
Abstract
Ovarian cancer can be treated with a very good prognosis if detected in the early stages, but not after it has advanced. Transvaginal ultrasound is capable of identifying changes in ovarian size and structure, and thereby detects early ovarian malignancies. This view has generated four major trials on transvaginal ultrasound detection: the Kentucky, PLCO, UKCTOCS, and SCSOCS trials. Each is sufficiently different to warrant examination. The Kentucky, UKCTOCS and SCSOCS trials report a shift to early stage detection. The Kentucky trial reports a survival benefit, while follow-up survival analysis is pending in the UKCTOCS and SCSOCS trials. Details of these trials are presented including definitions, inclusions/exclusions, analytic structure (intention-to-treat vs per protocol), performance (sensitivity, specificity, positive predictive value and negative predictive value), extent of screening-related treatment, time from screening to treatment, length of follow-up and survival versus mortality analysis. Questions are answered here about effectiveness, application, prevalence, cost and the potential for harm.
 Medscape: Continuing Medical Education Online
Medscape: Continuing Medical Education Online
This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Medscape, LLC and Future Medicine Ltd. Medscape, LLC is accredited by the ACCME to provide continuing medical education for physicians.
Medscape, LLC designates this Journal-based CME activity for a maximum of
All other clinicians completing this activity will be issued a certificate of participation. To participate in this journal CME activity: (1) review the learning objectives and author disclosures; (2) study the education content; (3) take the post-test with a 70% minimum passing score and complete the evaluation at www.medscape.org/journal/wh; (4) view/print certificate
Learning objectives
Upon completion of this activity, participants should be able to:
Assess the epidemiology and mortality risk of ovarian cancer
Distinguish the number of successful trials of transvaginal ultrasound to screen for ovarian cancer
Analyze the accuracy of transvaginal ultrasound to detect ovarian tumors and cancer
Evaluate the methods and results of the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial
Screening involves the examination of healthy individuals before any signs of disease become evident. By contrast, a diagnostic workup is appropriate whenever signs of disease are present in order to determine cause. Early stage ovarian cancers occur predominately without specific symptoms [1,2] and if discovered are highly curable with surgery and conventional chemotherapy, in contrast to late stage disease, which carries a poor prognosis despite radical tumor debulking and multiple courses of combination chemotherapy. Ovarian cancer is considered a ‘silent killer’ because there are often few signs of it until it reaches an advanced stage. Because ovarian malignancies claim more lives than all other gynecologic malignancies combined in the USA, it is imperative to try to detect this disease in an early stage of development through screening. The scope of this paper is focused on the detection of early stage ovarian tumors using transvaginal ultrasonography.
Screening
There are important tenets for screening [3,4]. Screening is appropriate for disease that is grave and threatens well-being; and curable if found early. The screening tool must be effective in finding disease that can be treated successfully and in not reporting that disease is present when it is not. It should be easy to administer and well-tolerated.
In addition, there are several considerations that are often incorporated into discussions about screening, but differ by disease and are considered here in the context of ovarian cancer.
The disease significantly impacts public health
Key to this consideration is the interpretation of ‘significantly impacts’. Diseases associated with mortality would appear to satisfy this criterion, but interpretations based on age can weight the significance in favor of earlier age risk. When prevalence is considered, it is often found to increase with age, as would disease-specific mortality. This leads to several dilemmas:
What weight should be given to significance when increased risk occurs at 50 years of age versus older ages of 60, 70 or 80 years when life expectancy is declining?
Should risk be based on the entire age population or gated for age group risk?
Is the probability of disease-specific death (as a function of all deaths or grouped deaths like cancer-specific deaths) more related to significance than prevalence?
Should the quality and cost of end-of-life experiences be included in considerations of significance in terms of avoiding extended palliative care as well as suffering and death? [5]
Should achievable cost savings be considered as part of significant impact? Significant impact: ovarian cancer kills more women than all other gynecologic malignancies combined and is associated with vastly lower costs of care in early stages than advanced stages [6] where outcomes are poor and suffering prolonged.
