
Abstract
Objective
Among vulnerable women, unequal access to advanced breast imaging modalities beyond screening mammography may lead to delays in cancer diagnosis and unfavourable outcomes. We aimed to compare on-site availability of advanced breast imaging services (ultrasound, magnetic resonance imaging [MRI], and image-guided biopsy) between imaging facilities serving vulnerable patient populations and those serving non-vulnerable populations.
Setting
73 imaging facilities across five Breast Cancer Surveillance Consortium regional registries in the United States during 2011 and 2012.
Methods
We examined facility and patient characteristics across a large, national sample of imaging facilities and patients served. We characterized facilities as serving vulnerable populations based on the proportion of mammograms performed on women with lower educational attainment, lower median income, racial/ethnic minority status, and rural residence.
We performed multivariable logistic regression to determine relative risks of on-site availability of advanced imaging at facilities serving vulnerable women versus facilities serving non-vulnerable women.
Results
Facilities serving vulnerable populations were as likely (Relative risk [RR] for MRI = 0.71, 95% Confidence Interval [CI] 0.42, 1.19; RR for MRI-guided biopsy = 1.07 [0.61, 1.90]; RR for stereotactic biopsy = 1.18 [0.75, 1.85]) or more likely (RR for ultrasound = 1.38 [95% CI 1.09, 1.74]; RR for ultrasound-guided biopsy = 1.67 [1.30, 2.14]) to offer advanced breast imaging services as those serving non-vulnerable populations.
Conclusions
Advanced breast imaging services are physically available on-site for vulnerable women in the United States, but it is unknown whether factors such as insurance coverage or out-of-pocket costs might limit their use.
Introduction
Whether patients have access to and utilize specific medical technologies is often influenced by local availability of resources.1–3 On-site availability of healthcare resources, which probably plays a role in downstream utilization, remains relatively unexplored for cancer care. 4 For breast cancer screening and diagnosis, it is uncertain whether differences in the ready availability of imaging resources beyond mammography contribute to persistent disparities in breast cancer outcomes. 5 Prior studies addressing timeliness of follow-up after abnormal mammography have been limited by a lack of data on the physical availability of advanced breast imaging modalities.6,7
Diagnostic work-up after abnormal screening mammography often requires the use of breast ultrasound, imaging-guided core breast biopsy (eg. ultrasound-guided breast biopsy, stereotactic breast biopsy), and potentially breast magnetic resonance imaging (MRI) (eg. extent of disease work-up prior to surgery). 8 Women at higher risk of developing breast cancer also seek supplemental screening modalities, including screening breast ultrasound and screening breast MRI. 9 The demand for advanced breast imaging is likely to increase with new legislation requiring imaging facilities to directly inform women with mammographically dense breasts that they are at increased risk of developing cancer and should discuss potential supplemental screening with their physicians. 10
Recent analyses have shown both disadvantages in geographic access to and utilization of advanced breast imaging technologies among vulnerable women.11,12 These women – including those from racial/ethnic minority backgrounds, with lower educational attainment, lower income, and those living in rural settings – continue to bear a disproportionate burden of breast cancer mortality.13–17 The mortality rate among African-American women compared with Caucasian women in 2006 was 49 v 35 per 100,000, even though African-American women have lower breast cancer incidence than Caucasian women. Since 1990, breast cancer mortality rates have decreased on average 2.4% per year for Caucasian women, but only 1.1% per year for African-American women. 18 Vulnerable women also experience lower rates of screening, longer wait times for diagnostic evaluation after abnormal screening, and more advanced cancer stage at diagnosis compared with non-vulnerable women. 19
To determine whether these persistent disparities are associated with the physical availability of advanced breast imaging, we compared on-site availability of advanced imaging, including ultrasound, MRI, and imaging-guided biopsy procedures, between screening mammography facilities serving vulnerable populations and those serving non-vulnerable populations. We examined data from a large, national sample of screening mammography facilities in the Breast Cancer Surveillance Consortium (BCSC) and hypothesized that facilities serving more vulnerable women were less likely to have on-site availability of advanced breast imaging and imaging-guided biopsy services, potentially contributing to disparities in patient outcomes among vulnerable populations.
