
Abstract
The importance of stroke in women is gaining increasing recognition in both clinical and public health environments [1,2]. Because of the increased life expectancy of women, there are more stroke events in women than in men, even though in all but the very oldest age groups age-specific incidence and mortality rates are higher in men than women [1]. Stroke is also important in women because women appear to not fare as well after a stroke event compared with men; stroke-related outcomes, including disability, functional status and quality of life are consistently poorer in women than in men, yet the reasons for this are not well understood [3,4]. Some of the reasons for poor poststroke outcomes undoubtedly stem from the fact that women are older (by approximately an average of 4 years) than men when they have stroke, but accounting for these age differences or differences in the burden of risk factors and comorbidities prior to the stroke event does not account for all of these observed differences [1]. The impact of stroke on women is also exacerbated by the fact that elderly women, compared with their male counterparts, are much more likely to live alone and be socially isolated at the time of their stroke, and so may be less able to adapt to the changes that a stroke event imparts [5,6].
A major development in the treatment of stroke over the last 15 years has been the approval of intravenous tissue thrombolysis (IV tPA) therapy for acute ischemic stroke. If given within 3 h [7], and possibly up to 4.5 h [8], tPA can significantly reduce the level of disability observed in patients 90 days after treatment. Despite the promise of tPA therapy, the stroke community has found it challenging to implement this treatment effectively and equitably in many communities. The proportion of ischemic stroke patients who are actually treated with tPA has historically been low, often not reaching more than 3–4% of all ischemic stroke admissions in the USA [9], although more recent data from national quality improvement registries, such as Get With the Guidelines® Stroke have shown great improvements in the proportion of eligible stroke patients treated [10].
The availability of tPA treatment for acute ischemic stroke has raised two important sex-based issues, one related to the potential for sex differences in the efficacy of tPA, and the other related to sex differences in the utilization of tPA. Empirical data illustrating the potential for sex differences in the efficacy of tPA was first shown by Kent and colleagues [11], who undertook a pooled analysis of three randomized placebo-controlled clinical trials of IV tPA [7,12–14]. The analysis showed that women received a substantially greater benefit from tPA treatment compared with men. These results were interpreted as showing that tPA had the potential to eliminate the sex difference in functional outcomes poststroke that were observed in the placebo groups of these three trials, as well as in many other observational studies [1,3,4,15].
Given that there is evidence that tPA is more effective in women than men, it is disquieting to find evidence that women may in fact be less likely to receive IV tPA treatment than their male counterparts. Several studies that have reported on the frequency of IV tPA use in both men and women have shown a trend towards women being less likely to receive treatment [16]. These reports have included a wide range of study designs and data sources including academic and community-based medical centers, registries and administrative databases [15,17–23]. A recent meta-analysis of these studies found that women had approximately a 30% lower likelihood of receiving IV tPA treatment compared with men, although there was significant variability between studies [24].
The goal of this article is to provide a review of the published literature addressing sex differences in both the utilization and efficacy of IV tPA, to discuss some of the reasons for these differences, and to discuss the implications of these findings for both the public health and clinical communities.
Methods
Search strategy & selection criteria
We identified studies that reported on sex differences in either the utilization or outcomes of IV tPA treatment for acute stroke, paying particular attention to recent meta-analyses. For the utilization of tPA, we used data from a recent meta-analysis that was conducted by our research team [24]. For this meta-analysis, studies of primary interest were those that reported on the use of IV tPA in a representative sample of women and men with acute ischemic stroke in typical hospital settings. Typical hospital settings included community-based or academic referral hospitals, as well as regional or national registries and administrative data sources. Eligible studies must have reported data on the IV tPA treatment rates in female and male acute stroke patients (or have provided sufficient data so that rates could be calculated), and were published before April 2008. For this current publication we updated the original search strategy to include relevant articles published between January 1995 and December 2010. We searched MEDLINE, EMBASE and the ISI Web of Science databases using the following combination of terms:
Cerebrovascular accident (MeSH) or stroke, and;
r-tPA or tPA or thrombolytics or thrombolysis, and;
Sex, sex factors, sex ratio, sex distribution, gender and gender difference.
