
Abstract
According to the WHO data [101,102], cervix and uterus cancer is the second most frequently detected type of cancer with approximately 500,000 new cases and 250,000 deaths per year.
Previously, the WHO recommended, in its 2005 Resolution [103], that its member states develop and reinforce cancer control programs in order to reduce the mortality and improve the quality of life of the women affected. In addition, the WHO published a cervical–uterine cancer complete control guide [102], which made recommendations for the prevention and early detection phases, preneoplastic lesions and cervical–uterine cancer invasive stage treatment, as well as the palliative care approach.
Within its preventive healthcare policy, in 2003 the EU published a recommendation work on cancer screening and the necessity of taking into account the cost–efficiency and the potential spin-off effects of the screening [104], and the special strategy guidelines for quality assurance in cervical–uterine cancer screening [105].
In relation to the Spanish Health Care System, the Carlos III Institute carried out a research on cancer in Spain in 2005 [106], ordered by the Spanish Health Ministry. The research served as a basis for the creation of the Cancer Strategy in the National Health Care System, published in 2006 [107], largely holding recommendations on different phases of the healthcare process. Additionally, the National Health Care System commissioned special reports on cancer screening (2006) [108] and the vaccine of the human papilloma virus (2007) [109].
In 2002, the Andalusian Health Care System published a study called ‘The integrated health care process of cancer of the cervix and uterus’ [110], a standardized healthcare plan for cancer of the cervix and uterus for nursing [111], as well as the portfolio of services in the primary health care of cervical and uterine cancer [112].
A recent bibliographical revision on the healthcare process of cervical–uterine cancer management in various geographical regions including Europe [1–11], North America [12–20], Latin America [21–25], Asia [26,27], Africa [28,29] and Oceania [30–33] indicates the general need to improve the accessibility and usage of cancer screening programs [1,3,8–10,14,23–24,26–27]. The aforementioned work highlights the motives, experiences and barriers for its utilization, including sanitary [24], social and cultural factors [10,14,23,27]. Other recurrent issues are the emotional side of diagnosis and treatment [7,21], the psychosocial effects [6,18,19], and the long-term quality of life [6,19,25,32], as well as the quality of healthcare at different stages of the process [4,5,13,17,22,25,30,31].
Among the studies reviewed, there were quantitative [8,15,17,21,24] and qualitative [4–7,14,18,19,23,27,31,102], as well as mixed methodologies [22,25,30], including certain studies that combine research and intervention. Special attention is paid to population groups with limited access to prevention services, among them, immigrant women [1,12], those of multiethnic origin [10], indigenous populations [30], women with low socioeconomic status [12], rural populations [22,23,27,29] and women in prison [14]. There was significantly less research on the experiences, needs and expectations of these women regarding the quality of healthcare. Although women's perceptions regarding cancer are conditioned by a combination of traditional beliefs and modern medical knowledge concerning risk and prevention [33], there is a general need for more information regarding the illness [34], improved access to health professionals and a more inclusive approach to their treatment [35]. Improved information regarding cervical cancer risk factors appears to reduce women's anxiety regarding their susceptibility to this disease [36]. Nevertheless, the studies highlight poor uptake of screening services and a reduced perception of vulnerability among the women surveyed [37]. It is also important to know that women value prevention as an important aspect of healthcare [38]. Given the importance of the patient's perspective in treatment outcomes, this article aims to clearly identify what women's needs and expectations are and examine how these correlate to their actual experience within the Andalusian Health Service.
Material & methods
For the present study we opted to use the methodology of focus groups and in-depth interviews with women in various stages of cervical and uterine cancer treatment.
Two focus groups and three in-depth interviews with 18 women were carried out. The participants were selected according to geographical, health status and sociocultural heterogeneity. The investigation included both healthy women attending the Cancer Early Diagnosis Program in health centers, women with precancerous lesions followed from primary healthcare and/or specialized care, and also women with cancer of the cervix and uterus undergoing specialized treatment. All of the women were users of health centers, outpatient consulting rooms and hospitals in Cadiz and Malaga. The inclusion criteria established were for the women to be, or have been, on one of the mentioned phases of treatment, while those women unable to participate in individual and group interviews were excluded. Initial contact was made by the researchers and those who agreed to take part were contacted later and invited to the sessions.
