
Abstract
Most combined oral contraceptive pills contain ethinyl estradiol (EE) with progestins. In order to minimize the pill's cardiovascular risks, the concept of using 17β-estradiol (E2), the endogenous estradiol, arose in the 1970s. Many attempts to develop a pill containing 17β-E2 have failed as cycle control was low. The first pill containing 17β-E2 was launched in 2011. This monophasic pill contains 24 pills with 1.5 mg 17β-E2 and 2.5 mg nomegestrol acetate, and four placebo pills. Studies conducted in Europe and the USA demonstrate that its Pearl index is 0.38 and 1.13, respectively. It has less influence on hemostasis, fibrinolysis markers, lipids and carbohydrate metabolism than the combined oral contraceptive levonorgestrel/EE (150 g/30 g and 100 μg/20 μg). Withdrawal bleedings are shorter and lighter as compared with women using drospirenone/EE (3 mg/30 μg). The number of women without withdrawal bleeding is approximately 30% after 12 months. Even though its contraindications are identical to other combined oral contraceptives, this nomegestrol acetate/E2 pill should be considered to be of interest for many women.
The combined oral contraceptive pill, containing estrogens and progestins, is more than 50 years old. Gregory Pincus and John Rock showed that doses of over 5 mg of progestin in a 21-day regimen could suppress ovulation but caused unacceptable bleeding [1]. The first pill, Enovid, contained mestranol (150 μg) with norethynodrel (9.85 mg). Mestranol was later replaced by ethinylestradiol (EE; also called 17-α-ethinyl estradiol). Over the years, the dose of EE has decreased from 150 to 15 μg. This decrease has been made possible thanks to the availability of new progestins. Progestins are classically characterized according to their structural origins [2]. Most progestins in oral contraceptive pills (OCPs) are 19 nortestosterone derivatives, including the so-called second- and third-generation OCPs. Some newer progestins have been available more recently in oral contraceptives, such as drospirenone [2]. A different family of progestins used in combined pills is represented by pregnane derivatives, such as chlormadinone acetate and cyproterone acetate [2]. In the different combined pills currently available, the progestin component in the pill inhibits luteinizing hormone (LH) peak, decreases ovarian senstivity to follicle-stimulating hormone (FSH) and therefore decreases estradiol (E2) production, while the estrogenic component regulates endometrium proliferation and compensates estrogenic deficiency induced by the antigonadotropic effect of the progestin.
Although EE has progressively decreased over the years, a low cardiovascular risk persists in women taking combined pills. The risk for venous thromboembolism (VTE) reaches 2–4/10,000 women-years, according to the different pills. It is higher during the first year after the introduction of the pill. The arterial risk, including stroke as well as myocardial infarction, is much lower, reaching 1/100,000 women-year [3]. Several cohort studies have shown that the risk for VTE is lower using second-generation than third-generation progestins [4,5]. The largest cohort comes from Denmark. It has so far included 1,626,528 women aged 15–49 years. Using pills containing the same amount of EE (30 μg), the risk for VTE with desogestrel and gestodene was at least double that of pills containing levonorgestrel [5]. The latest evaluation of this cohort, published in 2012, has shown that VTE risk when using pills containing drospirenone is close to that of pills containing desogestrel or gestodene [5,6]. In many countries, progestin-only pills devoid of cardiovascular risks are available. However, they are usually prescribed to women having contraindications to estrogens, as their efficacy is lower than combined pills and they are not always well-tolerated owing to increased incidence of irregular bleeding and acne compared with OCPs [7].
In order to minimize the cardiovascular risk in women using oral contraceptive drugs, the concept of using the natural 17β-E2 in combined pills has risen in the 1970s. More than 15 different attempts to develop a pill containing 17β-E2 have been made [8–13]. However, no satisfactory combinations have been available for many years. In many cases, the pills containing 17β-E2 were contraceptive but their tolerance was low, as women experienced many bleedings. Monophasic, bi- or tri-phasic combinations have failed over the years.
Overview of the market
Of the 208 million pregnancies that occured worldwide in 2008, 86 million were unintended, resulting in approximately 33 million unplanned births, 41 million abortions and 11 million miscarriages [14]. An estimated 100 million women worldwide use a combined oral contraceptive (COC) [15]. A recent analysis of 172 countries estimated that contraceptive use averted 44% of maternal deaths (272,000 [uncertainty interval 127,900–407,100]), in 2008. Furthermore, meeting the unmet need for family planning could prevent an additional 29% of maternal deaths (104,000) per year [16]. Therefore improvement in contraception use is necessary. COCs represent the most popular form of reversible contraception in the world. However, they have a low but still unacceptable failure rate reaching 1–5%, and second their use is associated with a small cardiovascular risk.