For the efficacy of tPA, studies of primary interest were randomized placebo controlled trials investigating IV tPA in acute ischemic stroke patients. Eligible studies must have reported data on the efficacy of tPA treatment in female and male acute stroke patients. To identify potentially eligible studies we first searched MEDLINE, EMBASE and the ISI Web of Science databases for all relevant trials and/or meta-analyses published during the same 1995 to 2010 time period using the following combination of terms:
Cerebrovascular accident (MeSH) or stroke, and;
Randomized control trial or RCT, and;
r-tPA or tPA or thrombolytics or thrombolysis, gender and gender difference.
After identifying all tPA trials (which included intra-arterial [IA] use), we then searched each article to determine if sex-specific estimates or interaction-based estimates of the efficacy of tPA in men and women were presented.
Results
Utilization of IV tPA
A total of 18 studies published between 2001 and 2008 were included in the prior meta-analysis examining differences in the utilization of IV tPA by sex [24]. Ten studies were based on data from North America, six from Europe, one from Australia and one from Israel. The study designs covered the spectrum from single hospital studies (n = 5), multiple hospitals (n = 6), registries (n = 4) or administrative datasets (n = 3). A total of 16 studies provided data on tPA use amongst all ischemic stroke admissions
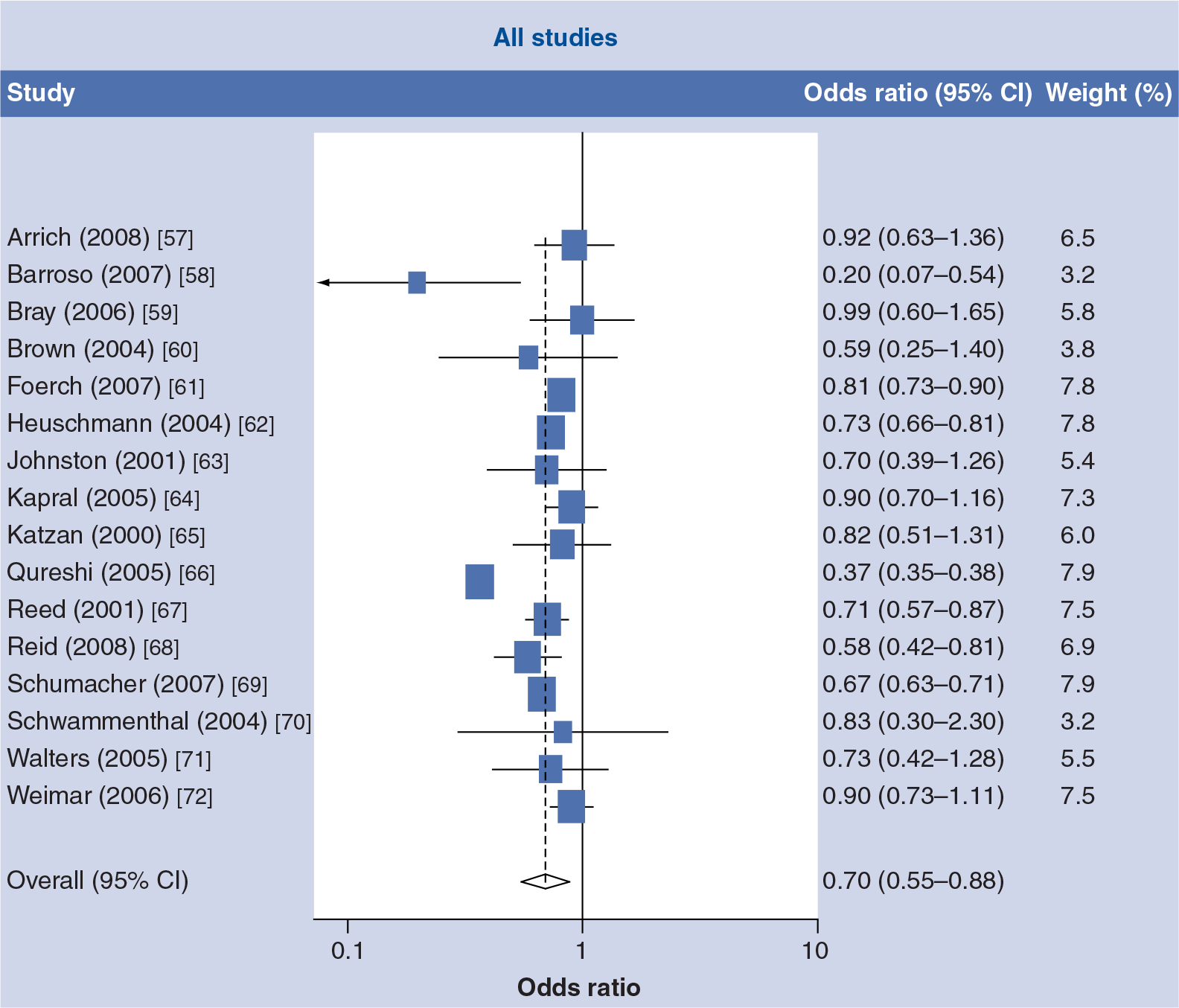
Forest plot of the unadjusted odds ratio of intravenous tissue thrombolysis use in women compared with men in all acute ischemic stroke admissions.
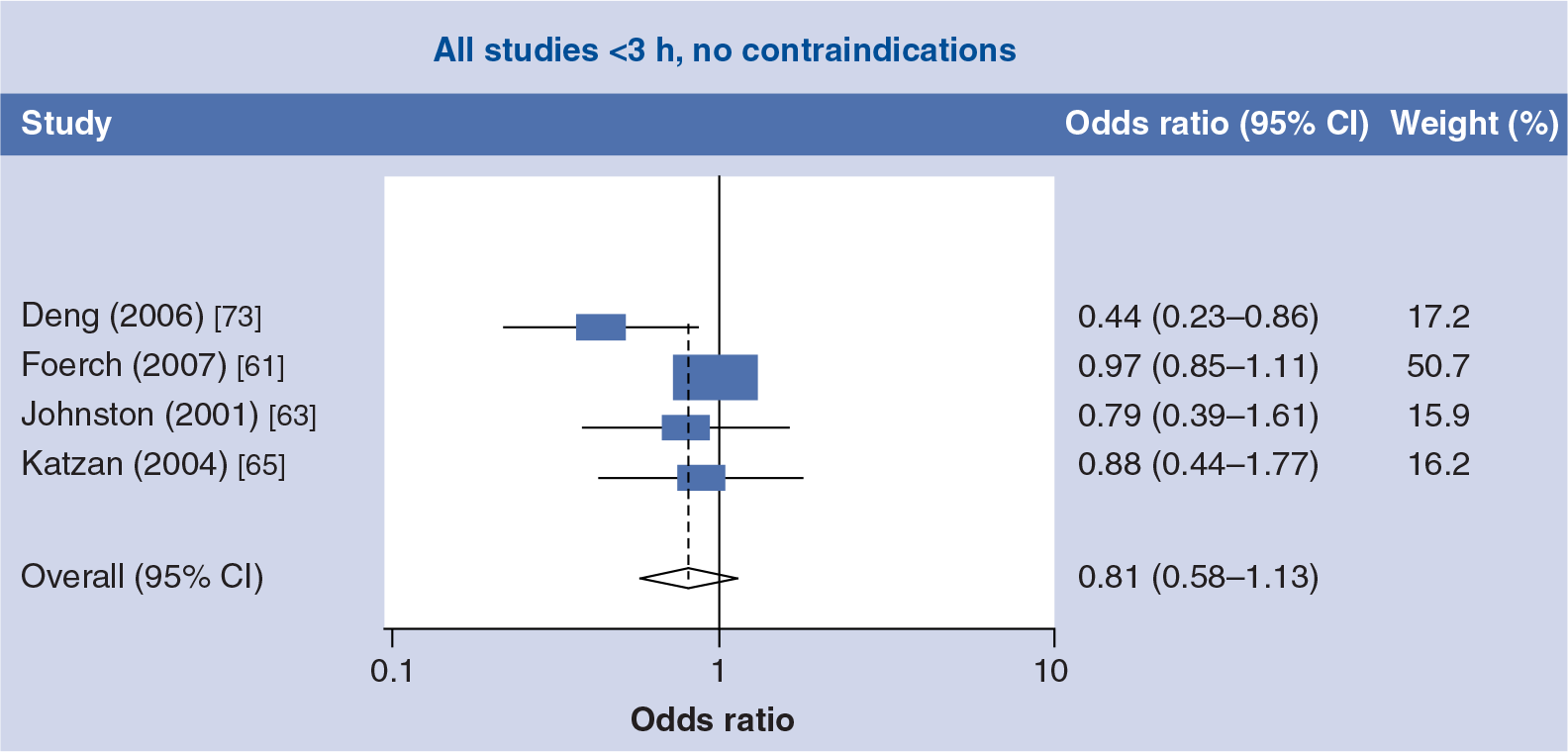