All participants received information on the methodology, the objectives and the contents of the study, ensuring confidentiality in the analysis of the results and thus gave verbal consent for participation.
The participants were asked about their experiences, needs and expectations at different stages of their treatment, following the SERVQUAL model [39]. A semi-structured scheme was used for the interviews.
The interviews were recorded, transcribed and their contents analyzed using the software program Nudist Vivo 1.0 (QSR International Pty Ltd, Doncaster, Victoria, Australia). The content analysis centered on the following aspects:
The patient's experience at various stages of their treatment (prevention and early detection phase, preneoplastic lesions and cervical and uterine cancer);
Perceived healthcare quality using the dimensions of an adapted SERVQUAL model [39] (accessibility, guarantee, personalized care and tangibility);
Strong points and priority demands.
Analysis and conclusions were compared among different members of the research team
Results
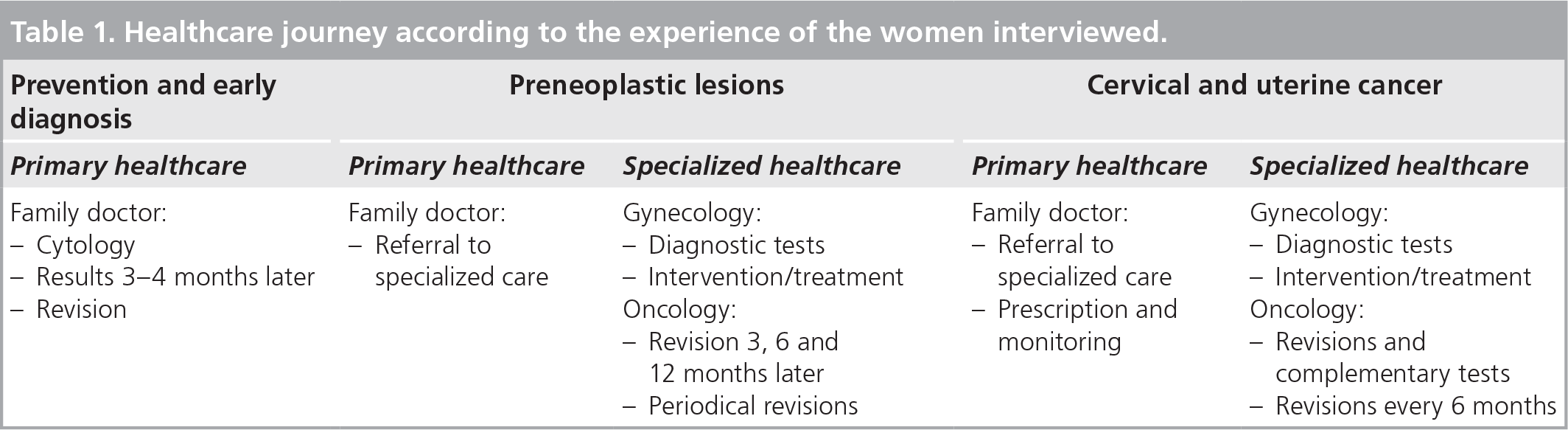
The women interviewed reported a highly structured healthcare process with three distinguished stages: prevention and early detection, treatment of premalignant lesions or cancer, and monitoring.
While the early detection process was carried out in primary healthcare center, preoperative testing and postoperative checks were performed in outpatient specialized care. The hospitalization phase included intervention and treatment
Healthcare journey according to the experience of the women interviewed
Experience of the process
Depending on the stage of care, the women interviewed related different experiences and needs.