Therefore, in the past several years, the major modifications concerning combined pills have not only been the decrease of the EE concentration, but also the introduction of different regimens in order to improve the pill's efficacy. Different studies have demonstrated that failure of contraceptive pills is due, for the greatest part, to the fact that women forget to take their pills, especially around the steroid-free interval [17]. Therefore, new regimens have been developed in which monthly steroid-free intervals have been shortened, or have been skipped, while placebo pills have been added to some combinations to maintain the routine of daily intake. Another point potentially improving the pill's efficacy might be the half-life of the progestin. In a large US prospective study, Dinger et al. have shown that the effectiveness of the pill was improved when it contained a progestin with a longer half-life [18]. This study included 52,218 women, followed for a period of 3 years. Life-table estimates of contraceptive failure for a 24-day regimen of drospirenone and EE and 21-day regimens of other progestogens were 2.1 and 3.5% after the first study year, and 4.7 and 6.7% after the third year. The 24-day oral contraceptive regimens containing a progestogen with a long half-life show higher contraceptive effectiveness under routine medical conditions compared with conventional 21-day regimens.
A further point in order to improve efficacy is to improve compliance. Therefore a nonoral route of combined contraception has been developed in the past few years [19]. Patches and rings containing EE as well as progestins are now available. However, the thrombotic risk is not decreased, when EE is administered vaginally or transdermally. It could even be higher than using the oral route with the same progestin [20].
The other pill containing E2: E2 valerate/dienogest oral contraceptive pill
The nomegestrol acetate (NOMAC)/E2 pill is the only pill available to date containing natural 17β-E2. Most combined pills contain EE (
Introduction to the compound
This NOMAC/E2 pill is a monophasic pill as in the first 24 pills it contains 1.5 mg of 17β-E2 and 2.5 mg of NOMAC. The four remaining pills are a placebo.
Chemistry
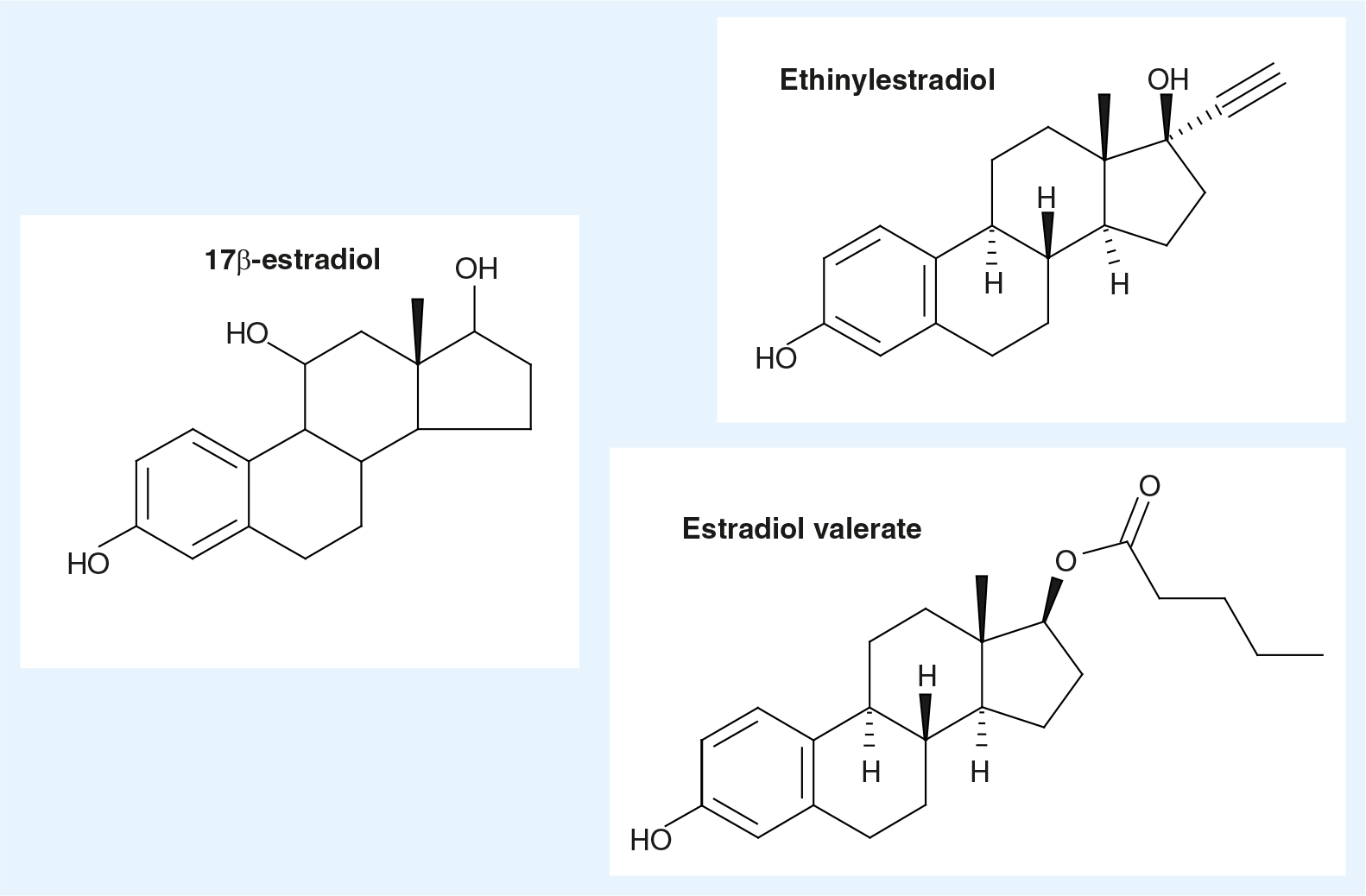
17β-E2
17β-E2 is the main endogenous estrogen in women (
NOMAC
NOMAC is derived from progesterone [25]. It is a 19 norprogesterone derivative (

The progestational potency of progestins is assessed by the McPhail Index, which measures the progestogen dose required for endometrial transformation to a secretory state [27]. By using this method, NOMAC has demonstrated a good progestational activity. Its effect was tested on human endothelial cells. It increases nitric oxide synthesis in human endothelial cells by transcriptional and nontranscriptional mechanisms, whereas medroxyprogesterone acetate lacks such effects [28].
It has a neutral impact on blood sugar levels and on lipid levels.
