describing interventions had to meet the following eligibility criteria: be published between 1990 and 2012; have a sample in which at least 25% of participants were identified as Latina; and the manuscript had to be written in English. Finally, in line with Figure 1, we considered intervention studies that addressed the following outcomes of interest for Latinas across one or multiple stages of the cancer continuum: timely adherence to recommended guidelines (screening practices [46,53–70], time to follow-up [15,71–74] and initiation of treatment [72]); physician–patient communication [75]; and psychosocial measures (depression/anxiety [76–78] and quality of life [30,41,79]). Exclusion criteria included interventions concerning breast cancer knowledge, intentions/expectations to obtain a mammogram and breast self-examination, as breast cancer knowledge and mammography intentions do not necessarily result in obtaining screening and breast self-examination has not been found to be an effective early detection strategy [80].
Within each stage of the cancer continuum, studies were categorized by four foci: study design, the type of intervention, who implemented the intervention and study outcomes. Studies were considered pre-/post-test design if all participants received the intervention and were tested before and after they received the intervention, and there was no control group. Occasionally, only a post-test was reported. Quasi-experimental designs included non-random assignment of individuals or sites/census tracts into conditions. Studies were labeled as RCTs if randomization occurred at the level of the individual and/or sites/census tracts. Interventions were further described in terms of their use of lay health workers (e.g., community health workers [CHWs], promotoras and peer navigators), community wide activities (e.g., health fairs and churches) and/or healthcare professionals (e.g., general practitioners and nurse navigators) to administer the intervention. Finally, we identified the focus of intervention on cultural and/or systemic targets. If interventions did not focus on either factor, we labeled them as ‘neither’.
Results
A total of 31 studies met the eligibility criteria for this review. Of these 31 studies, 30 provided percentages/counts and have been described here. In-depth detail regarding each of these studies are provided in
List of interventions and their outcomes by phase of the cancer continuum.
Measures related to clinical breast examination practices, including proportion of women receiving clinical breast examinations, as well as clinical breast examination rate per 100 eligible years.
Measures related to mammography practices, including percentage of women obtaining a mammogram at the end of the study, change in percentage of women reporting a mammogram and mammogram rates per 100 eligible years.
Study included two interventions.
Measures related to behaviors following receipt of an abnormal mammogram, including percentage of women who adhered to follow-up guidelines and days in diagnostic interval.
Quality-of-life measures.
Measures related to percentage change in depressioN/Anxiety scores.
Measures related to improvement in and satisfaction with physician–patient communication measures.
Percentage of women who began treatment within 60 days of diagnosis.
Values represent mean ± standard deviation.
Statistically significant differences between control/intervention groups and pre-/post-test designs at p < 0.05.</i>
N/A: No data collected at baseline or for the control group, as applicable; RCT: Randomized controlled trial.
Detection
Interventions addressed increases or decreases in CBE and mammography practices, although two-thirds focused solely on screening mammography. The authors found seven RCTs, six quasi-experimental and six pre-/post-test designs in the screening area.
The majority of screening interventions implemented cultural factors, as well as cultural values to promote screening CBE and mammography rates among Latinas. The primary mode of delivery was by CHWs or promotores who were members of the targeted communities. Specifically, CHW interventions included four RCTs, two quasi-experimental studies and five pre-/post-test study designs. Cultural norms and factors also were used in terms of community contexts. For example, messages about screening were introduced within local health activities, church-based programs and in local media outreach programs (e.g., print and TV). Notably, studies employing professionals or medical technologies (e.g., kiosks in healthcare settings) as modes of delivery were, in general, noted as bicultural and were linguistically matched to meet the needs of their local populations of women. Health professionals participating in screening interventions included nurses, general practitioners and health educators.
Fewer interventions addressed systemic barriers – that is, studies that attempted to decrease structural barriers, such as access to care. Two studies attempted to influence financial barriers (i.e., by providing vouchers), peer support in navigation of the US healthcare system (using patient navigators) and cultural competency training for healthcare providers. Other projects did not address access to care, but focused on logistical barriers to participation in interventions, for example, a few CHWs facilitated access to resources, such as transportation and child care needs.