Prevention & early detection phase
Despite being aware of the importance of the early detection of a possible lesion, some women admitted having postponed the review out of fear and anxiety, while other women prioritized regular reviews. One woman remarked, “And the truth is I get so nervous because I think: ‘Oh my God, there's something wrong with me’.” Another said, “But it doesn't matter while it's under control, the bad thing is not to go and have it.”
Methodology of the study.
Qualitative methodology (2007)
Two focus groups (seven healthy women attending early diagnosis program, aged between 35 and 55 years and eight women with preneoplastic lesions, aged between 35 and 55 years)
Three in-depth interviews (women with cancer of the cervix and uterus)
Primary healthcare
Specialized healthcare
Outpatient consulting room
Hospitalization
Accessibility
Guarantee
Personalized care
Tangibility
Another factor that could act as a barrier to the use of prevention services was the existence of contradictory information regarding the relevance and appropriate timing of cytology. In some cases, women confessed to having lost motivation for review because of a perceived lack of continuity on the part of health professionals. “Sometimes the doctor wants to do a lot of tests. But other doctors think it is not always necessary. So you think why don't they agree before asking you to come?”
As for the process of reporting the results, the women interviewed evaluated the waiting time as negative, and complained of not being informed when results were negative. This lack of communication was perceived as a lack of healthcare quality. One woman was told “Besides you don't have to come here for it, if there's something wrong we will summon you, and if we don't that's because all is fine.”
In general, the existence of a prevention and early detection program was viewed positively. There was a proposal of introducing regular check-ups in order to motivate the women to make use of the service. “Women like us, we should be offered yearly check-ups … Because if you are not summoned, you just don't go, you are frightened…”
Preneoplastic lesion
The women interviewed reported that being diagnosed with premalignant lesions produced a deep emotional impact and a high level of fear and anxiety. As an aid measure to confront the problem, they emphasized the importance of clear and concise information on diagnosis, treatment and prognosis. Regardless of the result, some women still sought a second opinion from a private clinician.
“When you heard this (diagnosis), you feel … miserable … and the doctor should help you deal with it, explain everything, and make things clear.”
Cervical & uterine cancer
The women who have had to deal with a diagnosis of invasive stage cancer, shared having experienced an emotional journey that began with rejection and denial until they eventually reached a point where they were able to accept the disease. Several study participants confessed that having missed both emotional and practical support from family members when they needed it. This lack of support contributed to disappointment and helplessness. One woman commented “And when you get home who does the meals? the cleaning? … and what happens when you need help?” Another said, “I thought I'd be cared for but I had to care for myself. You have to do it alone, no one will do it for you…”
In cases where a hysterectomy was required, some women expressed anxiety regarding the prospect of not being able to get pregnant, and welcomed the possibility of a mutual decision-making process that would permit them to postpone the operation in order to try having a baby before undergoing surgery. One woman said, “He said: ‘Look, you have got 6 months and that's as much as I can give you’. And then I didn't get pregnant, I just couldn't, I don't know what happened to me but when you get so obsessed you just don't get pregnant, so they had to operate me.” As emotional consequences of hysterectomy, the patients pointed out a feeling of emptiness, a feeling of being questioned on their femininity and sexuality itself, depression and the need to conceal the fact from their social network.
In order to know the perceived healthcare quality, the information received was structured using the following SERVQUAL model dimensions [39]:
Accessibility (easy access to health services)
Guarantee (professional competence, the quality of technology, the information received, the level of coordination between services, professionals and activities, and the perception of safety)
Personal attention (courtesy, trust, understanding and empathy, listening and interest)
Tangibility (the quality, comfort and cleanliness of the facilities, rooms and furniture, the quality of food during the hospital stay)
SERVQUAL dimensions
Accessibility
The weakest point identified was the waiting time for appointments and the reporting of results, which ranged from 3 to 8 months. To avoid long waiting times, the women with possible disease symptoms preferred to attend a private medical practice, despite considering the set of tests carried out by the public health service rather more complete. One woman said, “I trust public healthcare, but when you have to wait for so long, you sometimes prefer to go to a private doctor. It's normal, they can see you immediately.”
