
Abstract
Epigenetic changes favoring the transcription of the aromatase gene in the endometrium allow endometrial cells to survive in ectopic locations by producing estrogens that spare them from destruction through activated macrophages. Local estrogen production hastens prostaglandin synthesis by stimulating COX-2 activity, thus creating a self-perpetuating sequence of augmented estrogen formation and enhanced inflammation. Repetitive retrograde menstruation reintroduces aromatase-positive endometrial cells endowed with the capacity to implant and invade the peritoneum. In order to control endometriosis, an effective medication must inhibit aromatase, block COX-2, decrease fibrosis and induce amenorrhea. Within this framework, progestins, either alone or in the form of oral contraceptives, appear as first-line treatment for endometriosis owing to their capacity to block enzymes such as aromatase and COX-2.
Role of endometrial inflammation in the development of endometriosis
The relationship between inflammation and activation of the aromatase gene in the eutopic endometrium may represent an important step for the development of endometriosis, a medical condition that may be characterized as an inflammatory pathology capable of producing estrogens locally [1]. These locally produced hormones in both endometriotic lesions and in the eutopic endometrium are thought to play an important role in the modulation of the immunologic mechanisms responsible for controlling the development of endometriosis. Estrogen synthesis is regulated by enzymes, such as aromatase, that are able to convert circulating androgen into estrogen. In the endometrium of disease-free patients, this enzyme is absent because gene transcription is inhibited. However, in patients with endometriosis the aromatase gene promoter is activated in the endometrium by exposure to proinflammatory prostaglandins (PGs), such as E2 (PGE2), thus creating a vicious cycle of inflammation and enhanced local estrogen production, which is necessary for the survival of the endometrial cells in ectopic locations [1–3]. The link between inflammation and aromatase expression in endometriosis is established by NF-κB, a transcription factor responsible for the activation of genes involved in the inflammatory cascade.