Methods
Study Participants
The National Cancer Institute-funded BCSC consists of pooled breast imaging registry data shown to be representative of United States women undergoing routine screening mammography in relation to age, ethnicity, and urban or rural residence. 20 We analyzed data from five regional registries pooled at the BCSC Statistical Coordinating Center (SCC) for 2011 and 2012 (North Carolina, San Francisco, Vermont, Chicago, and Western Washington). The SCC and each registry received institutional review board approval for either active or passive consenting processes or a waiver of consent to enroll individual facilities, link data, and perform analytic studies. All procedures were Health Insurance Portability and Accountability Act (HIPAA) compliant, and the SCC and each registry received federal certificates of confidentiality and other protections for the identities of individual community facilities.
Facility Characteristics
Each of the five registries obtained data from their respective imaging facilities that offer screening mammography. Advanced breast imaging data for each facility included the availability of ultrasound, MRI, stereotactic core breast biopsy, ultrasound-guided core breast biopsy, and MRI-guided core breast biopsy. Facilities also reported data regarding any academic affiliation, for-profit versus not-for-profit status, facility location (hospital, stand-alone office, or other), and practice type (non-radiology practice, breast imaging only practice, full diagnostic radiology practice, or multi-specialty breast centre). We defined non-radiology practices as those located within and operated by a different specialty (eg. obstetrics and gynaecology clinic). Breast imaging only practices were those offering only imaging services specific to the breasts and no other body part, and full diagnostic radiology practices were those offering imaging services for multiple body parts. We considered multi-specialty breast centres to be part of an integrated care centre with on-site specialists in addition to radiologists (eg. a cancer centre with on-site breast oncologists).
Vulnerability Indices
Vulnerable or non-vulnerable populations were defined as in our previous studies,21–24 based on race/ethnicity, educational attainment, household income, and rural or urban residence. We recorded these characteristics at each mammography exam conducted at each BCSC facility in 2011 and 2012. For race/ethnicity, we used self-reported information provided at the mammography. For income, education level, and rural place of residence, we used geocoded linkages between residential zip codes and 2010 Census block-level data to assign each woman a median household income, education level, and a rural/urban score.
To characterize vulnerability of the patient population served by each facility, we calculated the following continuous facility-level vulnerability indices based on aggregated individual woman-level vulnerability measures across all mammography examinations performed at each facility in 2011–2012: 1) percentage of population composed of minorities (African-American or Hispanic/Pacific-Islander/Hawaiian/Native American race/ethnicity), 2) percentage of population with ≤high school-level education, 3) average median household income, and 4) average percentage of rural residence. We then dichotomized continuous vulnerability indices to provide binary facility-level vulnerability classifications for patient populations served by each facility. The following cut-off values were determined by taking one standard deviation above or below the means of the continuous measures: 1) racial/ethnic minority percentage >34.5%, 2) >15.8% of exams among women with less than high school education, 3) average median income <$USD 52,517, and 4) average percentage of rural residences >68.1%. In our multivariable analysis, we considered a facility to serve a vulnerable population if the threshold for any one of these four composite indices was met. We considered facilities not meeting any of the four thresholds as serving non-vulnerable patient populations.
Analysis
We performed all statistical analyses using SAS version 9.3 (SAS Institute, Cary, NC). We first computed descriptive statistics for facility-level characteristics, on-site availability of advanced breast imaging services, availability of advanced imaging services based on facility-level characteristics, and availability of advanced imaging services based on vulnerability indices. We then used unadjusted log binomial generalized estimating equations (GEE) models to calculate the relative risk of facilities serving vulnerable populations having on-site availability of different advanced breast imaging services, allowing for correlation among facilities belonging to the same group practice. Specifically, we examined the relative risk of facilities having on-site breast ultrasound, breast MRI, ultrasound-guided breast biopsy, stereotactic breast biopsy, and MRI-guided breast biopsy services based on vulnerability of patient population served (for each vulnerability characteristic and overall). We also estimated adjusted log binomial GEE models for each facility vulnerability characteristic, adjusting for whether or not the facility was located in an urban core based on Rural Urban Commuting Area Codes derived from United States Census commuting data (except for the patient rural residence index due to high collinearity between facility rurality and rurality of patients served). These additional adjusted models examined whether the relative risks of imaging availability by vulnerability index changed after accounting for the physical setting of imaging facilities.
Each model regressed a binary indicator of advanced imaging service provision on dummy variables for the patient population vulnerability characteristic of interest. Our GEE models accounted for correlation among individual facilities belonging to the same imaging group practice (one of 34 group practices) through the use of the robust Huber-White (sandwich) variance estimator. We estimated 95% confidence bounds around each probability estimate via the delta method.