The participants identified certain differences in the degree of accessibility on different stages of the care process. A positive aspect of the prevention and early detection phase was the possibility of a direct summons to the prevention service, skipping the family doctor, and also when the consultation and testing could be performed the same day at the health center without having to go to the hospital. The patients named the lack of uniformity concerning the frequency of revisions criteria a weakness of the prevention programs. One woman said, “There are those like me, who never had a problem and we have been called for a review every year and yet others with observed changes are summoned every 3 years.” As a proposal for improvement, the patients asked for annual regular gynecological examinations, a protocol introduction to ensure its smooth realization, as well as an active systematic appointment service to women by the health center, with the objective of promoting the use of prevention services. In rural areas, an unequal coverage of gynecology professionals in medical centers appeared, and the demand was to extend the human resources to ensure the presence of a gynecologist in every center.
The women interviewed expressed the need for a faster referral to specialized care units as soon as a preneoplastic lesion was detected, to ensure a rapid intervention. Similarly, women diagnosed with cancer of the cervix and uterus, required a shorter waiting period between the time of biopsy and the intervention date.
At this stage of the process, the negative perception of waiting time periods seemed to warrant special priority: waiting for the results, the intervention, and the administrative process. Both in preneoplastic lesions and cases of invasive cancer, the women asked for a higher frequency of periodic reviews, one said, “It takes at least a month to carry out all the tests. Then you have to ask for an appointment again and then there are 3 to 6 more months to wait and when they give you the results it's been about a year or 9 months since the first appointment date. That's too much time in my opinion.”
Guarantee
The prior expectation was to improve the medical competence on deciding the diagnosis. Especially in the early detection phase of primary care there was a common fear of diagnostic mistakes and a lack of knowledge on the necessity of gynecological control. One woman commented, “If you have to do a smear test, you need a gynecologic examination, and you see that this doctor by the questions he asks and his way of putting things, is not prepared and that he shouldn't be there… They are family doctors who are now supposed to do a little bit of everything.”
In the prevention and early detection phase, the amount of information on the results was seen as an aspect of the guarantee dimension: the women interviewed demanded that they should receive reports of the results, whether a health problem has been detected or not. The feeling that the professionals did not take the significance of the need for information on the outcome seriously was perceived as a lack of healthcare quality. One woman said, “I had the tests last year and did not get the results, I would have liked to have them but I was just told that everything was fine, but I would have liked to have had them.”
Moreover, the women emphasized that the information they got, especially that on self-care practices, should be comprehensible and appropriate to each individuals cultural level.
Another aspect criticized was the lack of coherency between information campaigns, an aspect that reduced credibility in its efficiency and discouraged participation in them at all. The women interviewed required more campaigns, with clearer messages and recommendations.
The patients who have been treated for precancerous lesions expressed their need for a better control of appointments. They also requiered exhaustive information about their health.
The patients treated for cancer of the cervix and uterus associated guarantee to the so-called ‘technical quality’, showing a high degree of satisfaction with the perceived technical quality during the intervention and treatment. Both women treated for precancerous lesions and those treated for invasive stage cancer expressed a desire to have a counseling support during the process, both for themselves and their partners.
Personalized care
Patients from all phases express their need of being attended by the same professional (preferably a female gynecologist), during the process of treatment, thus allowing a deeper knowledge of a patient's health and personal history. One woman said, “That is true, our history is all there, whatever you want, but every time you come you have a different person attending you, and that's not correct in my opinion. I understand that they are all doctors, they read your cytology and know how things are, but it would be better if the same patients were always seen by the same doctor.”
Dimensions of the healthcare quality perceived, adaptation of SERVQUAL model.
Architectural barriers
Bureaucratic barriers
Waiting lists
Waiting time
Telephone access
Competence of the professionals
Adequate technology
Received information
Coordination between services, activities and professionals
Security
Courtesy
Generated confidence
Understanding and empathy
Listening
Interest shown
Courtesy
Generated confidence
Understanding and empathy
Listening
Interest shown
In the prevention and early detection phase, the lack of privacy in the medical centers was seen as negative by the patients. Another request was to receive more personalized care and to improve communication strategies by primary care physicians.