The disease has a high-to-intermediate probability of occurrence in the population
High and intermediate probabilities are very subjective and are often used in the absence of evidence-based findings. Ovarian cancer is one of the top five causes of cancer death for US women [7]. Over 15,500 US women will lose their lives to the disease this year and 22,280 will learn that they have ovarian cancer [7]. By way of comparison, 229,060 women will be diagnosed with breast cancer and 39,510 will die from it, showing that ovarian cancer is ten-times less prevalent, but it will kill as many as 40% of the number dying of breast cancer [7]. Thus, the expected mortality ratio for ovarian cancer (15,500:22,280 = 69.6%) is fourfold greater than the expected mortality ratio for breast cancer (39,510:229,060 = 17.2%).
The probability of occurrence and prevalence is dwarfed by the high mortality rate of ovarian cancer.
A critical point for disease detection must exist
Postulate that the screened patient is asymptomatic before a critical point, that the critical point occurs before clinical diagnosis and that diagnosis would not otherwise occur early before the critical point. Importantly, the critical point must occur early enough to achieve a favorable outcome or cure. Because treatment of lung cancer cannot be started early enough to achieve a cure, the critical point occurs too early, while it occurs too late for endometrial cancer, since abnormal uterine bleeding provides a natural early warning system.
Ovarian cancer meets all of the critical point criteria.
Medical care is available if screening is positive
In a global sense, surgery is widely available, as is chemotherapy. On an individual basis, surgery for gynecologic cancer is elective and each case takes its place in the operating room queue. We stick to the position that delays should be kept to a minimum in order to keep ovarian disease from progressing to a stage that is less treatable [8]. Thus, it is imperative that screening sites have active roles in facilitating the scheduling of surgery. Availability of surgery and chemotherapy (surgery alone for low grade stage IA malignancy or surgery and chemotherapy for all else) for women in rural areas presents a challenge. Having surgery far from home and returning for chemotherapy is difficult.
Effective treatment and medical care exists for women with early stage ovarian cancer detected by screening with women in rural areas facing a burden of traveling to access medical care.
Patients are willing & able to undergo further evaluation & treatment
Since screening has no value if there is not subsequent diagnosis followed by treatment, it is important that encouraging support facilitates moving forward. For the woman without medical insurance this facilitation includes financial counseling.
Our extensive experience with over 37,000 women who received over 200,000 screens indicates that it has been possible to treat all women that had a transvaginal ultrasound (TVS) screen indicative of malignancy, regardless of having medical insurance.
Ultrasonography
The first efforts to identify ovarian tumors using ultrasound were reported by Campbell et al. [9]. These efforts employed abdominal ultrasound, but this abdominal approach was less accurate in defining ovarian details because the distance from the probe to the ovaries is large and includes significant airspace in which soundwaves attenuate. In TVS, the probe has a closer proximity to pelvic structures since most of the pelvic anatomy of interest is within 9 cm of the vaginal fornices. TVS use originated with fertility medicine in the mid-1980s [10–12], and was adapted to imaging ovarian pathology before the decade ended [13,14]. TVS with Doppler blood flow imaging and power Doppler is used to evaluate blood flow to ovarian tumors and to identify patterns of flow associated with ovarian neoplasia.