Results
Facility Characteristics and Availability of Advanced Imaging
Facility Characteristics.
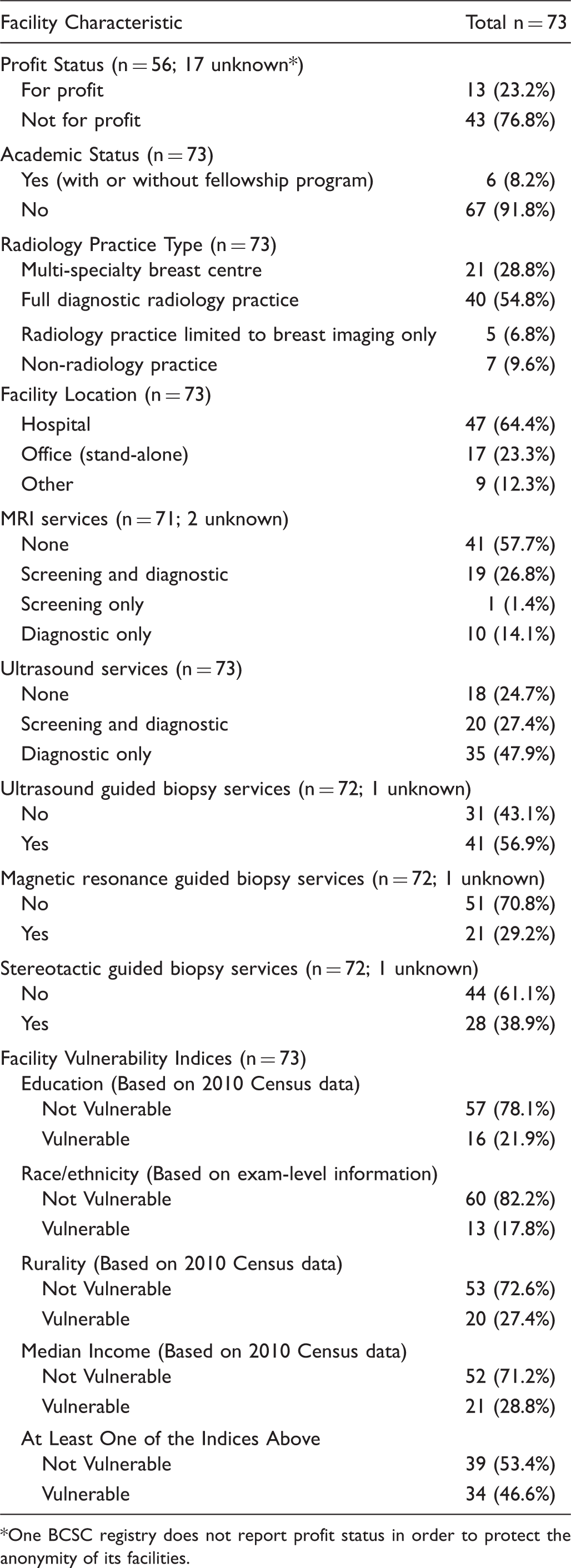
One BCSC registry does not report profit status in order to protect the anonymity of its facilities.
Advanced Breast Imaging and Image-Guided Biopsy Availability by Facility Characteristic.
