
Abstract
Ethnic differences in breast cancer survival have been a long-standing concern. The objective of this article is to present relevant studies for all major US racial/ethnic groups including African–Americans, Latinos, Native Americans, Japanese–Americans and Native Hawaiians, and to discuss underlying causes of disparity, In comparison to Caucasian women, African–American women continue to experience the poorest breast cancer–specific survival of all ethnic groups in the USA. The prognosis for Latinos, Native Hawaiians and Native Americans is intermediate, better than for African–Americans but not as good as for Caucasians, whereas Japanese–American women tend to have better outcomes. The following possible contributors to the observed differences are discussed in detail: unfavorable distribution of stage at diagnosis due to low screening rates, limited access to care and treatment, tumor type, comorbidities, socioeconomic status, obesity and physical activity.
According to the 2010 Surveillance, Epidemiology and End Results (SEER) report [1], the 5-year breast cancer-specific survival rate in the USA was 89.2%. The strongest determinant of survival is stage at diagnosis: 98.6% for localized disease, 83.4% for regional disease and 23.4% for metastasized breast cancer [1]. During the last 20 years, improvements in breast cancer survival have been observed in all ethnic groups [2,3], but substantial differences across ethnic groups have been reported repeatedly with worse outcomes among ethnic groups of low socioeconomic status (SES) [4–8]. Several of the predictors proposed as possible explanations for the ethnic-specific survival differences, for example, early detection, access to care, pre-existing chronic diseases, obesity, poverty and lifestyle factors, are related to SES [9–11]. This raises the question whether ethnic disparities may be due to SES rather than biologic differences, such as tumor types or genetic susceptibility [12–15]. The objectives of this article are to compare breast cancer survival rates for all major racial/ethnic groups in the USA (African–American, Hispanic/Latino, Asian–American, Native Hawaiian/Pacific Islander and Native American) to rates for Caucasian women and to examine underlying causes. Based on our own expertise, there is a special emphasis on Japanese–American and Native Hawaiian women. Genetic aspects of susceptibility are not presented as part of this article.
Methods
Relevant publications were identified in PubMed® and in the reference sections of published reports. From the large number of investigations that focused on African–American women, we selected the most recent ones and included a large meta-analysis to cover the earlier time period. For the other ethnic groups, we present all available studies even if they were small and published during earlier years. Due to the differences in methodology across studies and the large body of literature, we did not attempt our own meta-analysis or systematic review. Instead, we selected studies that compare breast cancer-specific and all-cause survival across ethnic groups and illustrate particular causes of disparity. The 24 reports summarized in
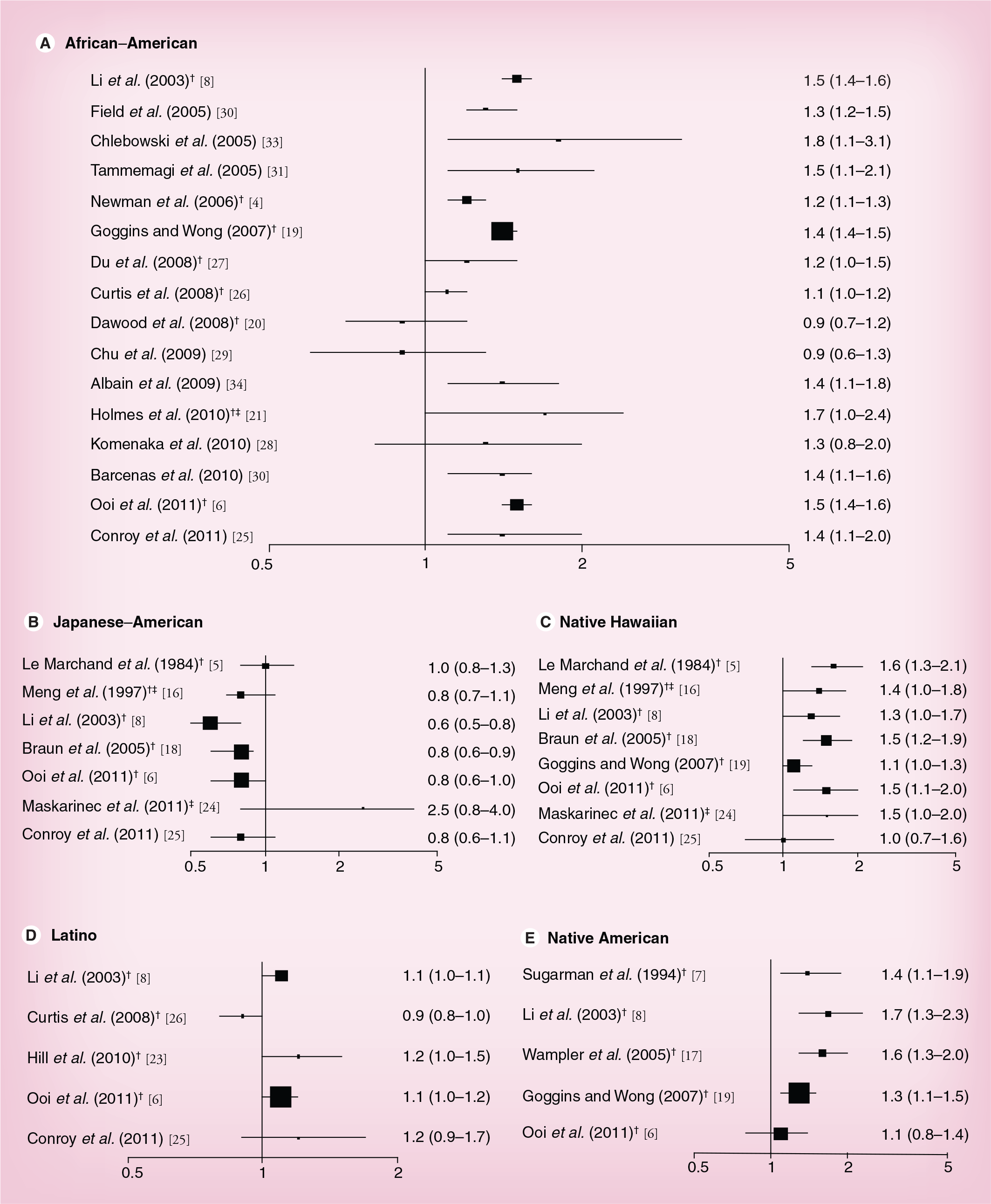
Selected studies comparing breast cancer-specific survival by ethnic group.

Ethnic groups: A: Asian–American; AN: Alaska Native; B: African–American; C: Chinese–American; F: Filipino; H: Native Hawaiian; J: Japanese–American; L: Latino; NA: Native American; PI: Pacific Islander; S: Samoan; W: Caucasian.