Factors for evaluating tumor detection performance
Factors used for evaluation are: true positives (TP; surgically confirmed malignancy after a positive screening test), true negatives (TN; no malignancy reported during the 365 days following a negative screen), false positives (FP; no malignancy at surgery after a positive screening test) and false negatives or interval cancers (FN; malignancy diagnosed within 365 days of a negative screen). Sensitivity is calculated to determine performance when disease is present (TP/[TP + FN]), while specificity is estimated to determine performance when the disease is absent (TN/[TN + FP]). The positive predictive value (PPV) is calculated to determine how many of those that test positive (TP/[TP + FP]) really have ovarian cancer, while the negative predictive value is calculated to determine how many that test negative really do not have ovarian cancer (TN/[TN + FN]). The greater these estimates are, the higher is tumor detection performance. Ovarian tumors of low malignant potential (LMP) are biologically less aggressive than invasive ovarian malignancies, but are counted as TPs because of their potential to spread beyond the ovary. LMPs rarely recur as invasive cancer, but those having micropapillary projections and/or those associated with peritoneal implants present a greater risk to women [15,16]. Tumor progression comprises a continuum that includes ovarian tumors of LMP [17] and indicates the potential involvement of LMPs in malignant progression, especially since K-RAS or B-RAF mutations of low grade serous carcinoma are also found in serous ovarian tumors of LMP [15]. Further supporting the continuum of progression is the finding that ~60% of low grade serous carcinomas contain areas of serous tumor of LMP [18]. Moreover, a serous ovarian tumor of LMP with extreme architectural complexity can be difficult to distinguish from a low-grade serous carcinoma resulting in significant interobserver variation among histopathologists in clinical classifications [15]. Large mucinous ovarian tumors of LMP may be difficult to adequately sample, so there is a risk of missing some small focus of malignancy [15]. Importantly, serous and mucinous ovarian tumors of LMP can be lethal [16,19]. Fallopian tube malignancies are considered as ovarian malignancies in three trials summarized here, while peritoneal cancers are excluded because they are not visualized by TVS. This exclusion has little impact on performance estimates because peritoneal cancer incidence is 5.7% that of ovarian cancer [20]. Thus, the approach in these trials is to include ovarian tumors that present a risk of malignancy and to exclude from performance evaluations malignancies that cannot be detected by TVS.
Evaluating the effect of ovarian tumor detection on survival
The evaluations of tumor detection performance can be made at any time point; however, the effect of this detection on disease-specific survival needs to be made only after sufficient time has passed for mortalities to have occurred. Estimates should include the survival of all ovarian malignancies in the screened group (i.e., both TPs and FNs). We have taken the position that ovarian tumors of LMP should be excluded from survival analysis so that the included cases reflect the effects on ovarian malignancies with the highest mortality risk. In the context of survival analysis, the comparison or control group warrants some consideration. There are two alternatives that must be considered. First, the survival of all screened cancers should be compared with the survival of all unscreened cancers representing the same region and time frame as those in the screened group. In the second alternative, all individuals in the screening group should be compared with all individuals in a group that hasn't been screened. Because there will be a relatively small number of cancers compared with a very large fraction of women without cancer, it will be difficult to detect significant differences between the groups, making the second alternative less favorable. It is best to use life tables from the Kaplan–Meier analyses to obtain numeric values of survival for screened subjects and unscreened members of the comparison groups, including error estimates, while overall significance for the effect of ovarian tumor detection on survival can be decided through Kaplan–Meier analysis that compares the screened and unscreened comparison group. Finally, in order to be sure that unknown ovarian cancer deaths do not exist, all participants must be checked for living versus dead status using, for example, the Social Security Death Index and then cause of death, determined through vital statistics and hospital records. Evidence of disease is the most significant single factor for assigning death due to ovarian cancer, especially since older members may succumb to other conditions and diseases. Consideration of a trial with participants randomized to intervention (screened) and control (unscreened) groups is appropriate. In the case of screening, the definition of the intervention group must extend beyond the initial randomized assignment to include both screening and, when deemed necessary by screening, expeditious diagnosis and treatment. While the unscreened definition of the control group may appear straightforward, this group has identities established by more than randomization to not receiving screening. For example, the identity of this group may not be the same as the screened group with regard to health conscious members who stay the course of the study, or members of the control group that cannot seek or receive ‘normal’ care. In studies where there is a low probability of the event occurring in each group (i.e., ovarian cancer), it may be difficult to achieve statistical significance. This difficulty can be circumvented by using a population control group where its large numbers can make significant contributions to the power of statistical comparisons. While randomized controlled trials are very powerful, there are settings that challenge them and ovarian cancer screening can be one of these settings.