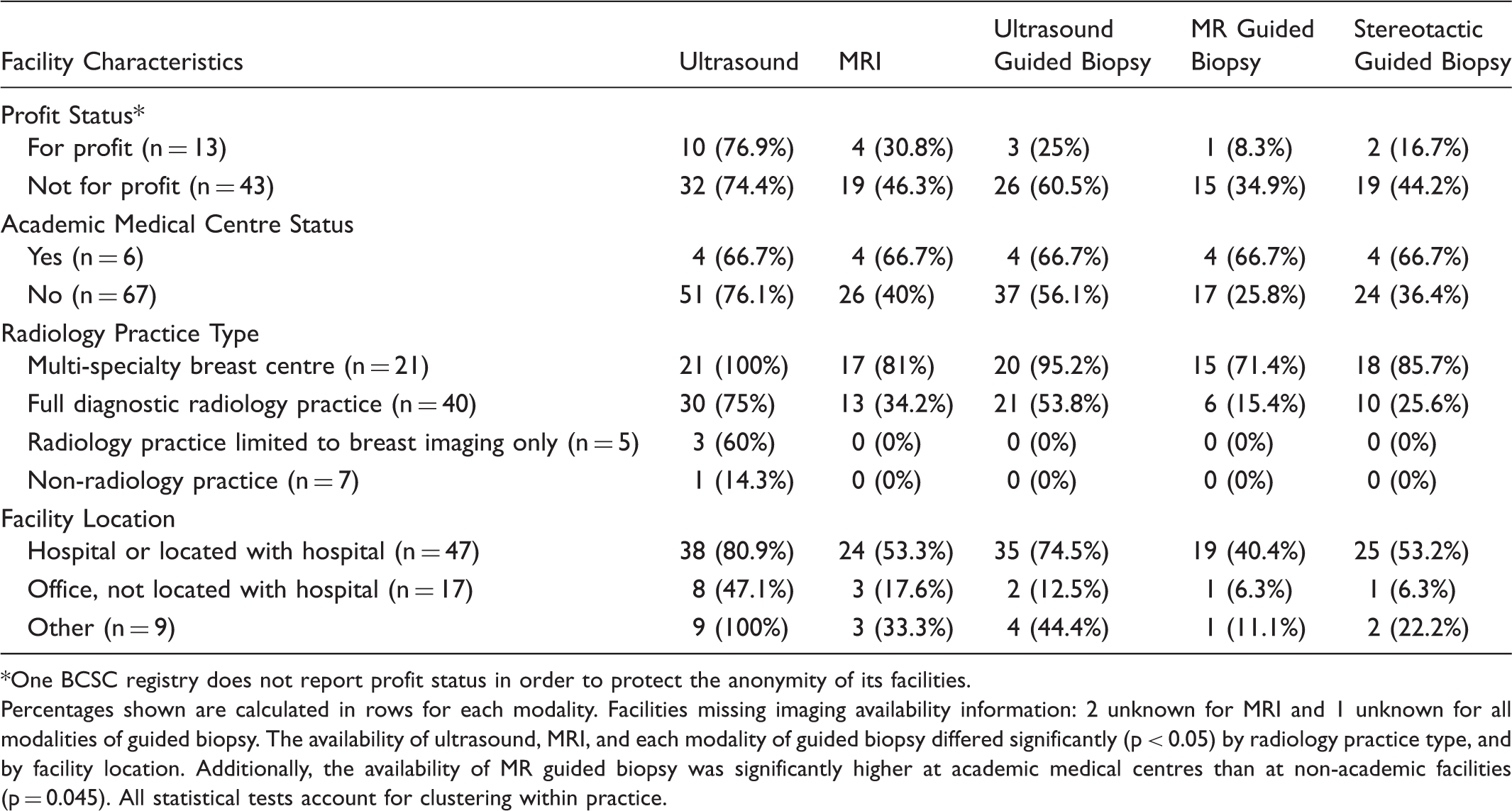
One BCSC registry does not report profit status in order to protect the anonymity of its facilities.
Percentages shown are calculated in rows for each modality. Facilities missing imaging availability information: 2 unknown for MRI and 1 unknown for all modalities of guided biopsy. The availability of ultrasound, MRI, and each modality of guided biopsy differed significantly (p < 0.05) by radiology practice type, and by facility location. Additionally, the availability of MR guided biopsy was significantly higher at academic medical centres than at non-academic facilities (p = 0.045). All statistical tests account for clustering within practice.
Facilities Serving Vulnerable Populations and Availability of Advanced Imaging
Advanced Breast Imaging and Image-Guided Biopsy Availability by Vulnerable Indices.