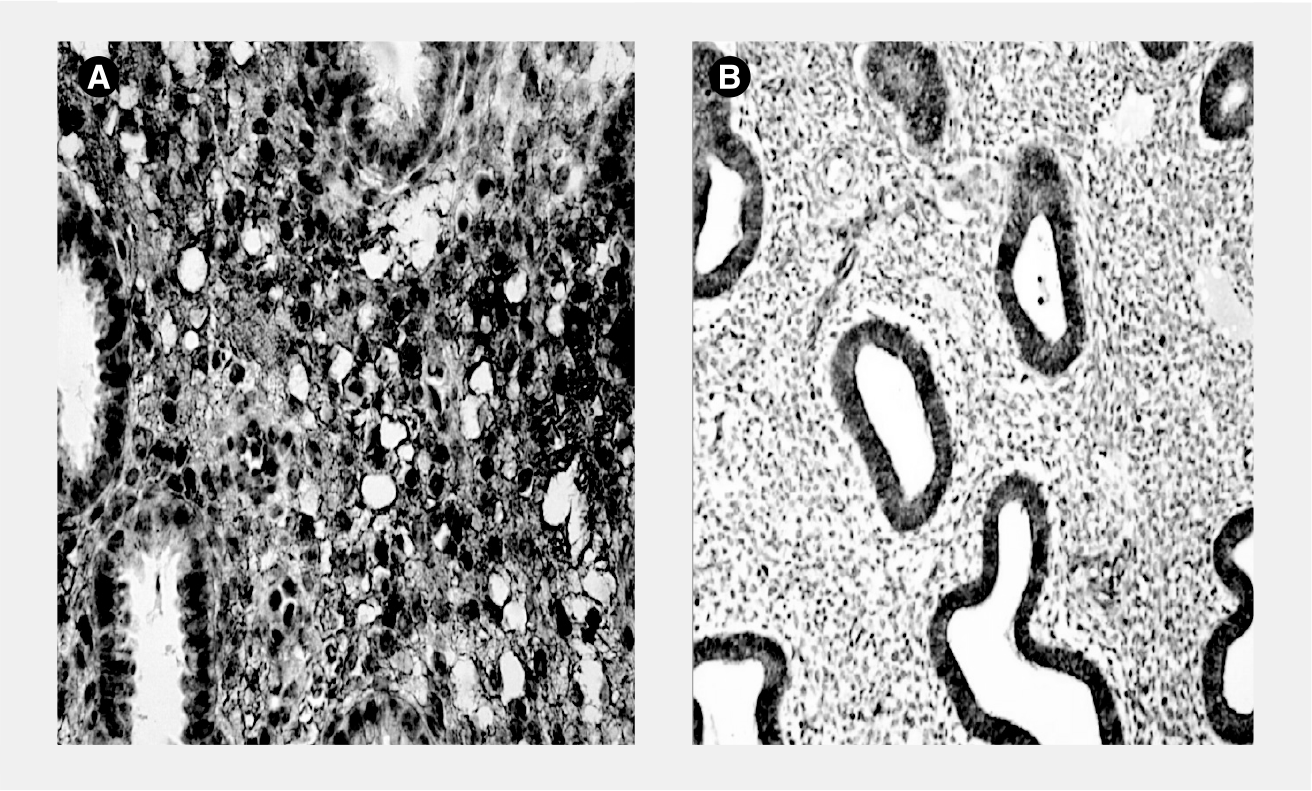
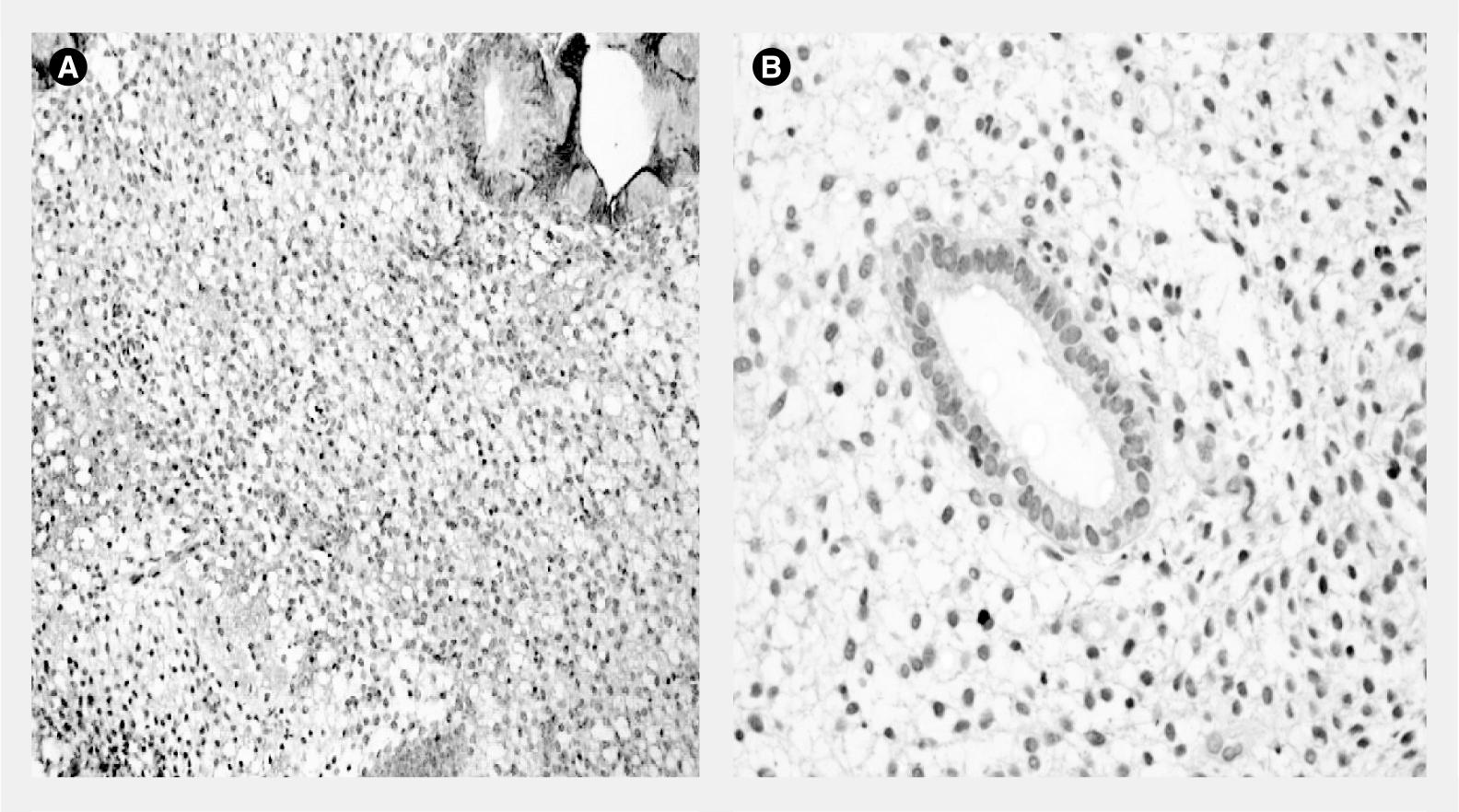
NF-κB activation and its translocation from the cytoplasm to cell nuclei, where it binds to DNA, are the initial steps in a cascade of events that will stimulate inflammation in the tissues [2,4]. In the endometrium, progesterone appears to act by inhibiting this mechanism, since hormone withdrawal, which predates the onset of menstrual bleeding, leads to the inactivation of the NF-κB inhibitory protein in the cytoplasm and the release of active NF-κB, which moves to cell nuclei where it will activate genes related to the inflammatory response, including COX-2 [2,5]. For this reason, the detection of NF-κB by immunohistochemical methods in cell nuclei provides evidence that genes related to inflammation are being activated in that tissue. In the endometrium, the NF-κB subunit bound to cell nuclei is detected more often in patients with uterine pathologies, such as adenomyosis and endometriosis, than in normal controls. This is observed during both the estrogen dominant proliferative phase and in the late luteal phase when progesterone withdrawal occurs in the days preceding the onset of menstrual bleeding [6]. The higher frequency of positive nuclear NF-κB in the endometrium of uteri harboring pathologies suggests a positive association between increased inflammation in the endometrium, the development of clinical conditions, such as endometriosis and the activation of the aromatase gene. In this context, estrogen dominance or progesterone withdrawal plays a pivotal role in the exacerbation of this mechanism [2,6]. The increased inflammation in endometriosis may therefore reflect the increased production of estrogens, which alone increases inflammation and PG production through COX-2 activation and NF-κB activation [1–3,6].