In order to test its antigonadotropic effect, a dose-finding study using three different doses was conducted. The three doses tested were 1.5, 2.5 and 5 mg in 13 control women during 25 days [29]. FSH and LH serum levels were decreased in the three groups. At a dosage of 1.25 mg/day, NOMAC inhibits ovulation while permitting follicle growth. Therefore, the 2.5-mg dose is the minimal dose necessary to inhibit ovulation as well as folliculogenesis.
Association NOMAC & 17β-E2
The dose-finding studies were initially performed with either NOMAC alone (2.5 mg) or combined with 1.5 mg E2. The dose of 2.5 mg of NOMAC was chosen, according to the study testing its antigonadotropic activity in control women [29]. A dosage of 1.5 mg per day of E2 has been established to achieve physiologic estrogen levels on the basis of an E2 dose range of 1–2 mg per day resulting in steady state E2 levels that range from 30 to 80 pg/ml [30]. Average E2 concentrations achieved by NOMAC/E2 at steady-state are 50 pg/ml, which are comparable to levels observed during the early follicular and late luteal phase of the natural menstrual cycle.
The dose of 1.5 mg of E2 has a synergistic antigonadotropic effect [30].
The NOMAC/E2 combination has been tested according to two different regimens, a 24/4 regimen versus a 21/7 regimen [31,32]. In the 24/4 regimen, 24 pills contain NOMAC/E2 and the remaining four pills contain placebo. In the 21/7, 21 pills are active. A randomized study was performed in 40 women using the 24/4 regimen and 37 women on the 21/7 regimen, respectively. FSH, LH, E2 and progesterone serum levels as well as the main follicular diameter were measured during three cycles. The FSH level was lower and LH inhibition lasted longer in the 24/4 regimen. The 24-day administration showed significantly smaller follicle diameters than on the 21-day regimen (mean ± SD mm in cycle 2: 9.0 ± 3.0 vs 11.3 ± 5.3 [p = 0.02] and in cycle 3: 9.2 ± 3.0 vs 11.5 ± 6.0 [p = 0.04]). This study demonstrates that the 24/4 regimen has more antigonadotropic effects than the 21/7 regimen [32].
Pharmacodynamics
Primary pharmacodynamic studies in vitro are receptor binding studies [33]. They have shown that NOMAC binds with a high affinity to the progesterone receptor in various hormone-sensitive cell lines derived from rat, rabbit or human and transactivates the human progesterone receptor in HeLa and Chinese hamster ovary cells transfected with progesterone receptor B (PRB) [33]. NOMAC showed antiandrogenic activity with an IC value of 92.1 nmol/l. NOMAC does not show antimineralocorticoid activity. Van Diepen et al. have recently reported the progestogen receptor profile, determined in Chinese hamster ovary cells transfected with human PRB; androgen, estrogen (ER-α and ER-β), glucocorticoid and mineralocorticoid receptors [34]. Agonistic activity rankings for PRB was: levonorgestrel (LNG) = NOMAC >> progesterone >> drospirenone (DRSP) > dienogest. No antagonistic activity at PRB was observed. Only LNG had androgenic activity. Anti-androgenic potency rankings were LNG >> NOMAC > progesterone > dienogest > DRSP. All agents were devoid of activity at ER-α, ER-β and glucocorticoid.
