
Abstract
Sex differences exist in the occurrence, treatment and outcome of ischemic stroke. Compared with men, women have more stroke events and are less likely to fully recover from a stroke. Given the rapidly aging population, stroke incidence and mortality among women are projected to substantially rise by 2050. This has important public health consequences. Mitigating the burden of stroke among women will require a fundamental understanding of sex differences and sex-specific issues including cerebrovascular disease pathophysiology, treatment and outcome. An aspect of stroke treatment receiving increasing but insufficient attention involves possible interactions between estrogen levels, antiplatelet drugs and stroke outcome. Emerging evidence suggests that antiplatelet therapy may provide primary stroke protection but not primary myocardial infarction prevention in women, while the opposite may be true among men. Understanding sex-specific issues related to women who experience stroke is critical to clinicians who treat women with antiplatelet medications as part of a secondary stroke prevention regimen; however, the ideal antiplatelet medication, and dose, in women requires further research. In this article we present a conceptual framework for sex differences in antiplatelet treatment response in ischemic stroke, thrombus formation and the mediating role of estrogen, sex differences in antiplatelet treatment response in clinical trials, and sex differences in antiplatelet treatment use in ischemic stroke.
Keywords
Women disproportionately shoulder the societal burden of stroke compared with men: annually 55,000 more women than men experience a stroke [1]. Furthermore, stroke outcomes, including disability and quality of life (QOL), tend to be generally poorer in women than in men [1]. The public health impact of the differential effect of stroke on women will continue to grow over subsequent decades as an aging population leads to an ever greater number of stroke events in women. Indeed, there are already projections that excess stroke deaths in women will steadily rise from 32,000 excess stroke deaths in 2000 to nearly 68,000 by 2050 [2].
With limited proven acute stroke treatment strategies, prevention remains the most viable avenue for mitigating the increasing toll of stroke among women. Modest reductions in the incidence of strokes over the past decade have been attributed to better recognition and control of traditional stroke risk factors [1]. However, these reductions in stroke occurrence seem to have benefited men more than women [3]. Moreover, women have unique stroke risk factors including the menopausal transition (women have their first stroke at older ages than men leading to theories linking lack of estrogen in menopause to higher stroke risk) and atrial fibrillation. While the proportions of etiology of stroke in women mimic that of men, women are significantly older when first stroke occurs (75.1 vs 71.1 years; p < 0.001) [4]. This increased age at first event may be related to the effects of a rapid decrease in estrogen levels in the postmenopausal state leading to the loss of its neuroprotective benefits. While the effects on the vasculature are immediate, the clinical consequences of increased risk of stroke and heart disease may not be seen for some time. In addition to age, the imbalance of stroke risk factors for women versus men, show that women are more likely to suffer from atrial fibrillation (1.1 vs 0.8%; p < 0.001) and hypertension (33.8 vs 30.0%; p < 0.001) [5]. By contrast men have a higher incidence of history of heart disease, myocardial infarction, peripheral arterial disease, diabetes and alcohol and tobacco use [6–9]. The identification of prevalent risk factors in women can guide the use of either antiplatelet or anticoagulation therapy for the prevention of ischemic stroke.
In view of this, there is growing focus on improving the understanding of sex differences and sex-specific issues in cardiovascular diseases. In this article, we examine thrombus formation and the mediating role of estrogen, as well as sex differences in antiplatelet treatment response for ischemic stroke.
Conceptual framework for a sex differential in antiplatelet treatment response
A conceptual framework for sex differences in antiplatelet therapy response among patients with ischemic stroke is presented in

Conceptual framework for sex differences in antiplatelet therapy in ischemic stroke.
Endogenous estrogen plays a mediating role in the ischemic process, although the exact mechanisms have not been described. Molecular, murine and human studies have suggested that endogenous estrogen provides dual neuroprotection effects via cerebral vasodilatation and antioxidant effects, while synthetic exogenous estrogens increase stroke risk in postmenopausal women with extended use [10,11]. It is theorized that via its dual neuroprotective effects, endogenous estrogen mediates the degree of brain tissue ischemia induced by thrombus, thereby decreasing brain tissue damage and therefore, neurologic deficit. In addition, estrogen may mediate the formation of thrombus via its activity on platelet surface receptors.