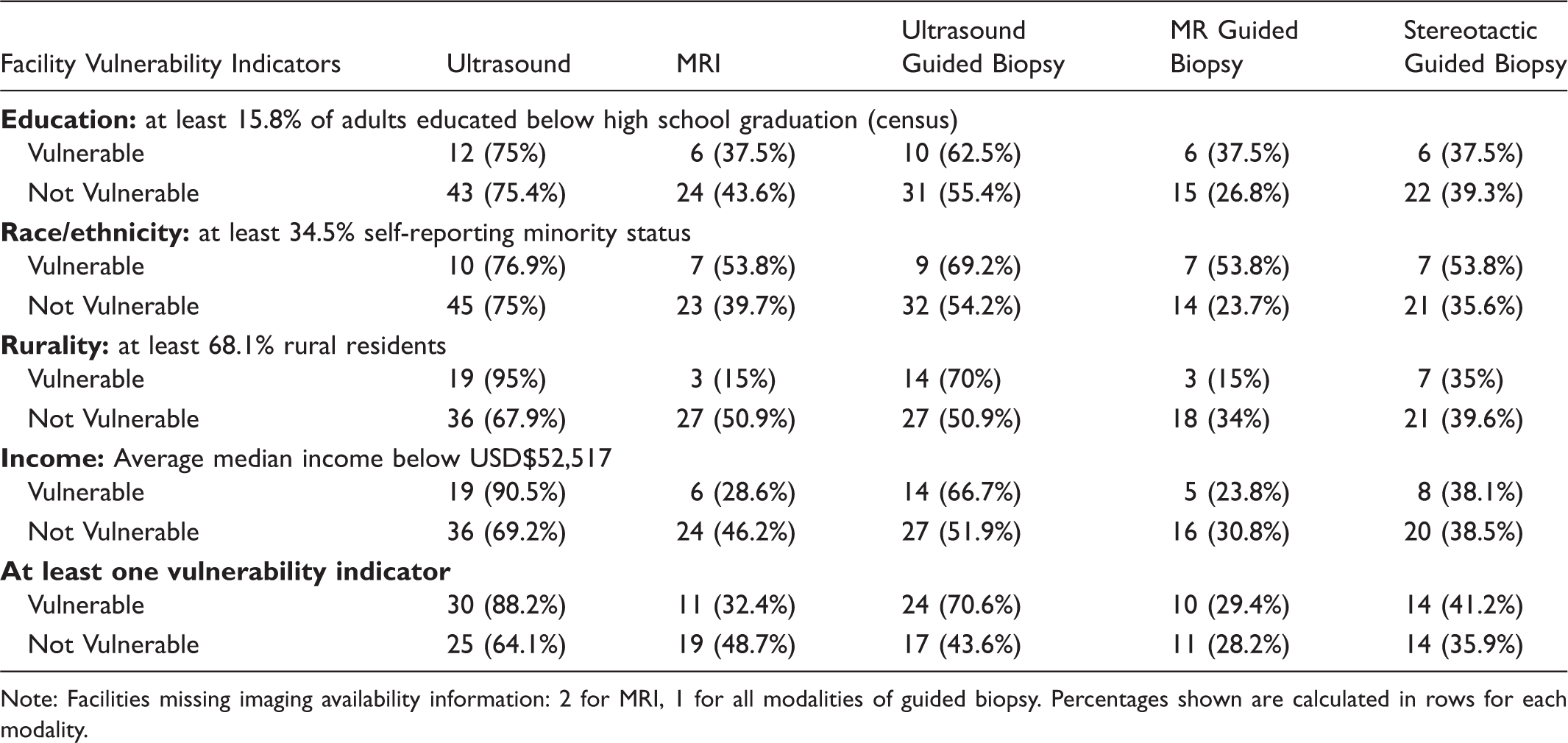
Note: Facilities missing imaging availability information: 2 for MRI, 1 for all modalities of guided biopsy. Percentages shown are calculated in rows for each modality.
Unadjusted Multivariable Models for Imaging Availability Associated with Facility Vulnerability Indices.