Stages: 0: In situ; I: Stage I; Loc: Localized.
CCR: California Cancer Registry; CRN: Cancer Research Network; ER: Estrogen receptor; HR: Hazard ratio; HTR: Hawaii Tumor Registry (part of SEER); IHS: Indian Health Service; MEC: Multiethnic Cohort study; N/A: Not available; PR: Progesterone receptor; SEER: Surveillance, Epidemiology and End Results; SES: Socioeconomic status; SWOG: Southwest Oncology Group; WHI: Women's Health Initiative.
Breast cancer-specific survival by ethnic group.
Results
African–Americans
The literature on ethnic-specific survival differences is most abundant for African–Americans. The higher breast cancer mortality rates have been a concern for many years, in particular in light of the incidence rates below those for Caucasians [1,3]. Despite some exceptions, the majority of publications show an elevated risk of dying for African–Americans compared with Caucasian breast cancer cases with HRs ranging between 1.2 and 2.6 (
Asian–Americans
Due to the large differences in SES across Asian–American subgroups, mortality differs considerably by subgroup and also by immigrant status. For example, in a California study, foreign born Chinese and Filipino women had poorer outcomes than those born in the USA [22]. For women of Japanese and Chinese ancestry, generally more favorable outcomes have been reported than for Caucasians, whereas Filipino, Korean, south Asian and Vietnamese immigrants tend to experience poorer outcomes [8,16,22]. When risk estimates for Asian–Americans as a group were presented, outcomes were better than for Caucasians [21,26]. Given the limited data on most Asian–American subgroups, we only summarize studies with Japanese–Americans in
Native Hawaiians/Pacific Islanders
Similar to African–Americans, health disparities in Native Hawaiians and other Pacific Islanders due to low SES and lack of access to care have been an area of great concern and active research [35]. Because only one report presented separate results for Samoans [19], all investigations shown in
Latinos
Of the five studies that included Latinos (
Native Americans
We identified five studies (
Discussion
While there is little doubt that mortality from breast cancer has decreased for all ethnic groups during the last 20 years [1,2], it is clear that survival differences between ethnic groups have not been eradicated. Based on many reports confirming disproportionate numbers of late stage disease, lack of screening and early detection due to limited access to healthcare remain important contributors to this situation [9,23]. Nevertheless, the role of lifestyle factors, such as obesity and physical activity, has become better understood and gained more attention [39]. The differences and time trends across populations are not easily disentangled since the studies do not control for a common set of covariates known to influence survival. As described in an excellent review, many of these factors are related to SES and affect prognosis in combination and through multiple pathways [10]. For example, poverty may directly be responsible for lack of screening but also indirectly affect tumor biology because obesity, smoking and poor nutrition may promote the development of tumors with adverse characteristics. We will consider the major factors that have been identified as contributors to the observed differences and explain the inconsistencies in the reports discussed above.