In primary pharmacodynamic studies in vivo, NOMAC exhibited the profile of a full progestogen in classical progestagenic bioassays performed in rabbits (McPhail and McGinty tests) and rats [35]. NOMAC induced a high decidual proliferation/differentiation in immature estrogen-primed female rabbits and induced a decidual reaction after trauma of the uterine horn of the rat. NOMAC had a strong antigonadotropic activity, which resulted in an inhibition of spontaneous ovulation in rats and monkeys. The oral ID50 (inhibition of ovulation in 50% of treated animals) was 0.5 and 0.2 mg/kg in rats and monkeys, respectively [34]. Moreover, NOMAC displays antiandrogenic activity, antiestrogenic activity and pituitary inhibitory potency.
In secondary pharmacodynamic studies, NOMAC was tested in combination with E2, using ovariectomized animals in the context of the development of NOMAC in hormone replacement therapy (HRT). The main characteristic of NOMAC is its neutral effect on the beneficial action of E2 in nongenital targets. Combined NOMAC did not interfere with the beneficial effects of E2. NOMAC has a strong progestational and antiestrogenic effect on the uterus and significantly reduced the proliferation that occurs with E2 alone. NOMAC alone has no functional impact on glucid and lipid metabolism at doses up to ten-times higher than the effective dose on bone in rats.
Oral absolute bioavailability in humans of NOMAC from the combination tablet is 63.4%. For E2, the absolute bioavailability is very low (with or without baseline correction) at approximately 1%. NOMAC/E2 has been registered since 2003 for HRT in menopausal women, in several European countries, using the combination of 3.75 mg NOMAC with 1.5 mg E2.
Pharmacokinetics & metabolism
The absorption, distribution, metabolism and excretion of NOMAC have been investigated in several species, especially in rats and monkeys at the time of the development of NOMAC in HRT. No specific pharmacokinetic animal studies were performed with the NOMAC E2 combination.
The metabolism of NOMAC involves CYP450 enzymes. In vitro studies using hepatic microsomes and recombinant CYP450s have shown that several CYPs are involved in the metabolism of NOMAC (CYP3A4/5, CYP2C8 and CYP2C19). NOMAC is extensively metabolized. The metabolism of NOMAC is characterized by hydroxylation reactions followed by conjugation. In vivo excretion/mass balance studies with [14C]-NOMAC were carried out in monkeys and humans. NOMAC drug-related material was observed in both urine and feces. The percentage of total dose recovered in feces was 74, 40–57 and 55–67% of the dose for female rats, monkeys and humans, respectively. The percentage of total dose recovered in urine was 19, 13–41 and 23–41% in rats, monkeys and humans, respectively.
The pharmacokinetic profile of NOMAC and 17β-E2 has been investigated after multiple and single dosing in 23 healthy women [36]. NOMAC reached steady state after 5 days with mean ± standard deviation (SD) trough NOMAC concentration (Cav) of 4.4 ± 1.4 ng/ml. On day 24, mean ± SD peak NOMAC concentration (Cmax 12.3 ± 3.5 ng/ml) was reached in mean 1.5 h (tmax); the mean ± SD elimination half-life was 45.9 ± 15.3 h. On day 24, E2 mean ± SD Cav was 50.3 ± 25.7 pg/ml; mean ± SD Cmax was 86.0 ± 51.3 pg/ml [36].
Clinical efficacy
In order to test the efficacy of a pill, the Pearl index (PI) is measured. It is calculated as the number of unwanted pregnancies occurring among 100 women, treated for a year. According to the Committee for Medicinal Products for Human Use criterion, the upper limit of the 95% confidence interval for the PI should not exceed one. Two main clinical Phase III studies have been performed in order to evaluate NOMAC/E2's efficacy [37,38]. The first one performed in Europe, Asia and Australia is called SAMBA and included 2126 women [37]. The second study, called RUMBA, was performed in North, Central and South America [38]. It included 2200 women from the USA, Canada, Argentina, Brazil, Chile and Mexico. In both studies, women were randomized between NOMAC/E2 and a reference pill, containing drospirenone 3 mg combined with 30 μg of EE. In the first study, the estimated PI for NOMAC/E2 among women aged between 18 and 35 years, was 0.38 (95% CI: 0.10–10.97) versus 0.81 (95% CI: 0.17–12.35) for the reference pill containing drospirenone and EE. In the American study, the Pearl Indices were higher in both groups reaching 1.13 (0.6–1.94) and 1.83 (0.74–3.77) in the NOMAC/E2 and DRSP-EE groups, respectively. The difference in the PIs between the SAMBA and RUMBA studies could be explained by statistically significant differences of study compliances, and the BMI between the two populations. In the American study the discontinuation rate was higher, although comparable to rates observed for other contraceptives evaluated in the USA [38]. Furthermore, the mean BMI was 24.5 ± 4.1, as compared with 23 ± 3.5 in SAMBA study. In summary, in both studies, the efficacy of NOMAC/E2 is at least equal to that of drospirenone-EE.