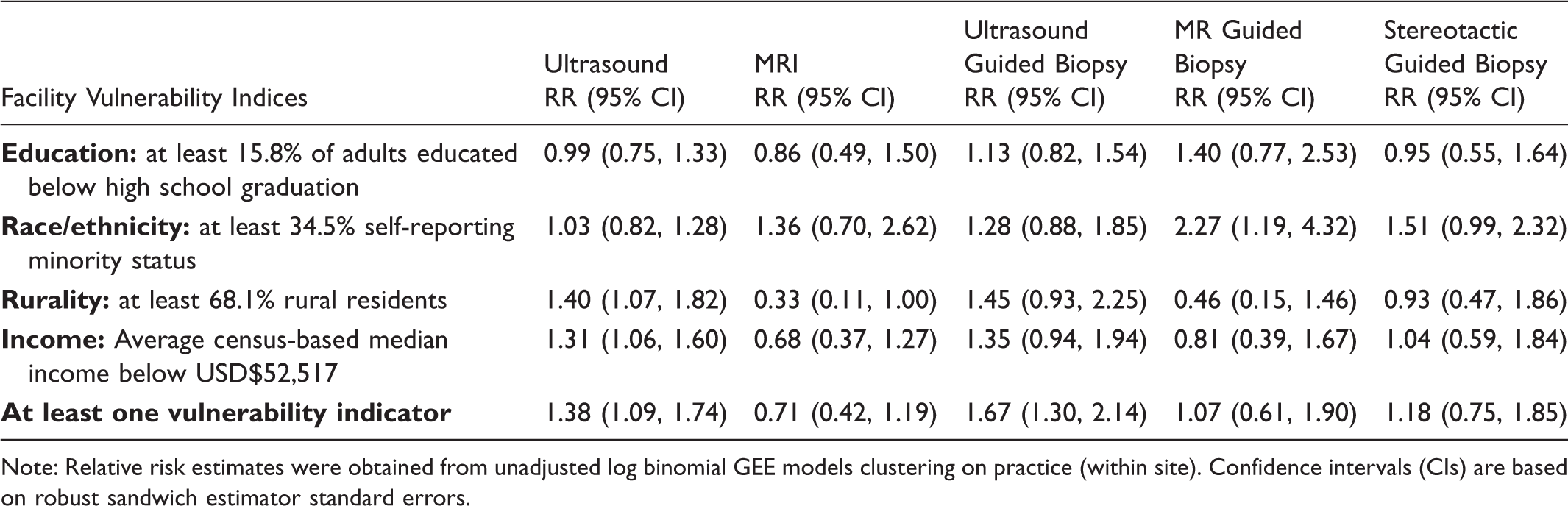
Note: Relative risk estimates were obtained from unadjusted log binomial GEE models clustering on practice (within site). Confidence intervals (CIs) are based on robust sandwich estimator standard errors.
Unadjusted regression analyses identified no significant differences in on-site availability of breast MRI (RR = 0.71 [95% CI 0.42, 1.19]), MRI-guided biopsy (RR = 1.07 [0.61, 1.90]), and stereotactic biopsy (RR = 1.18 [0.75, 1.85]) at facilities serving vulnerable populations versus facilities serving non-vulnerable populations. However, facilities serving vulnerable populations were statistically more likely to provide on-site breast ultrasound (RR = 1.38 [95% CI 1.09, 1.74]) and ultrasound-guided biopsy (RR = 1.67 [1.30, 2.14]) services than facilities serving non-vulnerable populations. We also found a borderline statistically significant relationship between rural population served and lower on-site availability of breast MRI (RR = 0.33 [0.11, 1.00]).
Multivariate Models for Imaging Availability Associated with Facility Vulnerability Indices Adjusted for Location in Urban Core.
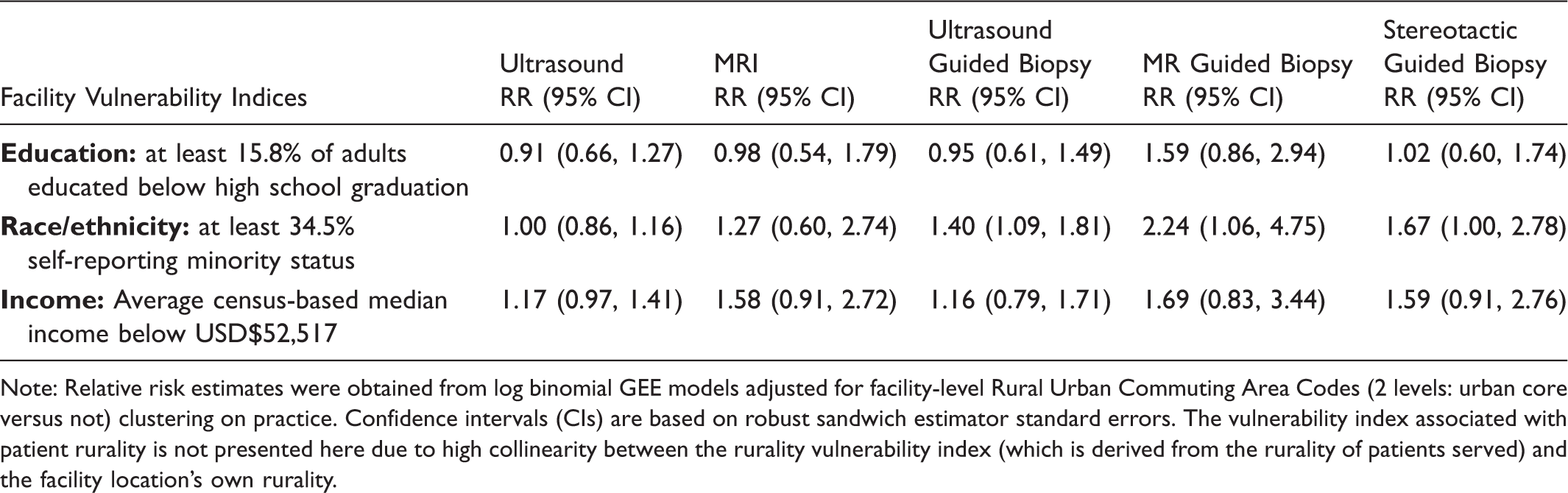
Note: Relative risk estimates were obtained from log binomial GEE models adjusted for facility-level Rural Urban Commuting Area Codes (2 levels: urban core versus not) clustering on practice. Confidence intervals (CIs) are based on robust sandwich estimator standard errors. The vulnerability index associated with patient rurality is not presented here due to high collinearity between the rurality vulnerability index (which is derived from the rurality of patients served) and the facility location’s own rurality.