Framework & findings: results from trials using ultrasound for the early detection of ovarian tumors
There are four published trials that summarize findings on the use of ultrasound for the early detection of ovarian tumors: the Kentucky trial [21], the PLCO trial [22], the UKCTOCS [23] and the SCSOCS trial [24]. It should be noted that a separate UKFOCSS for high-risk women is underway in the UK. These trials have some similarities, but also have significant differences and, accordingly, are deconstructed and summarized in
Summary deconstruction of trials using ultrasound for the early detection of ovarian tumors.
Subset group that received both TVS and CA-125.
Based on TP of 63 for all detected malignancies.
Based on TP of 45 for primary ovarian and fallopian tube malignancies.
CA-125: Cancer antigen 125; EOC: Epithelial ovarian cancer; FN: False negative; FP: False positive; LMP: Low malignant potential; NPV: Negative predictive value
PPV: Positive predictive value; TN: True negative; TP: True positive; TVS: Transvaginal ultrasound.
Together, the Kentucky, UKCTOCS and SCSOCS trials seemed to be more similar in their findings while the PLCO seemed more discordant. Because differences are reported in the PLCO trial with respect to the detection of early stage disease and to extended/improved survival, discussion here is focused at understanding the PLCO trial.
The PLCO trial
In the screening arm of the PLCO Trial, 39,105 women were enrolled with recruiting at different times over an eight year period (
PLCO survival analysis
The PLCO Trial reported 212 ovarian cancer cases observed during the screening portion and during the postscreening follow-up portion (
Mortality in the group screened in the Kentucky Trial.
Recovered dollars and equivalent screens by preventing progression to stage III ovarian cancer.
[A]: Unit case cost based on collections as reported ([a] and [b]) for Stage IIIC cases [6]. Avastin expense alone is based on the literature [e] [41]. The total estimate for care includes Avastin ([f] = [c] + [e]). A total of 76 ovarian malignancies have been culled to the 33 early-stage epithelial ovarian malignancies detected here ([B]: 22 Stage I and 11 Stage II) and further reduced to 28, which represents eliminating five cases that would be found without screening using the percentage of Stage I and II epithelial ovarian cancer that occurs for unscreened women in the Kentucky Cancer Registry (18.8% stage I and 8.6% stage II). We take these 28 as a set representing cases that have been prevented from progressing to Stage III by screening. The cost of these cases is then calculated as if they had progressed to Stage III by multiplying unit costs in column [A] by 28. [C]: Conversion to 2011 dollars (2006 base cf = 0.897, 2010 base cf = 0.969) [101]. [D]: Screen equivalents of expenses in C based on $40/screen [39,40]. [E]: Adjustment for false positives = 447 as previously reported [21]. This adjustment is based on $7000 collections/case as 78,225 screen equivalents at $40/screen ([447 × $7000]/$40 = 78225). False positives surgical cost is estimated at a charge for BSO at ~$18800 and an average collection rate of 34%, which was rounded to $7000. [F]: Adjustment for achieving a PPV = 20.2% as reported [21] that would yield false positives = 300 at $7000/case resulting in 52,542 screen equivalents at $40/screen ([300 × $7000]/$40 = 52,542).
FP: False positive; PPV: Positive predictive value; NA: Not applicable; SEM: Standard error of the mean.
Detection reported in the PLCO trial
In Table 2 of the recent PLCO trial report [22] detection in the intervention group (i.e., the group screened) is summarized as screen-detected cases during (n = 20 + 53 = 73) and after screening (n = 78) including 37 interval cancers (i.e., false negatives) and as never-screened cases during and after screening (n = 16 + 8 = 24) for a total of 212 ovarian cancers reported. First, it is hard to reconcile including 24 never-screened cases in the results summarized for the screening group in Tables 2–4 of the PLCO report [22], as well as in survival analysis shown in PLCO Figure 2 [22]. Second, by isolating the events of the screening period from those in the follow-up period because of the follow-up cases that may have begun well after screening as described above, it is possible to estimate the sensitivity of cases identified during screening as 66.4% (TP/[TP + FN] = [20 + 53]/[20 + + 37]). This is low sensitivity and compares quite unfavorably with the other screening trials in
There are four factors that account for the failure of the PLCO trial to detect early stage ovarian cancer. First, is the use of CA-125 alone. Second, is the inclusion of never-screened participants in the intervention group. Third is the inclusion of the never-treated group of women in survival analysis of the screened group because they couldn't possibly receive a benefit of early detection that would improve their survival. Fourth, is the appearance of ovarian malignancies very long after screening in the extended follow-up period. These failures enrich the screen-detected cases with late stage disease, which will have a poorer survival. Including cases that did not receive treatment or cases that may have started in the extended postscreening follow-up period pushes the survival of the PLCO screening/intervention group lower and makes it indistinguishable from the control group.