Forest plot of the unadjusted odds ratio of intravenous tissue thrombolysis use in women compared with men in the eligible subgroup who arrived within 3 h of onset with no contraindications (<3h, no contraindications).
Studies published since this meta-analysis, however, have generally found limited sex differences in the utilization of IV tPA, although findings were again variable. Data from the Swedish Risk-Stroke Registry in 2006 found that among ischemic stroke cases ≤80 years of age, thrombolysis rates were similar in men and women (3.4 vs 3.3%, respectively) [27]. In an analysis from the same registry that examined trends in use of tPA between 2003 and 2008, the adjusted odds ratio of thrombolysis was slightly higher in men compared with women (adjusted OR: 1.06; 95% CI: 1.00–1.12) [28]. In the USA, a study of consecutive ischemic stroke patients seen at 32 academic centers found that IV tPA treatments rates were comparable in men and women (7.5 vs 6.5%, respectively, p = 0.49) [29], while data from the Get With the Guidelines Stroke registry from 2003 to 2008 found that, among ischemic stroke cases who arrived within 2 h of symptom onset, thrombolysis rates were slightly lower in women compared with men (55.8 vs 59.4%); a difference that remained significant after multivariable adjustment (adjusted OR: 0.91; 95% CI: 0.86–0. 95) [30]. Finally, a study of acute stroke cases entered into a ‘code stroke’ database from six emergency departments in the San Diego area found that women were more likely than men to receive tPA (38 vs 32%, respectively) [31].
Efficacy of IV tPA