Ten of the 19 screening interventions reported significant differences related to participation in interventions (e.g., postintervention or in the intervention compared with the control group). Of those that reported significant differences, approximately 44.4% (four out of nine) were RCTs, 22% (two out of nine) were quasi-experimental and 33% (three out of nine) were pre-/post-test study designs. Among the different modes of delivery, 50% of those that employed CHWs, 25% of those that employed community activities and 33% of those that used health professionals reported significant outcomes for increased screening behavior. Although two out of three systemic interventions had significant differences in reporting increased CBE and mammography rates, similar patterns were less discernible among interventions focusing primarily on cultural barriers. Only eight out of the 17 in that category reported significant intervention effects. It should be noted, however, that four interventions did not provide sufficient data to indicate intervention effects (e.g., no control group and no preintervention data).
Abnormal screening result
Of the five interventions dedicated to improving time to diagnostic resolution after a woman received notice of an abnormal screening result, three research efforts were quasi-experimental and two utilized RCT designs. These studies primarily incorporated professional patient navigation designs and measured the percentage of women who adhered to the follow-up recommendations, as well as days to diagnostic resolution.
In this type of intervention target, culture was addressed in terms of bilingualism – that is, the patient navigators spoke both Spanish and English. In addition, referrals for care were made to community services such a local clinics or hospitals. Despite this community referral, only one of these intervention activities appeared to be in partnership with a local community organization or venue; thus, it was not clear whether the patient navigation continued after the woman sought out a biopsy. The primary focus of abnormal screening results interventions addressed the systemic factors that prevented follow-up, such as repeated attempts to contact women with an abnormal screening test and referrals to programs that would pay for a repeat mammogram or a biopsy. A few also incorporated responses to specific barriers such as scheduling appointments.
The quasi-experimental and RCT studies in this category reported significant improvements in participants compared with pre-assessment or control groups. In two studies that looked at time to resolution of an abnormal test, both significantly reduced the time to follow-up, by 18 days [74] and by 12.1 days (increasing mammographic adherence), respectviely [15]. A third study saw time to resolution actually increase [72].
Diagnosis/treatment
The six interventions related to cancer diagnosis/treatment were varied in their outcomes of interest and addressed diverse needs of cancer patients, specifically, days to treatment initiation (n = 1), physician–patient communication (n = 1), depression (n = 3) and quality of life (n = 2). Approximately half of the projects relied on the use of professionals (n = 3) compared with the use of CHWs alone (n = 2) or in combination with a CHW (n = 1). Four out of the five interventions implemented interactions with professionals, including mental health specialists and professional patient navigators; the other intervention attempted to improve quality of life through physical activity/yoga.
Approximately 50% (n = 3) of the interventions addressed both systemic and cultural factors. Systemic factors (n = 1) were addressed through patient navigation to initiate treatment. Cultural factors were addressed through use of bilingual and bicultural CHWs (n = 3). In addition, individual factors influencing quality of life and depression were addressed through yoga instruction (n = 1) and use of mental health specialists (n = 2).
Four interventions indicated significant differences in time to treatment initiation and quality of life as a result of participation in the intervention; notably, one of the other two interventions did not provide information to indicate changes or effects of participation.
Survivorship
Only one intervention met the eligibility criteria for this review. The one published study used a 10-week physical activity intervention tailored to the physical abilities of each participant to reduce distress and improve quality of life. The physical activity prescriptions were developed for each participant by healthcare professionals and participants were responsible for following the prescription.
Cultural factors were addressed with the use of bilingual survey assessment of distress, quality of life and physical instruction materials. Significantly improved levels of distress were observed and, although not significant, a trend toward improved quality of life was observed. Physical activity was not significantly improved.
Discussion
In this review of breast cancer interventions conducted with Latinas, the authors identified 19 interventions that focused on screening, five that focused on addressing abnormal follow-ups, six that examined time to treatment or treatment outcomes and one that was concerned with survivorship. Of these, however, only 13 were RCTs. Of the remainder, ten were quasi-experimental and eight were pre-/post-test or post-test only. In many cases, attempts were made to make the interventions culturally relevant; such attempts ranged from ensuring the use of bilingual materials to the use of CHWs as promotores or patient navigators.