Others too have reviewed the PLCO report and outlined the critical flaws of this screening approach. Specifically, ‘important limitations’ have been noted [26] and that the PLCO is “not the definitive answer on ovarian screening using these techniques” [27]. With regard to the mortality end point in the PLCO trial, “Basing decisions on the outcome of death ignores vital dimensions of life that are not easily qualified … There is more to life than death” [28]. Moreover, in contrast to serial TVS with morphology indexing, the single trigger approach in the PLCO trial for identifying sonographic positive screens resulted in a high rate of FPs. Although the PLCO trial constitutes an effort that failed to demonstrate benefits from the screening approach taken, we have presented evidence here from screening approaches that have been executed differently, which might benefit practitioners by showing the highly positive sensitivity and specificity results from three trials in which shifts to the detection of early stage disease occur.
Questions worthy of discussion
Is the early detection of ovarian tumors using ultrasound effective?
Improvement in survival is the best way to assess the effectiveness of the early detection of ovarian tumors using ultrasound. Three of the four trials reported a shift to the detection of early stage disease and follow-up for the effect on survival is still underway for two of these three. It is not surprising that the failure to detect early stage disease in the PLCO trial resulted in similar mortalities in the intervention and usual care groups. Importantly, analysis of survival must be realized as distinct from analysis of mortality. A disease-specific survival analysis will reveal an interval benefit of the intervention group relative to the comparison group. This interval benefit is greatest in the Kentucky trial for a 10-year interval and is followed by a constant continuing benefit in survival as shown in an updated survival analysis in

All-cause mortality was determined and reported in the PLCO trial demonstrating 8.5% deaths in the screening group. In the Kentucky trial, 5.2% of the group screened have died from causes that are summarized in
Are there differences in the application of an ultrasound screening algorithm that would affect screening results?
Delaying diagnosis and treatment on screen-detected cases would allow early stage disease to progress. The PLCO trial allowed up to 9 months for diagnostic evaluation [22]. In the Kentucky trial, 73% of the TPs received surgery within 30 days of their last suspicious screen (mean = 32 ± 4.5 days; median = 16 days, unreported). The number of surgical FPs was higher in the PLCO trial (

Is the prevalence of ovarian cancer fatal to screening?
It is often stated that the prevalence of ovarian cancer, which is approximately seven-times lower than breast cancer, presents a limitation that cannot be overcome even by very high sensitivity and specificity [31]. The Kentucky trial reports a PPV of 20.2% (
It should be realized that prevalence may be used to infer that too many cancer-free cases must be screened for each malignancy so that the issue of prevalence is really a cost issue.
We have previously reported the costs of stage IIIC ovarian cancer [6]. Preventing progression is the important outcome of TVS screening, not only in terms of the survival advantage that is gained, but also in terms of cost savings. Using collections at this institution as the basis for the cost of care for stage III ovarian cancer [6] (
Missing from the estimates presented here is the value of life lost due to cancer. The economic burden of OvCA is very high (~$28 billion/year [42]), translating to $1.8 million for each of the 15,500 US women that will succumb from OvCA in 2012 making the economic gain achieved by preventing one OvCA death enough to pay for 45,000 screens. The value of life lost is expected to increase 48.1% by 2020 [42] so that the value of lives lost continues to shift economics in favor of ovarian screening. Preventing of ovarian cancer deaths considered in terms of the value of life lost more than pays for the cost of screening, even at the Medicare reimbursement rate (CPT 76856: $151.47).