The augmented inflammatory milieu in the endometrium of patients with endometriosis may be pivotal, not only for the development of this pathology, but also for the appearance of other estrogen-dependent diseases [3]. In all these conditions, aromatase expression can be detected in the endometrium of affected patients, while in pathology-free women this enzyme is absent. The monthly exposure of the endometrium to the repetitive occurrence of menstruation with its associated inflammation may trigger transcription of the aromatase gene in susceptible patients through a PG responsive promoter [2,3]. NF-κB is probably one of the major culprits for the development of endometriosis, since it is constitutively activated in this pathology, not only in the lesions but also in the eutopic endometrium and macrophages (

Aromatase expression in the endometrium & the development of endometriosis
The pathogenesis of endometriosis is not yet completely understood since controversies remain with respect to several aspects of this disease, hampering the efficacy of treatment in the long term. Clinically, endometriosis behaves as a chronic, recurrent, debilitating disease and not as a single pathological event in the reproductive life of a woman that can be resolved with a specific short-term medical or surgical treatment. For this reason, it is a medical condition that may be controlled but never completely cured, since new endometrial cells are shed into the pelvic cavity following successive menstrual periods, thus predisposing the patient to recurrence of the disease [3,6].
The high rates of recurrence of endometriosis following successful treatment may be a consequence of stable epigenetic changes present in the eutopic endometrium that are not extinguished during treatment and that may resurface with the resumption of menstruation. The occurrence of retrograde menstruation, which leads to the seeding of endometrial cells in the pelvis, may explain the development of some forms of endometriosis that depend on the implantation of the endometrial cells in the peritoneum [3]. However, one important aspect of this disease is that despite the almost universal occurrence of retrograde menstruation, endometriosis is present in a much smaller proportion of patients. Instead of this being a drawback for the implantation theory originally proposed by Sampson in 1921, this apparent disagreement can be resolved if one assumes that these cells bear important epigenetic changes that are present exclusively in the eutopic endometrium of endometriosis patients, but not in the endometrium of disease-free women [3]. This considerably alters the comprehension of this pathology because endometriosis will then be viewed as an endometrial disease whose clinical course will be dictated by the unique epigenetic changes present in this tissue, thus affecting the transcription of several genes related to inflammation and steroid metabolism and, ultimately, leading to an augmented local inflammatory response and a subsequent boost in estrogen production [3,6]. Once initiated, these epigenetic changes may become stable and long lasting, thus explaining the high rates of disease recurrence upon the resumption of menstrual cycles following the conclusion of hormone therapy. Because of these resilient endometrial changes, the most effective way of controlling endometriosis and its symptoms is to induce long-lasting amenorrhea. The recommencement of menstruation with its retrograde flow will once again transport these modified endometrial cells into the pelvis where they will initiate the development of new foci of the disease in the peritoneum. For this reason, the ultimate medical treatment for endometriosis would have to fulfill the following objectives: reduce inflammation by blocking NF-κB activation, decrease local estrogen production by inhibiting aromatase, diminish fibrosis, inhibit metalloproteinases and, finally, provoke amenorrhea [3]. This amazing drug, which would be very difficult to develop in the laboratory, is commonly found in nature and is called progesterone.