Postmarketing surveillance
NOMAC/E2 is the first contraceptive pill containing 17β-E2 that received approval from EMA, in July 2011. No postmarketing information is currently available. Thrombotic events will be recorded. NOMAC/E2 is currently under registration in the USA. An international postactive surveillance study will be performed soon to assess and compare, with other COCs, the short- and long-term risk of NOMAC/E2 and, especially, the venous thromboembolism incidence rate.
Safety & tolerability
Metabolism of lipids & carbohydrate
The effects of NOMAC-E2 on lipid and carbohydrate metabolism have been evaluated in a randomized open-label study involving 121 women, in five centers in Finland [39]. Healthy, sexually active women aged 18–50 years with a BMI between 17–29 kg/m2 were randomly assigned to NOMAC E2 in a 24/4 regimen (n = 60) or LNG/EE (150/30 μg) in a 21/7-day regimen (n = 61). LNG/EE (150/30 μg) was used as a comparator based on regulatory guidance for safety evaluation of new COCs [40]. The outcome was the change from baseline to cycle six. No clinically relevant changes were seen in total cholesterol, high-density lipoprotein-C (HDL-C), low-density lipoprotein-C (LDL-C) or total triglycerides among women receiving NOMAC/E2 during six treatment cycles. LNG/EE treatment did not change total cholesterol either, but it decreased HDL-C, increased LDL-C, and increased total triglycerides. The decrease from baseline in HDL-C and the increase from baseline in LDL-C and total triglycerides observed in the LNG/EE group were statistically significantly different from changes observed in the NOMAC/E2 group (p < 0.05). Over six cycles of treatment, women receiving NOMAC/E2 had negligible changes from baseline in the area under the curve and incremental area under the curve for both glucose and insulin. In the LNG/EE group, increases from baseline were observed for all four parameters. The differences between treatment groups were statistically significant for all of these indices (p < 0.002). No changes in HbA1C were observed in either group. In summary, the monophasic COC NOMAC/E2 had less influence on lipids and carbohydrate metabolism than the COC LNG/EE.
Clotting factors
Two double-blind, comparative, randomized studies have evaluated clotting factors. The first study, including 90 subjects, was a monocentric study performed in France, for a period of 3 months [41]. The second study, including 121 subjects, was performed in Finland over a period of 6 months [40]. Both have compared NOMAC/E2 and LNG/EE as levonorgestrel is one of the progestins associated with the lowest risk of venous thrombosis [42]. The comparator contained 20 and 30 μg of EE in the French and the Finnish studies, respectively.
In the French study, after three cycles of treatment with NOMAC/E2, mean prothrombin fragments 1 + 2 levels did not increase with NOMAC/E2 compared with LNG/EE (−0.02 vs +0.08 nM, p < 0.01). Other significant differences between NOMAC/E2 and LNG/EE were mean changes in antithrombin (+0.3 vs −4.4%, p < 0.001), activated protein C resistance normalized ratio (+ 0.2 vs + 0.46, p < 0.01), d-dimer (−53 vs +43 ng/ml, p < 0.001) and plasminogen (+6 vs +30%, p < 0.0001) and plasminogen activator inhibitor-1 (−3.1 vs −8.0 ng/ml, p < 0.001). The NOMAC/E2 regimen has fewer adverse effects on blood biological coagulation and fibrinolysis than LNG/EE [41].
In the Finnish study, after six cycles of treatment, prothrombin fragments 1 + 2 essentially did not change in the NOMAC/E2 group, whereas a small increase in the LNG/EE group was observed (p < 0.085). Although d-dimer was nearly unchanged in both groups, these results are inconclusive because more than 50% of the values were below the limit of detection. The endogenous thrombin potential -based activated protein C sensitivity ratio increased by a statistically significant margin from baseline to cycle six in both groups; however, the change was much greater with LNG/EE than with NOMAC/E2 (p < 0.001). The activated partial thromboplastin time-based sensitivity ratio was nearly unchanged in both groups. Small changes from baseline were observed in the anticoagulatory factors ATIII, protein C, and free and total protein S in both treatment groups, but the between-group differences for these parameters were found to be statistically significant (p < 0.01) except for free protein S. NOMAC/E2 and LNG/EE induced minimal changes from baseline in procoagulatory factors II, VIIa and VIII. For factor VIIc, a minimal change from baseline was observed in the NOMAC/E2 group, whereas a decrease was observed in the LNG/EE group (p = 0.001) [39].