Those women who had to be treated for a preneoplastic lesion emphasized the importance of establishing good communication with the primary care physician. One woman said, “I got so much help from my family doctor. He said, for instance, you can come when you need to, even if you don't have a previous appointment, we will talk, and he phoned me at home every month… and thus supported me enormously.”
The cervical–uterine cancer patients highly rated the healthcare provided by oncology and nursery professionals, both in the sense of personalized attention according to each patient's need, and time to listen and the possibility to express doubts and fears. Another woman stated that, “The nurses were very attentive, the day before surgery as well. I needed treatment for an edema and they helped me with it, they were very friendly. They gave me a pill to stay calm overnight, then another one in the morning to be relaxed, well, I am very content. And you do not have to call them, they come without you having to call them.”
The patients stressed the importance of having the primary care services adequately technically equipped, so that all necessary tests could be carried out at the same medical center.
Women who had undergone surgery for cancer of the cervix and uterus had various recommendations for improvement: the cleanliness of the rooms, bathrooms and waiting rooms, adequate supervision of heating and air conditioning systems, and to better equip the rooms, with more comfortable chairs for family members. The negative aspects were having to share the room with more than two patients and the constant presence of the family members in the room. Regarding the hospital food, the wish expressed was to be able to choose between several menus
Improvement expectations at different moments of the care process of cancer of the cervix and uterus

Strong points & priority demands
In conclusion, the strong points of the cervical and uterine cancer healthcare process were the technical quality of oncology professionals, the personalized and human treatment from primary care physicians as well as medical specialists and nursing staff.
The priority improvement proposals included a greater coherence and consistency of the prevention campaigns, the reduction of waiting time for the appointments, the results of the tests and the intervention time, and, finally, improvement in communicating results.
Discussion & conclusion
Our study indicates that patients' experiences at various stages of treatment should be carefully considered when proposing strategies to improve treatment of cervical and uterine cancer.
The conclusions of the study are limited by the size of the sample. Although having 18 participants appears insufficient, the qualitative investigation indicates the information provided by the patients was extremely clear and concise. The women were able to express themselves and there was a broad consensus among the opinions voiced which, from our point of view, reflected the general view of patients' expectations and needs. This initial study with 18 women provided general information about their experiences and expectations, but we consider it important to complete this research in forthcoming studies. Our investigation should also be succeeded by others to look into more of the variables that may affect diagnosis and treatment experience, such as age, education, class, marital status and others.
Within the care process of cancer of the cervix and uterus, the phase of prevention and early detection receives special attention in the specialized literature. Early detection is considered to be essential and the election of adequate testing is needed, taking into account its cost–effectiveness and its potential psychological damage for the patients [1]. There are multiple research works [1,3,24,26] that investigate the factors influencing women's participation in screening. The aspects of potential influence can be considered:
Individual factors such as state of health [17,24], socioeconomic status [17,24], habit of attending primary care services, fear of adverse outcomes [24] and pain [17,27], and cultural aspects such as beliefs associated with the disease [23]; Factors related to health management, among them the accessibility [24], the quality of healthcare [17] and the information regarding routes of transmission of the disease [23] and the benefits of screening [27].
The women interviewed in this study are consistent in pointing out the fear of adverse effects as one of the major reasons for not attending screening. They add factors related to health management and physician–patient communication. In this regard, the problems highlighted include contradictory messages regarding prevention programs concerning the benefits and the frequency of testing and having experienced discouraging comments about the review from health professionals.