Early detection & access to care
Given the importance of stage at diagnosis for prognosis [1], screening participation and early detection are the most important predictors of survival. There are many examples of this in the literature, such as the analysis of 229,594 cases from the SEER registries that shows respective rates of 50 and 57% stage I cases among Caucasians and Japanese–Americans, compared with 35, 38,42 and 45% in African–Americans, Latinos, Pacific Islanders and Native Americans, respectively [6]. In a study among Latinos, the screen-detected proportion of cancers was only 52% compared with 61% in Caucasians, and adjustment for type of detection reduced the ethnic difference [23]. As described in a large trend analysis for 1987–2005 [2], absolute ethnic disparities declined for mammography screening, stage at diagnosis and 5-year cause-specific probability of death during this time period; however, relative ethnic disparities in 5-year cause-specific probability of death persisted.
Lack of early detection is further complicated by delay in treatment initiation [9]. Another important issue is compliance with consensus recommendations to treat breast cancer, which have been associated with improved survival [40]. Many reports suggest less surgery, radiation therapy and hormone treatment and 20–50% rates of inappropriate treatment among African-Americans as compared with Caucasians [8,32]. When detailed information from medical charts was used to assess breast cancer treatment [41] or comorbidity and treatment patterns from insurance claims were included as covariates [36], survival times were relatively similar across ethnic groups in Hawaii with a rather unique healthcare environment. Because cancer registries do not typically collect information on treatment beyond 6 months, many of the published reports are missing detailed treatment information after initial treatment. However, access to care and health insurance rates [42] are probably not the only reason for these delays; geographic distance from good treatment centers and cultural factors probably also contribute as suggested by the disparate outcome in the SWOG trials [34].
Tumor type
Advances in molecular classification and characterization of breast tumors into distinct subtypes by using DNA micro arrays independent of disease stage has allowed stratification of cases by prognosis [43,44]. Whereas the respective proportions for the major subtypes appear to be similar in Japanese–Americans and Chinese–Americans as in Caucasians [45], the distribution in African–Americans is skewed toward the subtypes with poorer outcomes [46,47]. African–American women are more likely to be diagnosed with higher tumor grades as well as ER/PR-negative and triple-negative tumors than Caucasians, partly as a result of later stage at diagnosis [9,11,33,48]. The same observation was made for Latino women, although to a lesser degree [6]. Interestingly, a study among a socio-economically deprived population with high obesity rates showed more tumors with poor prognostic features (i.e., late stage, triple negative and lymph node metastases [49]). This suggests that a low SES regardless of ethnic background is associated with breast cancer tumors that have an unfavorable prognosis [10].
Comorbidity
Closely related to the question of appropriate treatment is the issue of pre-existing conditions. Given the high rates of obesity, diabetes and hypertension among African–American and Latino [42] as well as Pacific Islander women [37,38], the presence of these conditions may be responsible for worse breast cancer outcomes, possibly due to less tolerance to cancer treatments. Women with comorbidities may receive less aggressive treatment, as described for diabetic women, due to disease-related complications [50]. The association of comorbidity with lower survival rates among breast cancer patients has been shown repeatedly [36,51,52]; however, comorbidity contributes more to higher overall mortality in breast cancer patients than to breast cancer-specific mortality [31]. On the other hand, controlling for comorbidity does not eliminate all ethnic differences as can be seen in several studies within the meta-analysis [4].