Discussion
Contrary to our original hypothesis, we found that imaging facilities serving more vulnerable women were as or more likely to have on-site availability of advanced breast imaging modalities and imaging-guided biopsy services. We controlled for differences in facility profit status, academic affiliation, practice type, and practice setting. Our findings suggest that physical on-site availability does not contribute to observed health disparities among vulnerable populations in relation to accessing advanced breast imaging services, addressing a critical knowledge gap regarding the relationship between health care resource availability and disparities in breast cancer care.
Facilities serving vulnerable populations were more likely to offer breast ultrasound and ultrasound-guided breast biopsy services on-site than facilities serving non-vulnerable populations. The reasons for these seemingly paradoxical findings are unclear, but may include rural versus urban practice settings and the lack of availability of additional diagnostic imaging centres in close proximity to rural screening facilities. As breast ultrasound and ultrasound-guided breast biopsies represent the two most common advanced imaging services utilized in the diagnostic setting after abnormal mammography, it is not unreasonable for facilities to offer these additional services if they represent the only breast imaging facility accessible to a large patient population.
Of the four vulnerability indices, education level of the population served was not associated with more or less on-site availability of advanced breast imaging services. Race/ethnicity, income, and rural versus non-rural residence of the patient populations served all contributed to differences in advanced imaging availability at the facility-level. The significant relationship between rural population served and lower on-site availability of breast MRI corroborates our earlier finding regarding geographic access to breast imaging in the United States, that found longer travel times for rural residents to obtain breast MRI. 11
Our findings should not be misinterpreted to suggest that there are no disparities in access and utilization of breast imaging technologies beyond screening mammography among vulnerable women. Our analysis is limited in scope to the physical on-site availability of additional imaging modalities at the facility level among a large, national sample of facilities, and accounts for the possibility of facilities being part of the same group practice. While our results suggest that physical on-site availability does not contribute to potential disparities in access to advanced breast imaging technologies between vulnerable and non-vulnerable women, other enabling factors, such as patient insurance status and additional out-of-pocket expenses, are not addressed due to lack of data and were considered outside the scope of this analysis. Our study is limited to addressing facility-level availability of breast ultrasound, breast MRI, and image-guided biopsy services among differing patient populations. It does not address newer technologies such as digital breast tomosynthesis, approved by the FDA in 2011 and being adopted in community settings at a rapid pace, 25 but available in only 6% (4/71) of BCSC facilities at the time of our study.
Our study suggests that on-site availability of advanced breast imaging and image-guided biopsy services do not significantly differ between facilities serving vulnerable women and those serving non-vulnerable women. Future research should address potential disparities in actual on-site utilization of advanced breast imaging modalities and image-guided biopsy services among vulnerable women, including examination of additional patient characteristics, such as insurance status and health literacy. Our prior research suggests that vulnerable women experience longer wait times for follow-up of abnormal mammogram at facilities serving vulnerable populations. 22 Thus, while we found that advanced imaging services may be physically available on-site at imaging facilities, these technologies may be under-utilized by vulnerable women, due to other enabling factors.
Footnotes
Funding
This work was supported by grants from the National Cancer Institute (RC2CA148577 and, for the Breast Cancer Surveillance Consortium (BCSC), P01CA154292 and HHSN261201100031C), as well by a grant from the American Cancer Society (MRSG-14-160-01-CPHPS).