Another clinical situation that results in the remission of endometriosis is menopause, a condition associated with very low circulating estrogen levels. Pharmacologically, this can be accomplished with the use of gonadotropin-releasing hormone (GnRH) analogs, which downregulate gonadotropin secretion from the pituitary gland. However, the ensuing hypoestrogenism causes unacceptable consequences in a woman of reproductive age, precluding the prolonged use that would be required for the treatment of endometriosis [3]. Safer, more patient-friendly but equally effective therapies are clearly needed and this will undoubtedly move in the direction of treatments that will imitate the endometriosis-preventing effects of pregnancy that result from its soaring progesterone levels.
One successful way of mimicking this condition would be to induce a condition of pseudopregnancy by administering progestins, either alone or in the form of oral contraceptives, in continuous regimens [3]. Progestins have the advantage of being relatively cheap and highly effective. In addition, they provoke fewer undesirable side effects and can be used for prolonged periods of time without causing the major adverse events provoked by the protracted use of GnRH analogs. However, before discussing the use of progestins for the treatment of endometriosis, it is important to discuss the function of inflammation and aromatase expression in the eutopic endometrium in the pathogenesis of endometriosis. Progesterone exerts important anti-inflammatory and antiaromatase effects on the endometrium, which are of great relevance for the treatment of endometriosis and the management of its related symptoms [1,3,6].
Role of estrogens in the suppression of cell-mediated immunity & the development of endometriosis
Several studies have revealed that the implantation and development of endometriotic lesions in the pelvis depend on numerous factors that are connected not only to the epigenetic changes in the endometrial cell, but also to a defective immunological system that fails to cope with the destruction of these newly arrived cells transported by retrograde menstrual flow [3,6–10].
The combination of frequent menstruation, an epigenetically modified endometrium and a faulty local immunological response could offer a plausible explanation for the growth of endometriosis in a relatively small percentage of patients, regardless of the almost universal occurrence of retrograde menstruation [3,7,8].
These epigenetic changes in the endometrium may involve, for instance, the commencement of aromatase gene transcription, consequently rendering the endometrium capable of synthesizing estrogens. In sequence, these hormones will upregulate COX-2 expression and the concomitant augmented inflammation may create a susceptible milieu for the development of endometriosis, whose variable clinical course may be ultimately dependent on the strength of aromatase expression and the amount of inflammatory response in both the eutopic endometrium and extrauterine lesions [3].
The initiation and progression of endometriosis may consequently be determined by the intensity of aromatase activity in the endometrium, which may vary with regard to the response to the inflammatory mediators produced during menstruation. The regulation of aromatase expression in the endometrium of endometriosis patients occurs at the level of gene transcription for this enzyme and it is initiated and regulated by promoters that are responsive to PGE2 (
These endometrial changes causing activation of the aromatase gene may even precede the establishment of endometriosis as a clinically diagnosed disease. The consequence of this hyperestrogenic milieu is the enhanced synthesis of proinflammatory PGs, which will not only provoke pain and menstrual bleeding, but will further activate the transcription of the aromatase gene and increase the risk of developing endometriosis [3,10]. This may explain the long period during which symptoms are reported by endometriosis patients prior to the diagnosis of this condition.
Recent studies have shown that the aggressive clinical course of endometriosis may be influenced by the amount of aromatase that is expressed in the endometrium [10,11]. This regulation occurs at the gene transcription level, since the amount of mRNA transcripts for aromatase found in endometrial samples of endometriosis patients shows a positive correlation with the severity of the disease [11]. Likewise, the immunohistochemical detection of this enzyme is also more common in the endometrium of patients with more advanced stages of the disease (American Society of Reproductive Medicine stage IV) compared with those at earlier stages (stage I) [10]. The positive correlation between mRNA levels in the eutopic endometrium and the severity of endometriosis and adenomyosis is also in agreement with this hypothesis [11]. Whether or not endometriosis begins as an endometrial disease before establishing itself elsewhere in the pelvis cannot yet be proven conclusively, although previous studies demonstrating that the onset of symptoms associated with this pathology may commence many years prior to its diagnosis may support this hypothesis [3,6,10,12].
The clinical observation that endometriosis behaves as a chronic, recurrent disease has important therapeutic implications, since the treatments currently available are unable to effectively cure this disease in the long term. Most of the meta-analyses carried out so far have indicated high recurrence rates following either surgical treatment or the discontinuation of medical therapy [3,10–14]. The resumption of menstruation with its retrograde flow appears to represent a risk factor for the recurrence of the disease. Nevertheless, rather than any lack of efficacy on the part of the various surgical and medical approaches for the treatment of this disease, these high recurrence rates may reflect more subtle differences between the endometrium of patients with endometriosis and disease-free women, predisposing the former to recurrence of the disease with the resumption of menstruation [3,10]. Aromatase expression in the eutopic endometrium is probably an important risk factor for the development of endometriosis, since the clinical behavior of endometriotic foci may ultimately depend on the amount of aromatase expression that is present in the lesions and also in the eutopic endometrium [1,3,10,11,13]. This hypothesis is in agreement with observations that aromatase expression is not detected in the endometrium of disease-free women, whereas it is present in the endometrium of patients with other pathologies, such as adenomyosis, endometrial polyps and myomas, which are commonly associated with endometriosis [3,13].