Does screening for ovarian tumors with ultrasound do more harm than good?
The title of a recent article took the position that “Screening Women for Ovarian Cancer Still Does More Harm Than Good [31],” being prompted by results in the PLCO trial report [22]. Regarding this question, neither ‘harm’ nor ‘good’ were defined or evaluated in the PLCO trial. Factors to be considered regarding this question are the ovarian screen itself, which is very well tolerated [43] and one of the things women overwhelmingly have indicated they want [44]. The risk of a suspicious TVS study leading to surgery and a FP outcome have already been discussed here, being similar to clinical benchmarks. Complications occur in surgery and can be graded with regard to their seriousness [45]. In the PLCO trial, complications were not graded and consequently the question of harm due to serious high-grade complications was not addressed. Nonphysical or psychological harm to women has been and continues to be examined with women in the Kentucky trial. When compared with an age and education matched group with no history of ovarian screening, women in the Kentucky trial had more ovarian cancer-specific distress/anxiety, less optimism and less knowledge about risk factors upon entry [46]. Thus, some distress or anxiety relative to ovarian cancer appears to play a motivating role for entering the Kentucky screening trial. As part of these efforts, the validity of self-reporting by women in the Kentucky trial was evaluated and found to be very high [47]. In a study with baseline, 2-week and 4-month measurement, recipients of a normal ovarian screening examination showed decreased ovarian cancer-related distress, increased positive effect and increased knowledge of risk factors [48], indicating that for the vast majority of women screened there are beneficial effects on ovarian cancer-specific anxiety, attitude and knowledge. Women who received an abnormal TVS screening result were found to have an elevated ovarian cancer-specific distress (but not general distress) at 2-week follow-up that returned to baseline at the 4-month follow-up [49]. Results were influenced by a monitoring coping style, low optimism and family history of ovarian cancer. Needs that have been identified in women with an abnormal TVS screening result deal with anticipation, emotional responses, role of the sonographer and impact of prior cancer experiences [50]. In examining social cognitive processing versus cognitive social health processing after an abnormal TVS screening, analyses found that greater distress was associated with greater social constraint [51]. Thus, psychological conditions that are apparently associated with ovarian screening are governed by different underlying factors in different women and not the screening result per se.
Future perspective
For the reader concluding that the ability to detect early ovarian cancers with TVS is very good, but has reservations about four to five screen-detected benign cases reaching surgery for every malignancy, the future rests on improvements to the PPV. Some of this improvement will come as confidence builds in making use of serial TVS with morphology indexing to allow for the resolution of ovarian structure interpreted as abnormal by TVS, and thus reduce the number of abnormal results going to surgery. Improvements may also arise as new biomarkers are used in conjunction with TVS to separate the identities of malignancies requiring surgery from those abnormalities that do not. Likewise, serial rises in serum biomarkers may be identified to be used as a prerequisite for surgery.
For readers concluding that the ability to detect early ovarian cancers with TVS is not very good, the future will depend on innovation and biodiscoveries of new ways to proceed.
For both of these groups, the changes that will accompany the Patient Protection and Affordable Care Act (PPACA) will be absolutely determinate for the future of ovarian cancer screening with TVS in the USA. Price and cost will likely be major drivers upon implementation of PPACA so that systems not only have the lowest unit costs, but also can be delivered with aggregate lowest cost will be the best candidates for acceptance. This is likely to mean that screening centers that are able to always achieve capacity screening will need to come into creation. Detection of ovarian tumors with TVS is very amenable to the screening center approach, as indicated by the Kentucky trial experience. Importantly, with the caregiver shortage that is anticipated when the PPACA brings access to at least a third more Americans, a screening center approach is likely to dove-tail well with new ways of providing care with efficiency of scale. A reasonable expectation is that results from follow-up in both the UKCTOCS and SCSOCS trials will demonstrate a survival benefit because both trials have demonstrated a shift to early stage disease. Application in Europe will fit well with a screening center approach through national health services. In light of much poorer ovarian cancer survivals in the UK relative to Canada and Australia [52], approaches that identify early stage disease with good prognosis will be capable of bringing needed improvement in ovarian cancer survival in these countries.