Our systematic search identified several randomized placebo controlled trials of IV tPA for acute ischemic stroke [7,12–14,32], as well as the most recently updated Cochrane review of thrombolysis treatment trials [33]. After examining the individual reports from the trials included in the Cochrane review we did not find any sex-specific estimates that addressed the efficacy of tPA treatment in men or women. Thus, the only available data remains to be the pooled analysis of the three randomized clinical trials of IV tPA conducted by Kent and colleagues [11]. The analysis showed that the proportion of men and women who had positive outcome (defined as modified ranking scale [mRS] of ≤1) following tPA treatment was similar (38.5% in men vs 40.5% in women; p = 0.50), whereas among the placebotreated group, women had significantly worse outcome (36.7% in men vs 30.3% in women; p = 0.03). These data therefore indicate that there was a significant interaction between sex and tPA treatment, with women receiving a substantial and statistically significant greater benefit of tPA treatment (i.e., mRS ≤1 40.5% with treatment vs 30.3% without; p = 0.0008), while men received no such benefit (i.e., mRS ≤1 38.5% with treatment vs 36.7% without, p = 0.52). These data indicate that tPA treatment eliminated the sex-differences in poststroke functional outcomes that were observed in the placebo groups of these trials (a so-called ‘nullification’ effect). These findings remain the primary evidence for sex differences in the efficacy of IV tPA for ischemic stroke treatment. It should be noted that a similar sex difference in the efficacy of IA thrombolysis treatment (Pro-Urokinase) was found in a randomized trial of ischemic stroke patients with middle cerebral artery occlusions [34].