In these pathological conditions, aromatase expression in the eutopic endometrium is enhanced by PGs, particularly PGE2, and possibly other inflammatory mediators [15]. However, PGE2 only augments aromatase in the endometrium in which basal levels of this enzyme are detected, having no effect on the aromatase-negative endometrium of disease-free women. This may suggest that the initial epigenetic changes that render the promoter of the aromatase gene in the endometrium responsive to proinflammatory mediators represent an early event in the pathogenesis of endometriosis and in the manifestation of its associated symptoms [1,3,10,15,16]. Retrograde menstruation carries endometrial cells to the pelvis, which will then trigger an intense inflammatory reaction, attracting an efflux of immunologically active cells including macrophages and natural killer cells. This intense inflammatory reaction will generate great amounts of PGs and other inflammatory mediators, which will stimulate aromatase expression exponentially in endometrial cells that already express basal levels of this enzyme, but not in the aromatase-negative cells [1,3,15,16], thus expanding local estrogen production, which will further enhance PG synthesis by activating COX-2. This will result in a vicious cycle of augmented inflammation and enhanced aromatase expression, and the subsequent local estrogen production will not only facilitate the implantation of these endometrial cells in the peritoneum, but also prevent their destruction by the immune system [10,15,16].
In patients with an established diagnosis of endometriosis, endometrial positivity for aromatase at the protein level or the amount of mRNA transcripts for this enzyme tend to increase with the severity of the disease [10,11]. One possible explanation for these findings would be a higher likelihood of spontaneous regression of endometriosis in the earlier stages of the disease, possibly as a consequence of a reduction in aromatase activity in the eutopic endometrium caused by a decrease in systemic inflammation, which renders the aromatase gene promoter less operational [10]. This may explain why positive lifestyle changes known to curb inflammation are associated with a reduction in the symptoms of endometriosis.
Although aromatase expression in the eutopic endometrium may be pivotal for the onset and progression of endometriosis, how this enzyme affects the development of this condition remains to be clarified. The role played by estrogens in inhibiting immune surveillance by activated macrophages has been suggested as one of the likely mechanisms by which the presence of aromatase in the endometrium affects the clinical course of endometriosis [3]. Therefore, the decreased cytotoxicity of the innate immune system in endometriosis may be a consequence of the disruption of the mechanisms of phagocytosis by estrogens [17–19]. Local estrogen production, rather than an innate defective immune system, would explain the occurrence of diminished immunological surveillance in patients with endometriosis [3,10]. Although this may appear a rather simplistic explanation for a complex multifaceted disease, this hypothesis may explain why, instead of destroying the endometrial cells that have recently reached the pelvis and halting the progression of the disease, the macrophages are subverted to collaborate with its progression by releasing a variety of inflammatory and angiogenic factors. The presence of estrogen receptors in the macrophages make them responsive to these locally produced hormones by curtailing their scavenger function (

Inhibition of phagocytosis by local estrogen production is consequently the conceivable mechanism through which endometrial cells in the peritoneal cavity are spared from destruction, thus implanting and developing into endometriotic lesions, while the aromatase-negative cells are eradicated from the pelvic cavity in the days following menstruation [3,10,15,18,20,21].
The presence of an epigenetically modified endometrium in endometriosis capable of producing estrogens locally is a plausible explanation, not only for the recurrence of the disease with the resumption of menstrual cycles after successful medical or surgical treatment, but also to explain the paradox that endometriosis develops in only a small percentage of women despite the almost universal occurrence of retrograde menstruation. The role of menstruation with its retrograde flow is therefore pivotal for the establishment of the disease, which explains why amenorrhea is the only effective way of controlling it. The need for constant seeding with recently arrived endometrial cells for the de novo appearance of endometriotic lesions in the pelvis following surgical treatment is corroborated by clinical observations showing that the recurrence rates of this malady decrease significantly if an endometrial resection is carried out concomitantly with the surgical procedure [22]. The presence of an intact endometrium rather than merely an incomplete surgery appeared to be the principal risk factor for the recurrence of endometriosis in this study. However, the intrinsic capacity of the endometrium to regenerate may limit the long-term success of this procedure.