Socioeconomic status
As for many conditions, outcomes tend to be worse for individuals with lower education and income than for those with higher SES [53]. In a recent report on health disparities [42], the persisting ethnic differences in education, health insurance coverage and poverty status are well documented. Although many survival analyses included SES indicators, the registry-based studies usually only had neighborhood-level SES indicators with well documented limitations available since more accurate individual-level SES data are difficult to collect [54]. Nevertheless, in the meta-analysis of studies among African–American women, the area-wide measure of SES narrowed the survival difference considerably [4]. Interestingly, it appears from a limited number of studies within Caucasian populations with low SES that poverty is associated with similar cancer disparities as observed across ethnic groups [2,10,49]. Adjustment for SES probably remains insufficient because a person's economic and social situation is more complex than just assessing income and education; housing, environmental, dietary, cultural, behavioral and access to healthcare issues are additional contributors to health effects and are not easily captured by traditional demographic data [4,53,55]. Since SES is not a biologic risk factor itself and rather a marker for other factors, such as access to screening and healthcare, it is also challenging to interpret studies that controlled for SES and true mediating variables, such as obesity, at the same rime.
Obesity & physical activity
The role of obesity at diagnosis and later has become much clearer over recent years and is important in light of the higher obesity rates in non-Caucasian women [37,42]. There is increasing evidence that obese women with breast cancer experience worse breast cancer survival, as much as 30% higher mortality, than survivors with normal weight [39,56]. This difference appears to be due to estradiol formation in adipose tissue, which stimulates neoplastic cell proliferation in obese women [57], contributing to more biologically aggressive tumors [58]. Estrogen-independent pathways, in particular adipokine production (e.g., adiponectin and leptin), may also contribute to an aggressive breast cancer phenotype [59,60]. Furthermore, obese women may be given lower doses of chemotherapy because the ideal body surface area rather than true body surface area is used to estimate the dose of chemotherapy [61]. Epidemiologic data for other modifiable factors such as physical activity and healthful diets are not as convincing [39], but a growing number of large observational studies have demonstrated that participation in moderate intensity recreational physical activity after diagnosis may improve survival in women with breast cancer [62,63].
Methodological issues
In the studies included in this review (
Conclusion
From the existing evidence, it appears that African–American women continue to experience the poorest breast cancer-specific survival of all ethnic groups in the USA. The prognosis for Latinos, Native Hawaiians and Native Americans is intermediate, better than for African–Americans but not as good as for Caucasians and Japanese–Americans. One possible explanation of this evidence is that genetic susceptibility or lifestyle factors predispose some ethnic groups to tumors with more adverse behavior [12–15]. Future genetic investigations may also detect ethnic-related genetic polymorphisms of chemotherapy metabolizing enzymes [64]. However, an alternative interpretation is that, regardless of ethnic background, women with low SES and unhealthy lifestyles are more likely to experience late stage disease and to develop more aggressive tumors than more affluent women. This hypothesis is supported by the following pieces of evidence. One, research among Caucasian women with low SES indicates similar tumor types and poor survival as observed in African–American populations [49]. Second, improvements in outcomes have occurred over time across ethnic groups [2]. Finally, inclusion of more treatment, comorbidity, SES and lifestyle information in the statistical analysis appears to diminish the observed ethnic differences (
Future perspective
For the future, Newman et al. proposed two research areas that need to be strengthened in addition to improved early detection and access to care: methods to measure effects of sociobehavioral issues and poverty (e.g., environmental, economic, cultural and lifestyle factors) on breast cancer risk, and an exploration of associations between ethnicity and variation in primary breast tumor biology [4]. As to efforts in reducing the unequal mortality to breast cancer, improvements in SES, health insurance and access to care will still achieve great improvements, although we do not know at this time whether a part of the observed ethnic differences is due to genetic factors that cannot be modified.
Executive summary
Although breast cancer survival has improved for all ethnic groups over the last 20 years, poor survival rates in some ethnic groups remain an important concern.
In comparison to other ethnic groups in the USA, African–Americans have worse breast cancer-specific survival rates.
Breast cancer-related mortality among Latino, Native Hawaiian and Native American women is intermediate between African–Americans and Caucasians, whereas Japanese–Americans and some other Asian–American groups show better survival rates than Caucasians.
Adjustment for prognostic predictors reduces ethnic differences in breast cancer survival.
Lack of early detection, late stage at diagnosis and limited access to healthcare are the most important predictors of poor breast cancer survival.
Low socioeconomic status appears to be associated with tumors showing unfavorable characteristics and higher breast cancer-related mortality independent of ethnic background.
Comorbidities, obesity and lifestyle factors have emerged as additional significant determinants of prognosis.
Improvements in early detection of breast cancer and access to healthcare will lead to further reductions in breast cancer-related mortality.
Better methods of measuring the effects of sociobehavioral factors and poverty on tumor biology are needed to understand these associations.
Explorations of tumor biology and genetic susceptibility may be able to identify additional determinants of ethnic differences.
Footnotes
SM Conroy was supported by a postdoctoral fellowship on grant R25 CA 90956. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.