We identified several observational studies including registry-based studies that attempted to quantify the relative benefits of IV tPA treatment in ischemic stroke patients by examination of post-treatment outcomes in men and women [35–37]. A recent meta-analysis by Meseguer and colleagues of 16 such observational studies published in 2009 found no evidence of a sex difference in favorable outcomes after IV tPA treatment [38], which is consistent with the results of the pooled analysis of the randomized trials [11]. However, as discussed by both Kent [37] and Jananovic [36] results from these observational registries – which are essentially large case series of treated cases – should be viewed with caution, since the absence of a control population means that such analyses have to rely on risk-adjustment methods to satisfactorily account for baseline sex differences in outcomes that have been shown repeatedly to be clinically important. It is highly unlikely that current risk adjustment models for stroke outcomes are sufficiently well developed to satisfactorily account for these differences [39,40]. Hence, meaningful interpretation of the lack of a sex difference among treated cases is difficult, if not impossible. However, a recent observational study of IV tPA use in the Canadian Stroke registry, published by Shobha and colleagues in 2010 [41], did include untreated patients, and was therefore able to examine sex differences in the effectiveness of tPA by making a direct comparison between treated and nontreated groups. The results support the conclusions of Kent's analysis; the findings showed that untreated women had a worse outcome than untreated men, but when both sexes were treated with IV tPA, their outcomes were similar (thus the sex-difference was nullified after treatment).
Conclusion
There is reasonably strong evidence that there are clinically important sex differences in both the efficacy and utilization of IV tPA, with women gaining more benefit when they receive treatment, but paradoxically being less likely to receive IV tPA treatment (although there is more variability across studies in the latter finding). Larger placebo-controlled thrombolysis trials, specifically powered to look at sex differences in treatment efficacy, are required to better elucidate the potential for sex differences in tPA efficacy [42]. An important ongoing study is the Third International Stroke Trial (IST-3), which is a placebo controlled randomized trial of IV tPA given within 6 h of the onset of symptoms. This trial should provide important data regarding the presence of a sex difference in tPA efficacy since it is a large study (the planned enrollment is 6000 patients), there is no upper age limit for eligibility (which should increase the number of women included in the trial), and there is a preplanned subgroup analysis by gender [43]. If sex differences are shown to exist in this and other future tPA trials, then this should stimulate more research on understanding the biological basis for the greater efficacy of tPA among women.
The exact mechanisms for the enhanced efficacy of tPA in women are not known with certainty. Higher recanalization rates in women following IV tPA treatment has been proposed as one potential mechanism for the greater efficacy of IV tPA in women [44]. However, differences in recanalization rates have not been observed in reports that have examined sex differences in the efficacy of IA tPA [34,45,46]. The absence of any sex differences in recanalization rates after IA tPA use has been explained by the higher doses of tPA used in IA applications; IV tPA treatments are administered in a fixed-dose fashion, while IA treatments are administered until recanalization is achieved or a maximum dose is reached [46].
Numerous explanations for the greater efficacy of IV tPA in women have been proposed [44,46], including the fact that occlusions that result from cardioembolic sources (which are more common in women)[47,48] are richer in fibrin and are more easily dissolved compared with the platelet-rich occlusions that characterize thomboembolic strokes [35,44]. Other explanations have included the fact that women generally have smaller intracranial arteries and smaller clot volumes, which can result in greater efficacy of IV tPA and increased recanalization [49], as well as the fact that women may be less likely to have internal carotid artery/middle cerebral artery (ICA/MCA) occlusions that have a lower recanalization rates than isolated MCA occlusions [44].