The endometrial hypothesis may also successfully explain other forms of this malady such as deep-infiltrating endometriosis. The similarity of the lesions and the common association between adenomyosis and deep-infiltrating endometriosis suggest that the same epigenetic changes occurring in the eutopic endometrium during repetitive menstrual cycles and leading to the invagination of the basal layer into the myometrium may also occur in the Müllerian remnants deeply embedded in the rectovaginal septum. Likewise, if the endometrial cells acquire an aggressive phenotype rendering them capable of infiltrating the underlying myometrium and causing adenomyosis, it is also expected that when they arrive in the pelvis they will display the same aggressive behavior in the peritoneum, invading deeper into this tissue rather than just forming superficial implants. This hypothesis differs from the model proposed by Nisolle and Donnez, in which they suggests that there are different types of endometriosis [23]. However, the various forms of this disease may merely represent different facets of the same endometrial disease caused by the intrinsic capacity of this tissue to generate more or less estrogen in response to inflammation. In sequence, this will affect the immune surveillance mechanisms and the individual capacity to respond to inflammation by increasing fibrosis.
Aromatase inhibition with progestins & the treatment of endometriosis
The hypothesis that endometriosis is a chronic condition that depends on, for its progression, the amount of aromatase expression in the eutopic endometrium predicts that the clinical course of this disease may depend on the amount of inflammation present in the eutopic endometrium during the menstrual cycle, since the promoter gene for this enzyme responds to PGs [15]. If this hypothesis is correct, it may also explain the high failure rates of all forms of surgical or medical treatments for endometriosis over the long term, as, once incorporated into the eutopic endometrium, these epigenetic changes may be long lasting and stable and may be reactivated upon the return of menstruation and its associated inflammation [3]. Likewise, lifestyle or dietary changes capable of curbing inflammation will contribute towards the remission of this disease.
Since aromatase expression in the eutopic endometrium appears to be crucial not only for the development of endometriosis, but also in determining the aggressiveness of its clinical course, drugs that suppress aromatase expression or modulate immunological activity will play an important role in endometriosis therapy [1,3,10]. Recent reports have shown that the efficacy of aromatase inhibitors in the treatment of unusually aggressive forms of endometriosis is associated with high levels of aromatase expression [24–27].
A clinical, observational study published recently by the present authors' group showed that aromatase expression in the eutopic endometrium of patients with endometriosis showed a positive correlation with the clinical stages of endometriosis as rated according to the American Society of Reproductive Medicine classification [10]. Similar results were observed using mRNA transcripts for aromatase in the eutopic endometrium of patients with severe forms of endometriosis and adenomyosis [11]. In the endometriotic lesions, the severity of the disease also showed a positive correlation with aromatase level and COX-2 expression [13]. These results, although not establishing a causal relationship between aromatase expression in the eutopic endometrium and the progression of endometriosis, suggest a strong association between the amount of expression of this enzyme, the stage of the disease, the intensity of the inflammatory response and the magnitude of pain symptoms. Regression of endometriosis, on the other hand, may be associated with the disappearance of aromatase expression in the eutopic endometrium [24]. The clinical course of this disease may, therefore, be commanded by the presence of aromatase in the endometrium. On the other hand, pharmaceutical treatments that inhibit aromatase activity in the eutopic endometrium or in the endometriotic lesions will halt estrogen production and reduce the ensuing inflammation and fibrosis [25]. This will have a positive effect on the clinical course of the disease, keeping it under control as long as amenorrhea is maintained [3]. Ideally, an effective treatment for endometriosis will have to disrupt all the different molecular pathways that are responsible for the progression of this disease. This hypothetical medication should block NF-κB activation, suppress COX-2 activity, inhibit aromatase expression and induce amenorrhea [3,24]. The medication should also be safe, reasonably cheap and devoid of major side effects that would preclude its prolonged use. This therapeutic goal can be achieved with the use of progestins as in the pseudopregnancy regimens with continuous oral contraceptives (
Due to their strong progestational effect on the endometrium and their suppressive effect on ovarian steroidogenesis, oral contraceptives may interrupt this vicious cycle of augmented COX-2 and aromatase expression at the endometrial level, consequently decreasing both estrogen synthesis and inflammation [3,24]. The mechanism of the suppressive effect of oral contraceptives on aromatase expression in the endometrium is direct and occurs at the gene transcriptional level, as suggested by the present authors' group in a 2006 publication and later confirmed by molecular biology studies [24,25].