In cases of premalignant lesions or a diagnosis of cancer of the cervix and uterus, the participants describe having experienced a deep emotional impact that eventually gave way to the acceptance of the disease. The women interviewed identified the lack of family support and help in domestic affairs as an influential factor in the development of depression and despair during intervention and treatment. This process has also been mentioned in previous studies [15,19,21], which stated that there is a high degree of depressive symptoms in hospitalized oncology patients, as well as the fact that there is a relationship between positive psychological adjustment and the supportive attitude by the social and family environment. Referring to the evaluation of the quality of care, the participants highlighted the accessibility to comprehensive and understandable information as priority. The importance of improving the field of information and communication is also mentioned repeatedly in previous studies [4,6,10,19,23,28].
According to Walton et al., the availability of comprehensive information and the possibility of participation in decision-making provides an increasing sense of control over the patients' own lives [32]. The good technical quality and proper coordination between services and healthcare levels are identified as significant aspects in this phase of the healthcare process [12]. The women interviewed emphasized that as well as a good technical quality of care, personalized support by the family physician (phone calls, possibility to express doubts and the presence of a listening attitude) was equally important.
During the hospitalization phase, the women interviewed highlighted the lack of privacy and hygiene in the rooms as areas for improvement. This coincides with research conducted in British NHS hospitals that noted the lack of privacy in the hospital environment as the most critical point [5].
Various research [6,7,15–16,18,19,26,32] has investigated the influence of the disease on life quality in the long term, identifying the influence of physical problems [15–16,18,26], the strategies of psychological adaptation [15,19], social and cultural beliefs [6], as well as the understanding and being accompanied by health professionals, especially nurses [7]. The sexuality problems experienced have been identified as aspects that negatively influence quality of life [15–17]. As a consequence, the relationship and communication between the patients and their physicians and nurses are considered to be highly important in order to respond to most of the patients' needs [18].
The participants of the present study confirm the impact of the disease on the quality of life, sexuality and corporal self image [6–7,15–16,18,19,26,32], as well as significance of a proper physician–patient communication and the opportunity to participate in decision-making. At this point, the continuity of care appears as extremely important for the interviewed women, as it provides better information, more trust and more effective communication channels.
The needs of the women interviewed confirm the significance of comprehensive and personalized healthcare especially in the post-treatment phase [26].
The patients' experiences and proposals described by themselves are an important factor in the process of improvement of healthcare quality [39,40]. The expectations expressed by the women interviewed in this study were included in the design of integrated healthcare process of cervical–uterine cancer by the Andalusian Health Service, published in 2002 [110]. The recommendation is to conduct further research, making use of a qualitative methodology in order to provide, from the perspective of the users, the guidelines for an improved treatment and attention for patients with cervical–uterine cancer.
Future perspective
We think the patients' expectations and needs are highly important and are liable to play a greater part in shaping health policy and treatments in the future. Researchers should enhance their efforts to identify areas where healthcare delivery falls short of patients' expectations and propose effective strategies to respond to their needs.
Executive summary
Considering the importance of including the patients' opinions, this study aims to describe women's experiences, needs and expectations about the treatment of the cervical and uterine cancer.
Qualitative methodology with 18 women, using focus groups and personal interviews. The study looked at different stages of the treatment and used SERVQUAL criteria to analyze its findings.
The qualitative methodology allows indepth knowledge of women's needs and expectations.
The experience regarding treatment depends on the stage of the illness: prevention and early detection, preneoplastic lesion or cancer.
The perceived healthcare deficiencies include long waiting time for the check-ups, a lack of accessibility, the need of medical competence, personalized care and improved patient-physician communication.
As proposals of improvement of the SERVQUAL dimensions, women identify: the design of a protocol for annual regular gynecological examinations, an active systematic appointment service to women by the health center, a faster derivation to specialized care units, a higher frequency of periodic reviews, the demand of being delivered comprehensible and appropriate reports of the results, a better administrative control over the tests, to be attended by the same professional.
Patients' experiences during the different stages of the treatment are aspects to take into account and are to be incorporated during the process of proposing strategies to improve care for the treatment of cervical and uterine cancer.
Footnotes
The authors receive funding from FEDER and Consejería de Economía, Ciencia e Innovación. Grupo CTS-177. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.