Executive summary
Screening is appropriate for disease that is grave and threatens well-being, and is curable if found early.
The screening method must be effective in finding disease that can be treated successfully.
Survival estimates need to be made only after sufficient time has passed for mortalities to have occurred.
Only cases that reflect the highest mortality risk should be included in survival analysis so that tumors with low malignant potentials are excluded.
Survival estimates should include both true positives and false negatives in the screened group.
The living versus dead status of all screening participants should be determined and cause of death established.
Kaplan–Meier survival analysis yields the most powerful method for comparing screened with unscreened groups.
Similarities and differences exist in different trials with regard to population control versus randomized control and intent-to-treat versus per protocol analysis.
Three of the trials (Kentucky [70%], UKCTOCS [50%], SCSOCS [67%]) detected a significant shift to the discovery of early stage I and II disease, while one did not (PLCO [28%]).
High sensitivity ranging from 80–89% was achieved by these three trials, as well as high specificity >98%.
Positive predictive value was highest in the SCSOCS (47%) and Kentucky (20%) trials indicating, that one to four women without malignancy received surgery for each woman with a malignancy.
A majority of aggressive type II ovarian cancers were detected in each trial.
The Kentucky trial found a significant survival benefit, while the PLCO did not.
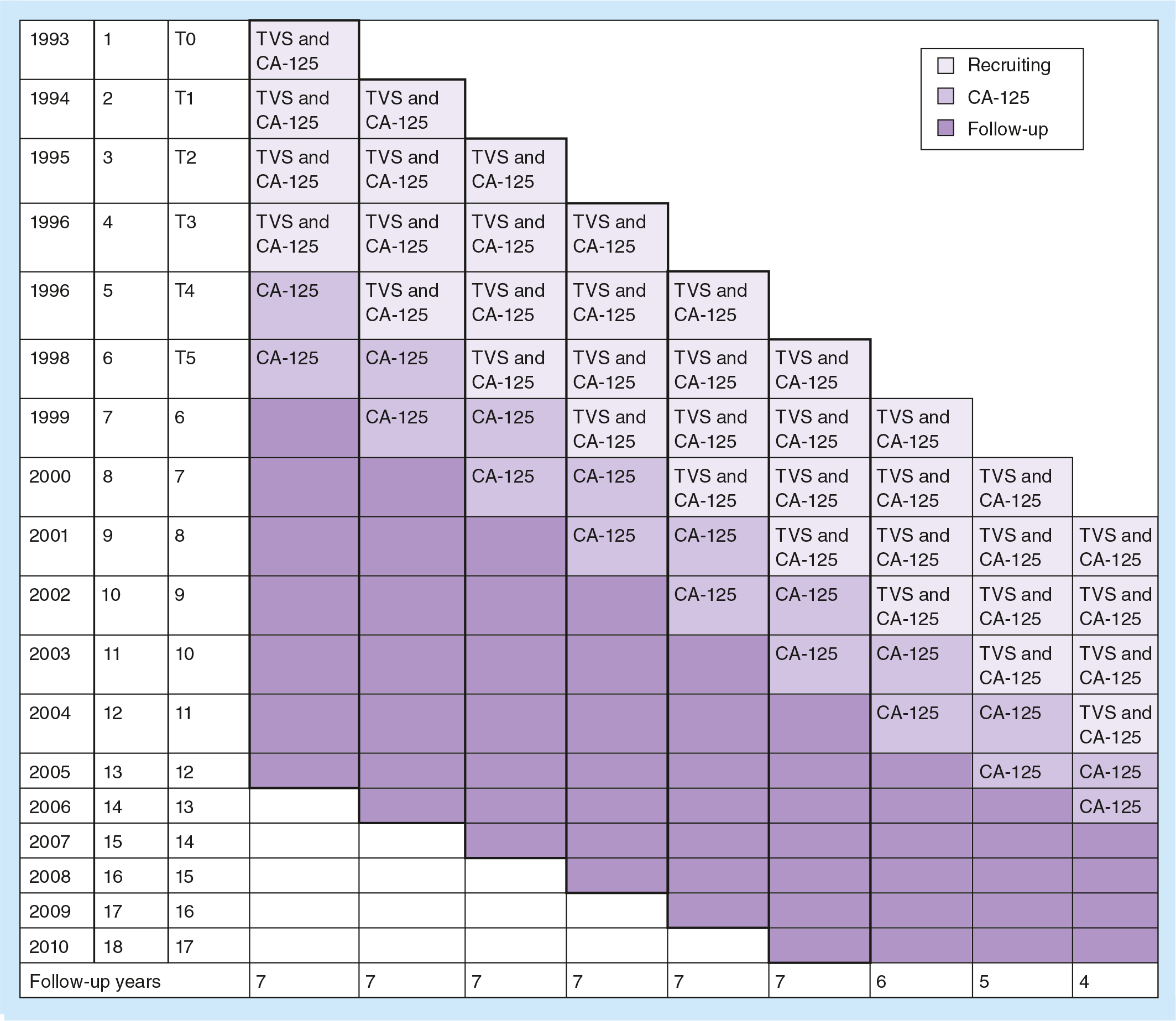
34,253 women were screened with recruiting at different times over an 8-year period to receive four annual screens using a TVS/CA-125 combination and two annual screens using CA-125 alone and received follow-up for a maximum of 13 years.
Not all women in the intervention group received all six rounds of screening.
In the usual care group, bimanual physical examination was stopped in year 6 out of the 14 years that were possible.
Not all screen-detected malignancies were treated.
Women in the screened group that developed ovarian cancer were considered in the survival analysis even if they were never screened or not treated because of how they were randomized.
No difference in mortality was observed between the screened and control groups.
Ovarian cancers that developed as long as 7 years or more after screening were counted as ovarian cancer deaths in the screening group.