The absence of aromatase expression in the endometrium exposed to progestins is therefore the result of the decreased formation of this enzyme rather than a competitive blockade of enzymatic activity [24,25]. A decrease in inflammation is also observed with the use of oral contraceptives. In patients with uterine pathologies and symptoms of menorrhagia and dysmenorrhea, the continuous use of oral contraceptives containing gestodene significantly decreased the frequency of positive nuclear NF-κB in the endometrium [26]. This effect was observed only in patients in whom amenorrhea was achieved, since the presence of breakthrough bleeding is associated with the exacerbation of inflammation. These results suggest that the anti-inflammatory effects of gestodene on the endometrium are mediated through suppression of NF-κB activation, thus leading to the inhibition of COX-2 and aromatase, and the resolution of pain and bleeding associated with endometriosis [27].
A similar effect was also recently observed in explants of endometrial cells with the use of dienogest, a progestin newly introduced into the market for the treatment of endometriosis [28]. As with gestodene and other progestins investigated so far, dienogest was also effective in reducing both aromatase and COX-2 expression in endometrial cells. This effect appears to be a class action of all progestins, acting by binding to and activating progesterone receptors, which will elicit a strong anti-inflammatory response leading to NF-κB inactivation and the suppression of both COX-2 and aromatase in the endometrium [29]. This effect appears to be necessary to resolve endometriosis-related symptoms and halt the progression of the disease.
Danazol, a testosterone derivative also commonly used for the treatment of endometriosis, also inhibits aromatase expression in the eutopic endometrium of patients with adenomyosis by acting directly on gene transcription and reducing the levels of mRNA [30]. The present authors' findings that oral contraceptives containing gestodene are able to reduce aromatase expression in the eutopic endometrium of patients with adenomyosis, endometriosis and myomas may explain their effectiveness when used to prevent, not only recurrences in surgically treated patients with endometriosis, but also the bleeding and pain associated with these pathologies [3]. In patients with adenomyosis, the use of a levonorgestrel-releasing intrauterine device was also effective in inhibiting aromatase expression in the endometrium, which explains the usefulness of this device for the treatment of both the menorrhagia caused by adenomyosis and the endometriosis-related pain [31].
The present authors' group recently investigated why some patients failed to respond to continuous oral contraceptives in terms of pain control. In patients with endometriosis using a continuous contraceptive regimen of 30 μg of ethinylestradiol and 3 mg of drospirenone, the presence of pain and breakthrough bleeding was associated with the persistence of aromatase expression in the eutopic endometrium, while in those patients who achieved amenorrhea and became pain free, the enzyme could no longer be detected in the endometrium. These results are summarized in
Percentage of aromatase-positive endometria in patients with endometriosis using oral contraceptives, according to whether or not they complained of pelvic pain.
p < 0.001.
OC: Oral contraceptive.
Recent clinical observations showing that the association of a progestin with an aromatase inhibitor was effective in reducing pain in endometriosis patients who had failed to respond to conventional medical treatment is in accordance with the present authors' findings that these patients did not respond fully to treatment because aromatase expression remained active [32]. In this group of patients who reported breakthrough bleeding and pain while using continuous oral contraceptives, the use of naturally occurring aromatase inhibitors was also effective in reducing pain and bleeding.
One effective aromatase inhibitor was resveratrol, a grape-derived polyphenol that inhibits both aromatase and COX-2 expression [33]. In endometriosis patients who remained symptomatic while using a combined pill containing drospirenone and ethinylestradiol, the concomitant use of resveratrol at a daily dose of 30–50 mg resulted in a significant reduction in the number of patients reporting the occurrence of breakthrough bleeding and pain. These results are summarized in
Effect of resveratrol on the percentage of dysmenorrhea in patients with endometriosis/adenomyosis using drospirenone/ethinylestradiol in a continuous regimen.
χ2 test: p < 0.05 for DRSP/EE + resveratrol × resveratrol; p < 0.0001 for DRSP/EE + resveratrol × DRSP/EE.
DSRP: Drospirenone; EE: Ethinylestradiol.