Overall, trials that had a systemic intervention target appeared to do better than those that focused primarily on cultural adaptation. The systemic factors assessed often emphasized increased access to care; therefore, it is not surprising that they are strong motivators of behavior change [78,82]. These included reducing the costs for Latinas to be screened by providing vouchers to defray expenses, as well as patient navigation that provided information and activities to support resolution of an abnormal screening test and initiate treatment.
Some interventions that included only cultural factors were also successful. The extent to which an intervention was culturally appropriate was not always clear and it may be that minimal efforts (e.g., bilingual materials only) might not be as effective as more in-depth cultural appropriateness. Future studies may wish to test these different circumstances. On the other hand, it has become part of the prevailing conceptual models to recognize the importance of making an intervention as culturally pertinent as possible to better engage the targeted population [83].
Importantly, there were some interventions that did not address cultural or systemic factors, but focused on individual-level factors involved in wellbeing along the cancer continuum. It is worthwhile to consider that these three interventions occurred during diagnosis and treatment and pertained to depression/anxiety and quality of life for cancer patients. Altogether, the existence of interventions for predominantly Latina samples that do not focus on cultural or systemic factors speak to the particularly challenging experiences faced by cancer patients in general.
The type of intervention implementation showed a trend over time, going from an emphasis on professional delivery of intervention to CHW delivery of intervention, especially with regard to early detection. In recent years, the use of lay health workers, or promotores in Latino culture, has become a well-established method of delivery of interventions [84]. Given the strong emphasis and value Latino culture places on interpersonal relationships, it is not surprising that many CHW-driven interventions also incorporated support for and participation from families and friends. Throughout later stages of treatment, interventions still relied heavily on the focus of professionals, which may be more helpful with regard to systemic barriers (e.g., patient navigators). Future interventions concerning these stages in the continuum may seek to incorporate a cultural perspective into designs regarding quality of life and mental health status, especially given the underutilization of existing interventions and programs for cancer patients and survivors by Latinas [85]. This literature has indicated the potential benefits of incorporating family support into support programs [85]. Simultaneously, for cancer patients, literature has indicated the importance of family in treatment decisions [42]; given this, future interventions to improve outcomes at the diagnosis/treatment stage may seek to include these cultural values and norms into interventions.
Interestingly, interventions with healthcare providers also paid attention to language barriers; only one of the healthcare provider interventions did not mention the importance of bilingual resources or the bicultural nature of healthcare providers or navigators. What was missing, however, was the extent to which information was written or presented in an understandable manner. This is especially important for Latinas who have fewer years of schooling or have difficulty with health literacy [86]. These issues were rarely addressed.
As is the case with all reviews of Latina activities, there is considerable heterogeneity in Latina populations. It is known that screening varies considerably by type of Latina; for example, Mexican Latinas have the lowest rates of screening mammography and CBEs compared with other groups of Latinas [12].
It is not surprising that the majority of the breast cancer intervention research identified in this review has been on attempts to increase early detection (screening). Screening is typically the first step in early detection as it identifies cancers at the earliest stage. However, given that Latinas are more likely to have advanced stage at diagnosis and lower 5-year survival rates, it is also necessary to focus on the intervening steps. It is clear that delay of following-up or ignoring an abnormal screening test is probably linked to stage of diagnosis. Furthermore, delay in seeking treatment for an abnormal finding will have implications for treatment and stage at diagnosis. Finally, survivorship data indicate that Latinas are less likely to survive for 5 years compared with their NLW counterparts, suggesting that efforts to address post-treatment sequelae are important [1,3,101].
In reviewing the outcomes, it should be noted that the studies presented varied by degree of scientific rigor, with RCTs having the highest degree of rigor, followed generally by quasi-experimental designs, and then followed further by the pre-/post-test designs (and the post-test only designs). A further caveat is that the units of randomization varied so that some research focused on individual women, while others focused on larger units of randomization, such as churches [57,65] and even communities [46,66]. For the purposes of this review, we desired a complete accounting of Latinas and breast cancer interventions; thus, the authors included all designs. Nevertheless, caution should be used in interpreting the results.