To date, no VTE has occurred in the NOMAC/E2 group in any clinical study. One case of deep VTE was observed in a 28-year-old woman in the drospirenone group. This woman had a heterozygote mutation for factor V and factor II (data transmitted from marketing authorization holder).
Blood pressure
Overall, no mean changes from baseline to the final measurement for either systolic or diastolic blood pressure were observed with NOMAC/E2, over the study period ranging from six to 13 cycles, depending on the studies (data transmitted from marketing authorization holder).
Tolerability & bleeding pattern
In order to assess tolerability and bleeding patterns, two trials have been performed, in healthy, sexually active women (18–50 years) with a BMI of between 17 and 35 kg/m2 who needed contraception and did not plan to use condoms, were included. Women were randomly allocated in a 3:1 ratio to either NOMAC/E2 (2.5/1.5 mg) in a 24/4-day regimen or DRSP/EE (3/30 μg) in a 21/7-day regimen for 13 cycles [37]. In the first trial, participants were recruited from gynecological and/or general practitioner's practices in Europe, Asia and Australia. On average, each of the 95 centers recruited between 20 and 60 women. Out of a total of 2152 women, 1613 were randomized to NOMAC/E2 and 539 to DRSP/EE [37]. In the second trial, women were recruited from North, Central and South America from 89 gynecology and general practitioner practices. Out of a total of 2281, 1710 were randomized to NOMAC/E2 and 571 to DRSP/EE [38].
The vaginal bleeding pattern analysis was performed by a so-called ‘cycle analysis’ based on the bleeding records from an electronic diary. A reference period (RP) analysis was performed in accordance with the WHO and Committee for Medicinal Products for Human Use recommendations [43]. The incidence of amenorrhea (i.e., no bleeding-spotting at all over a consecutive period of 91 days) increased from 8.1% in RP2 to 13.4% in RP4 for NOMAC/E2 users. Amenorrhea was almost absent among users of DRSP/EE (1.1% in RP4). In the cycle analysis breakthrough bleeding/spotting was found to progressively decrease in both groups over the course of the trial. The respective incidences for NOMAC/E2 and DRSP/EE (cycles 4–13) were similar and ranged from 20 to 14% and from 17 to 11%, respectively, and occasionally reached statistical significance between treatments. For women with breakthrough bleeding/spotting, the median number of days per cycle was similar between treatment arms (2–3 days in the NOMAC/E2 group and 1–4 days in the DRSP/EE group). In both treatment groups, the majority (>75%) of breakthrough bleeding/spotting episodes consisted of spotting only. Scheduled withdrawal bleedings were shorter and lighter among users of NOMAC/E2. A progressive increase in the incidence of absence of withdrawal bleeding was observed in the NOMAC/E2 group, ranging from 22 (cycle four) to 31% (cycle 12), which was not observed in the DRSP/EE group (varying between 3 and 6% without particular trend). For women experiencing withdrawal bleeding, the median number of withdrawal bleeding/spotting days was lower when using NOMAC/E2 (range 3–4 days) compared with DRSP/EE (5 days), the difference being caused by the median number of bleeding days, which is 2 days for NOMAC/E2 and 3 days for DRSP/EE. Calculated over the entire trial period for all NOMAC/E2 users and based on evaluable cycles, 43% of women on NOMAC/E2 never missed a withdrawal bleed, while another 21% missed exactly one and another 9% missed two withdrawal bleedings. In summary, the scheduled withdrawal bleedings were shorter and lighter among women using NOMAC/E2, as compared with women using DRSP/EE [37]. The same results have been observed in the American trial [38]. By the end of the trial, shorter, lighter scheduled bleeding or an absence of scheduled bleeding occurred with greater frequency (32.9%) in the investigational group, whereas unscheduled bleeding or spotting episodes were low (16.2%).
During the clinical trials, approximately 80% of all participants reported one or more adverse events (AEs) during the in-treatment period. The percentage was similar between both groups. In the NOMAC/E2 and DRSP/EE groups, 51.2 and 37.0% of the women, respectively, had AEs that were determined by the investigator to be treatment related.