In patients using contraceptive pills containing gestodene for the treatment of endometriosis, the combined use of ω-3 fish oil at a daily dose of 3 mg was more effective in decreasing pain and breakthrough bleeding compared with the use of oral contraceptives alone. ω-3 is a natural COX-2 inhibitor that, in addition to decreasing inflammation, also offers other health benefits to the cardiovascular system. Contrary to the prolonged use of COX-2 inhibitors, ω-3 is devoid of adverse effects on the gastrointestinal and cardiovascular system, and its prolonged use may substantially increase the therapeutic efficacy of continuous regimens of oral contraceptives in the treatment of endometriosis (

The blockade of COX-2 expression plays a pivotal role in the management of endometriosis-related dysmenorrhea, since the amount of PGs produced in the endometrium correlates positively with the intensity of pain [34,35]. Because of their progesterone-like effect on the endometrium, oral contraceptives not only suppress aromatase but also COX-2 expression in this tissue [35,36]. This will certainly suffice to ensure that they become the first line of treatment for endometriosis. Nevertheless, the use of combined multitherapy with resveratrol or ω-3 for the treatment of endometriosis rather than the conventional monotherapy may represent a more rational approach for the treatment of this multifaceted disease, whose chronic nature renders prolonged treatment regimens mandatory. Oral contraceptives, particularly in continuous regimens, effectively block aromatase and COX-2 expression in the endometrium [36]. The blockade of this local estrogen production will treat not only the menstrual-related symptoms but will also prevent the future development of estrogen-dependent pathologies [37,38].
Controversies still exist in the literature with respect to the role of aromatase in endometriosis. One interesting paper published by Colette et al. failed to reproduce the findings of other earlier studies showing that aromatase expression could be detected in both the lesions and in the eutopic endometrium of endometriosis patients [39]. However, when analyzing the results, the authors failed to take into consideration that a great number of patients in this study were undergoing treatment with either progestins or GnRH analogs, which are known to suppress aromatase expression at the gene transcription level. Furthermore this paper also failed to mention how many of their patients who were going through menstrual cycling had used hormonal therapy for endometriosis in the recent past. Because this information is lacking, their conclusions have to be taken with caution, since it is likely that many of their negative results were caused by current or previous hormonal treatment.
In the future, combining oral contraceptives with naturally occurring anti-inflammatory and antiaromatase agents may increase the efficacy of treatment without the adverse effects that are found with letrozole and NSAIDs [35]. However, further studies need to be conducted in order to improve the efficacy of these new therapeutic combinations.
Conclusion
In conclusion, oral contraceptives, particularly when used in continuous regimens, are considered as the first-line treatment for endometriosis because of their efficacy and safety, and the long-lasting amenorrhea that can be induced with their use. Progestins are able to suppress aromatase, COX-2 and NF-κB activation in the eutopic endometrium and in endometriotic cells, thus fulfilling the necessary criteria for an effective treatment for endometriosis. Contrary to the classical aromatase inhibitors, such as letrozole, which act by suppressing enzymatic activity, progestins act at the gene transcription level by silencing the gene that codes aromatase. If the endometrium is exposed to progestin, the aromatase enzyme that would excite estrogen production in this tissue is not formed, thus permitting the immune surveillance mechanisms to become operative again. In this respect, the role of estrogens in promoting the development of endometriosis can be summarized as proinflammatory, while also blocking phagocytosis by activated macrophages (

The importance of aromatase expression in the eutopic endometrium for the development of endometriosis.
While most patients respond favorably to medical therapy with progestins and oral contraceptives, in some cases pain cannot be effectively suppressed and these patients remain symptomatic. In this case, preliminary studies have shown that the association of the use of resveratrol or ω-3 with oral contraceptives will increase the efficacy of treatment. The reason for this progesterone resistance is not completely understood but may involve the persistence of aromatase expression in the eutopic endometrium.
Future perspective
Endometriosis is an inflammatory pathology that develops as a consequence of enzymatic changes in the eutopic endometrium that enable this tissue to survive in ectopic locations by producing estradiol. The local estradiol production plays a pivotal role in the development of endometriosis, since it blocks endometrial cell phagocytosis by activated macrophages. Progestins and oral contraceptives are capable of inhibiting both aromatase and Cox-2 expression, making them the ideal treatment for endometriosis. Combined therapies with natural aromatase inhibitors or antiinflammatory agents may further increase the efficacy of hormonal treatment, rendering them excellent candidates for the future treatment of endometriosis.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Executive summary
Inflammation in the eutopic endometrium of endometriosis patients is triggered by NF-κB. This transcription factor is more active in the endometrium of patients with endometriosis and other estrogen-dependent pathologies.
Aromatase expression is activated in the endometrium by inflammatory mediators such as prostaglandin E2.
Aromatase expression in the endometrial cells spares them from destruction by activated macrophages when they are transported through retrograde menstruation into the pelvis.
Synthetic progestins and natural progesterone are inhibitors of aromatase expression in the endometrium, acting by silencing the gene that codes for this enzyme. A combination of oral contraceptives in continuous regimens with natural aromatase inhibitors, such as resveratrol, increases their efficacy in the management of endometriosis-related pain.
Aromatase expression in the eutopic endometrium plays a pivotal role in the development of endometriosis by blocking cell-mediated immunity. Progestins inhibit aromatase expression in endometriosis and in the eutopic endometrium at the gene transcription level.