This review adds to the existing literature on Latinas and breast cancer. It is an area that will benefit from ongoing updates as Latina rates of breast cancer are not decreasing, and are increasing in some age groups (i.e., the 40–49-year-old group) [83]. Furthermore, as the proportion of Hispanics in the USA continue to increase, we may expect to see higher rates of breast cancer in this group owing to environmental exposures, ranging from chemicals to psychosocial exposures [87,106].
Executive summary
Although Latinas have a lower incidence of breast cancer than non-Latina whites, breast cancer is the major cancer killer of Latinas.
Despite the lower incidence of breast cancer, Latinas are more likely to die of the disease than their non-Latina white counterparts; reasons for this range from biological differences to screening and treatment differences.
Intervention studies to ameliorate the consequences of the disease are found along the cancer continuum – that is, Latinas are less likely to be screened, less likely to follow-up abnormal screening tests, less likely to be treated, and have poorer survivorship than non-Latina whites.
The purpose of this review is to gain a perspective on the entire scope of interventions along the breast cancer care continuum.
The authors examined diverse interventions on breast cancer among Latinas.
The authors were comprehensive in the approach and included randomized controlled trials, quasi-experimental and pre-/post-test interventions.
A total of 31 studies met the criteria for inclusion.
The screening subgroup of interventions focused on cultural interventions and approximately half had significant results in increasing breast cancer screening by Latinas.
For abnormal screening, patient navigation was a primary focus that contributed to reduced time to follow-up.
In the diagnosis/treatment category, the interventions focused on healthcare professionals.
Only one study emphasized survivorship.
Systematic interventions that reduced costs and other barriers to screening did better at increasing breast cancer screening than cultural interventions.
Over time, there was an increased focus on the use of promotores or community health workers in terms of responding to all parts of the breast cancer care continuum.
Many studies noted that language barriers are important to address when changing behavior of Latinas.
It is important to continue to make progress in Latinas and breast cancer incidence, mortality and survivorship.
There is increasing attention on Latina survivorship and it is likely that a focus on survivorship will develop.
It is especially important to examine interventions at all phases of the cancer continuum as Latinas ‘fall out’ at all stages of the continuum.
As the Affordable Care Act becomes implemented, more work will be devoted to systemic breast cancer interventions.
Conclusion & future perspective
In conclusion, this review demonstrates that in both rigorous randomized trials and quasi-experimental approaches, much has been achieved in increasing breast cancer screening, time to follow-up and time to treatment among Latinas. Furthermore, there is some evidence that survivorship intervention can improve Latina quality of life and mental status after treatment for the disease. Addressing all stages of the cancer continuum holds hope for Latinas who are diagnosed with breast cancer. Systemic interventions appear to be effective, whereas greater work remains to be completed for interventions targeting cultural factors. Future intervention projects that are warranted include comparison of different approaches to culturally pertinent interventions; implementation and evaluation of interventions dedicated to cultural factors in later stages of the continuum (e.g., diagnosis, treatment and survivorship), and specifically in relation to communication and psychosocial outcomes; and a greater number of RCTs to gain robust support for the benefit culturally pertinent interventions.
Footnotes
Breast cancer interventions serving US-based Latinas: current approaches and directions
To obtain credit, you should first read the journal article. After reading the article, you should be able to answer the following, related, multiple-choice questions. To complete the questions (with a minimum 70% passing score) and earn continuing medical education (CME) credit, please go to www.medscape.org/journal/wh. Credit cannot be obtained for tests completed on paper, although you may use the worksheet below to keep a record of your answers. You must be a registered user on Medscape.org. If you are not registered on Medscape.org, please click on the New Users: Free Registration link on the left hand side of the website to register. Only one answer is correct for each question. Once you successfully answer all post-test questions you will be able to view and/or print your certificate. For questions regarding the content of this activity, contact the accredited provider,