The most frequently reported treatment-related AEs (related incidence ≥5%) were acne, irregular withdrawal bleeding, weight increase and headache. In the European study, the respective discontinuation rates for NOMAC/E2 and DRSP/EE were 3.3 versus 0.2% for acne, 4.0 versus 0.7% for irregular bleeding and 1.4 versus 0.7% for weight increase. In the American study, acne and weight gain accounted for 13.5 and 8.3% of discontinuations, respectively, in the NOMAC/E2 group. Concerning acne, in the American study, most participants who did not have acne at baseline also were free from acne at last measurement (87.6% in the NOMAC/E2 versus 95.8% in DRSP/EE). Overall, the presence of acne compared with baseline decreased over time for both treatments. However, there were more cases of acne in women receiving NOMAC/E2 (12.4%) than in those receiving DRSP/EE (4.2%). Differences in change of acne from baseline to last measurement were in favor of DRSP/EE (p < 0.001). Those results have been confirmed in the trial from Europe.
Women on NOMAC/E2 experienced a small increase in mean body weight (i.e., from 63.4 kg at baseline to 64.4 kg at last measurement); women on DRSP/EE increased from 63.7 kg at baseline to 64.0 kg at last measurement. The change from baseline in weight at last measurement was statistically significant between NOMAC/E2 and DRSP/EE (p = 0.001) [37]. A relative increase (at least 7% in body weight) was estimated during the treatment period for 16% of the subjects in the NOMAC E2 group and for 11% of the subjects in the DRSP EE group. In the American study, the modest increase in weight from baseline until last measurement was significant in both groups (p = 0.001). Weight increased from 65.8 kg at baseline to 66.7 kg (median 1 kg) and 65.8 to 66 kg (median 0.2 kg) at last measurement in the NOMAC/E2 and DRSP/EE groups, respectively.
Of the total clinical population, 1.3% of women taking NOMAC/E2 versus 1.7% of women taking DRSP-EE experienced breast pain that was considered by investigators to be treatment related. Breast tenderness was reported in 0.8 versus 1.2%, respectively. No women left the study as a result of breast pain.
As NOMAC has an antigonadotropic effect, even though 1.5 mg E2 is present in NOMAC/E2, a study evaluated bone mineral density [44]. No clinically relevant effect on bone mineral density at the lumbar spine and femoral neck and no statistically significant difference in the effect on bone mineral density between NOMAC-E2 and the LNG-EE, was observed in women aged 21–35 years and treated for 26 cycles. However, the population of women aged 21–35 years cannot be compared with the post-menarcheal adolescent. Indeed, for women aged 21–35 years the peak bone mass is already reached and the bone turnover is limited. These results cannot be referred directly to adolescents [44].
Regulatory affairs
NOMAC/E2 was approved in EU, marketing at the end of 2011. It is currently approved in Australia, New Zealand, Russia, Colombia and Switzerland.
Discussion
Contraception is hard to achieve all over the world. In 2012, many pregnancies are still unintended. A recent prospective American study has shown that low socioeconomic status and low educational level are directly linked to an increased rate of undesired pregnancies [45]. This study showed that long-acting contraceptives such as intrauterine device are associated with 20-times less contraceptive failure, even in women less than 21 years of age. However, many women or their partners refuse to have intrauterine devices and/or prefer short-term contraception such as combined pills. It remains the most used contraception worldwide after condom use. Therefore having a pill containing 17β-E2 can represent a real opportunity for women's health. This pill has a good Pearl index. As it is monophasic, it is easier to use than its comparator containing E2 valerate, which is a quadriphasic pill, especially in case of missed pill. A recent Cochrane database review has compared quadriphasic contraceptive pills with monophasic contraceptive pills. The conclusion was that available evidence is insufficient to determine whether quadriphasic pills differ from monophasic oral contraceptives in contraceptive effectiveness, bleeding pattern, minor side effects and acceptability [46].
NOMAC/E2 uses a continuous regimen minimizing the risk of forgetting pills. Furthermore, as the progestin NOMAC has a long half-life reaching 46 h, the efficacy of the NOMAC-E2 pill might be maintained even if a pill is forgotten. Furthermore, data in several studies suggest that this pill induces few metabolic changes. As this pill is rather neutral on glycemia, lipids and tension, it could be used in overweight women, women with polycystic ovarian syndrome or women with diabetes. However, no data are available to date in overweight women, nor in women with polycystic ovarian syndrome or diabetic women. Although data are rather reassuring in the different clinical trials, this pill should not be prescribed to women with a significantly increased cardiovascular risk. It is important to remember that contraindications of this pill containing 17β-E2 are the same as other combined pills.
Conclusion
NOMAC/E2 is the first oral contraceptive pill containing 17β-E2. This monophasic pill contains 1.5 mg of 17β-E2 and 2.5 mg of NOMAC, on a 24/4 regimen. Its efficacy is at least equal to that of drospirenone/EE and the cycle control of NOMAC/E2 is characterized by shorter and lighter withdrawal bleeding episodes, which sometimes do not occur at all. This pill provides the metabolic and hemostatic profile expected from an E2 pill, with good contraceptive efficacy, and without compromising cycle control and acceptability for women. However, although this pill might be safer based on its low impact on metabolic and hemostatic variables, prescribers should be careful, especially in women having increased cardiovascular risk.