The exact causes of the observed sex disparity in IV tPA use for ischemic stroke are not known. Additional representative registry-based studies should be undertaken in order to learn more about the variation in the utilization of tPA in women across hospitals and regions, and to determine whether these differences are decreasing now that this phenomenon has been widely reported. Whether hospitals that participate in systems-based quality improvement programs, such as Get With the Guidelines Stroke or the Riks Stroke Registry, are less likely to have sex differences in the quality of care (including tPA treatment) remains an important question. Sex differences in the eligibility criteria for tPA treatment, particularly arrival time, may impact treatment decisions for women. However, while some studies have found longer prehospital delays in women with stroke [50], most have not [1,51,52]. Compared with men, women are older at the time of their stroke and are more likely to live alone [5,6], and so it may be more difficult to establish symptom onset time and perhaps to obtain consent for treatment. The presence of more atypical symptoms in women with stroke, such as chest pain and shortness of breath, has been thought to potentially impact delayed diagnosis and create other in-hospital delays [53]. An analysis of sex differences in emergency department delays (door-to-doctor and door-to-image times) from a Michigan stroke registry found that while women did present with somewhat different symptoms compared with men, these did not account for the longer in-hospital delays that women experienced [54]. Numerous contraindications and warnings for IV tPA have the potential to contribute to lower treatment rates in women; for example, the increased prevalence of atrial fibrillation, cardioembolic stroke and potential for greater stroke severity (as indicated by increased coma or altered consciousness) in women [3,15,53,55] could all lead to clinicians being more cautious about using IV tPA in women. It has also been suggested that sex differences in the acceptance of thrombolysis treatment may also contribute to the observed finding that women are less likely to receive tPA [56].
Executive summary
There are more stroke events in women compared with men and women have poorer outcomes in terms of disability, functional status and quality of life.
Intravenous tissue thrombolysis (IV tPA) is a proven therapy for reducing disability in acute ischemic stroke patients, and studies indicate that it may be more effective in women compared with men.
However, evidence also points to women being less likely to receive IV tPA treatment.
We updated a previous meta-analysis examining observational studies of sex differences in the utilization of IV tPA.
We conducted a comprehensive review of clinical trials, observational studies and meta-analyses of studies examining sex differences in the efficacy of IV tPA.
Data from observational studies published before April 2008 of IV tPA use show evidence of under-utilization in women, although wide variability between studies suggests that differences are specific to local conditions and populations.
More recent studies have generally found limited sex differences in the utilization of IV tPA, although findings are again variable.
Prior analyses of randomized trial data show strong evidence that women but not men receive statistically and clinically significant benefit from IV tPA treatment.
Most observational studies of the effectiveness of IV tPA treatment in men and women have limited validity because of the absence of comparable control groups.
There is reasonably strong evidence that there are clinically important sex-differences in both the efficacy and utilization of IV tPA, with women gaining more benefit when they receive treatment, but paradoxically being less likely to receive IV tPA treatment.
Reasons for the greater efficacy of IV tPA in women are unknown but possible explanations included higher recanalization rates resulting from clinical and biological differences in ischemic stroke lesions in women.
Larger placebo-controlled thrombolysis trials, specifically powered to look at sex differences in treatment efficacy are required.
Footnotes
Mathew J Reeves receives salary support from the Michigan Stroke Registry and serves on several American Heart Association's Get With the Guidelines Committees. Lee H Schwamm serves as chair of the American Heart Association's Get With the Guidelines Steering Committee; serves as a consultant to the Research Triangle Institute and to the Massachusetts Department of Public Health, and serves on the international steering committee for the DIAS-4 trial of thrombolysis (Lundbeck). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.