The use of two final screens with CA-125 alone as a single trigger showed a much reduced ability to detect ovarian malignancies.
Is the early detection of ovarian tumors using ultrasound effective?
– Three of the four trials reported the detection of early stage disease. Long-term follow-up from the Kentucky trial has demonstrated a survival benefit supporting effectiveness.
Are there differences in ultrasound screening algorithms that affect screening results?
– There were to be shorter delays to surgery in the Kentucky trial than in the PLCO trial so that progression to a later stage disease at diagnosis was less in the Kentucky trial. A single abnormal trigger from screening in the PLCO trial resulted in a lower positive predictive value than in the Kentucky trial that used serial TVS to advance a suspicious case to surgery.
Is the prevalence of ovarian cancer fatal to screening?
– Prevalence is really a cost question. Examination of the cost to screen the population utilized in the Kentucky trial shows that the savings gained by preventing progression of the early stage cases offsets 85–97% of the cost to screen the entire group. This offset is increased by additionally considering the dollar value of life lost so that the savings gained by screening more than pays for the cost of screening.
Does screening for ovarian tumors with ultrasound do more harm than good?
– Psychological conditions that are associated with ovarian screening are governed by underlying factors in different women and not the screening result per se.
Footnotes
Early detection of ovarian tumors using ultrasound
To obtain credit, you should first read the journal article. After reading the article, you should be able to answer the following, related, multiple-choice questions. To complete the questions (with a minimum 70% passing score) and earn continuing medical education (CME) credit, please go to www.medscape.org/journal/wh. Credit cannot be obtained for tests completed on paper, although you may use the worksheet below to keep a record of your answers. You must be a registered user on Medscape.org. If you are not registered on Medscape.org, please click on the New Users: Free Registration link on the left hand side of the website to register. Only one answer is correct for each question. Once you successfully answer all post-test questions you will be able to view and/or print your certificate. For questions regarding the content of this activity, contact the accredited provider,