Future perspective
The era of contraception using 17β-E2 instead of EE has started with this pill containing 1.5 mg of E2 and 2.5 mg of NOMAC. The use of 17β-E2 is currently being developed in patches as well as in vaginal rings. Studies are needed to prove a lack of increased thrombotic risk using these different routes of contraception. The ideal contraception would have very high efficacy without cardiovascular risk. Furthermore, educational programs should be developed as failures of contraceptive pills are often linked to their misuse.
Financial & competing interests disclosure
S Christin-Maitre has been involved in the clinical study testing the 21/7 or 24/4 regimens of the nomegestrol acetate/E2 pill. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Executive summary
The combined oral contraceptive (COC) pill, containing estrogens and progestins, is 50 years old.
Most COCs contain ethinylestradiol (EE).
Due to cardiovascular risk in women using oral contraceptive drugs, the dose of EE has been decreased over the years.
In order to minimize the cardiovascular risk in women using oral contraceptive drugs, the concept of using the natural 17β-estradiol (E2) in combined pills arose in the 1970s.
Many trials of pills containing 17β-E2 have failed as tolerance was low and women experienced many bleedings.
Nomegestrol acetate (NOMAC)/E2 is the first monophasic pill containing 17β-E2.
Of the 208 million pregnancies worldwide, 86 million were unintended, resulting in approximately 33 million unplanned births, 41 million abortions and 11 million miscarriages. Significant progress has to be made concerning contraception.
An estimated 100 million women worldwide use COCs.
This NOMAC/E2 pill is a monophasic pill as the first 24 pills contain 1.5 mg of 17β-E2 and 2.5 mg of NOMAC. The four remaining pills are placebos.
17β-E2 is the main endogenous estrogen in women.
17β-E2 has less impact on liver functions, as it increases sex hormone-binding globulin, transcortin and angiotensinogen 600–, 500– and 350-times, respectively, less than EE.
NOMAC is derived from progesterone; it is a 19 norprogesterone derivative.
NOMAC binds with high affinity to the progesterone receptor. It has no estrogenic, androgenic, mineralocorticoid or glucocorticoid effects; it has a moderate antiandrogenic effect.
The 2.5-mg dose of NOMAC is the minimal dose necessary to inhibit ovulation as well as folliculogenesis.
Oral absolute bioavailability in humans of NOMAC from the combination tablet is high, reaching 63.4%.
The metabolism of NOMAC involves CYP450 enzymes.
The mean ± standard deviation elimination half-life of NOMAC in women treated with NOMAC/E2 is 45.9 ± 15.3 h.
The E2 serum level of women treated with NOMAC/E2 is similar to the E2 serum level during a follicular phase.
The efficacy of NOMAC/E2 is at least equal to that of drospirenone/EE.
The estimated Pearl index for NOMAC/E2 among women aged between 18 and 35 years is 0.38 (0.10–10.97) in a study from Europe, Australia and Asia.
The Pearl Indices are 1.13 (0.6–1.94) and 1.83 (0.74–3.77) in the NOMAC/E2 and DRSP-EE groups, respectively, in the American study. This difference in Pearl index is probably related to the compliance rate, which was lower in this study than in the previous study.
No significant changes were seen in total cholesterol, high-density lipoprotein C, low-density lipoprotein C or total triglycerides among women receiving NOMAC/E2 during six treatment cycles.
NOMAC/E2 has less influence on carbohydrate metabolism than COC levonorgestrel (LNG)/EE.
The NOMAC/E2 regimen has fewer adverse effects on blood biological coagulation and fibrinolysis than LNG/EE.
No mean changes from baseline to the final measurement for either systolic or diastolic blood pressure was observed with NOMAC/E2.
Women on NOMAC/E2 have shorter, lighter scheduled bleeding or an absence of scheduled bleeding (~30%). The frequencies of scheduled bleeding or spotting episodes are low (~12%).
The most frequently reported treatment-related AEs (related incidence >5%) are acne, withdrawal bleeding, weight increase and headache.
NOMAC/E2 has been approved in the EU, it was launched into the at the end of 2011. It is currently approved in Australia, New Zealand, Russia, Colombia and Switzerland.
NOMAC/E2 is the first pill containing the endogenous E2, 17β-E2.
The efficacy of NOMAC/E2 is good.
This pill has less metabolic impacts than pills containing LNG, it is well tolerated and is associated with decreased bleeding.
An international postactive surveillance study will be performed to assess and compare with other COCs, the short- and long-term risk of NOMAC/E2 and especially venous thromboembolism incidence rate.