Thrombus formation
Phases of cell-based coagulation
Platelets activated by endothelial tissue injury, such as that caused by atherosclerosis, acquire an enhanced capacity to catalyze interactions between activated coagulation factors [12]. This activation has traditionally been described as the intrinsic and extrinsic pathways of the coagulation cascade as independent means of clot formation. However, more recent evidence suggests that these pathways are not independent, and the coagulation process has been reconceptualized as a cell-based process that functions to initiate, amplify, and propagate formation of the thrombus
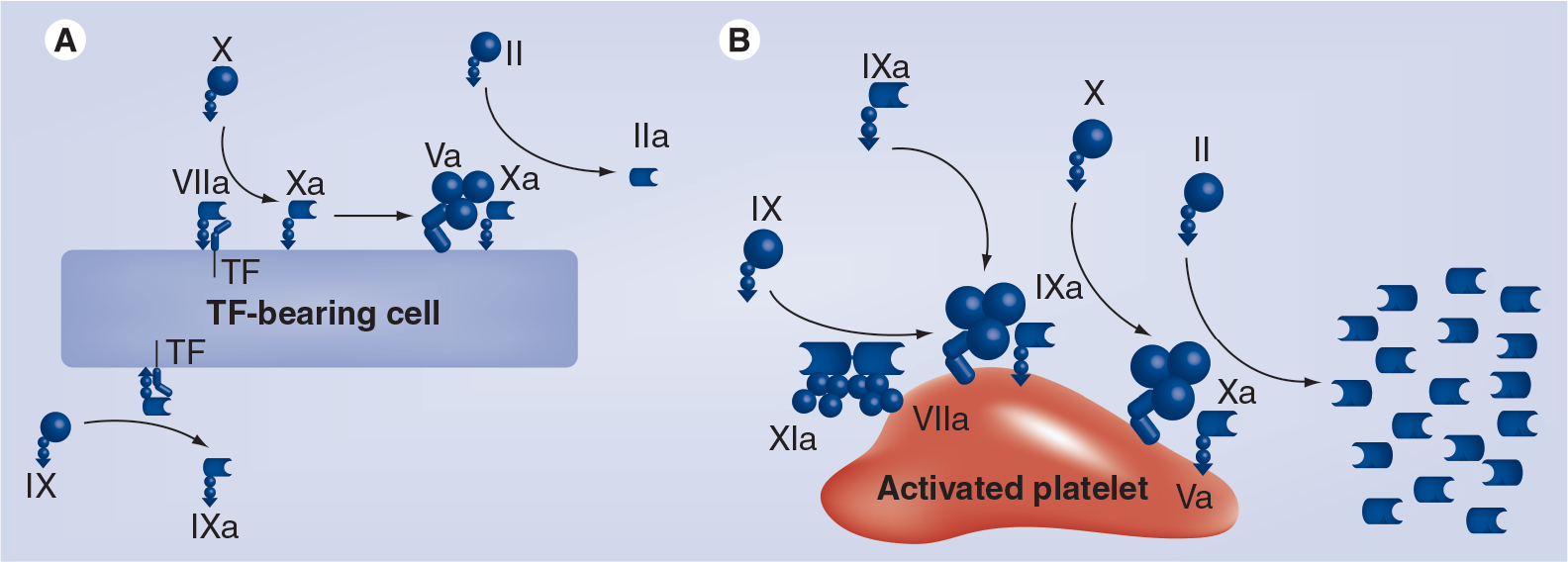
Cell-based coagulation model.
The initiation phase of coagulation
The initiation of clot formation begins when injury to the subendothelium leads to exposure or expression of tissue factor (TF), a protein present in subendothelial tissue, platelets and leukocytes to the blood stream [14]. The coagulation process that occurs on TF bearing cells primarily functions to build a strong fibrin (FIa) mesh network to form a stable clot. When TF is expressed, it combines with activated factor VIIa (FVIIa) (activated by thrombin) that is present in the bloodstream. This combination (TF/FVIIa) activates two other factors that are present in the circulating blood; IX (FIXa) and X (FXa). When activated FXa and activated factor V (FVa) combine, the resultant prothrombinase complex FXa/Va is formed at the site of tissue injury. The FXa/Va complex causes a conversion of a small amount of prothrombin (FII) to thrombin (FIIa). FIIa leads to the conversion of fibrinogen (FI) to FIa. Coagulation only proceeds to the amplification and initiation phase when the factor VIII/von Willebrand Factor complex are spilled out into extravascular tissue secondary to vascular injury
The amplification phase of coagulation
Whereas the initiation phase occurs on endothelial cells expressing TF, the amplification phase occurs on the activated surface of circulating platelets
The propagation phase of coagulation
The propagation phase of coagulation also occurs on the activated platelet surface
Thrombolysis
Immediately after forming the thrombus, the process of disrupting the thrombus, thrombolysis, begins. Tissue plasminogen activator (t-PA) naturally exists in the circulating blood stream to prevent a stable clot from becoming a vascular occlusion. t-PA converts circulating plasminogen and plasminogen within the forming clot to its active state, plasmin. Plasmin dissolves the FIa networks within the clot, which leads to a dissolution of the clot and resumption of normal blood flow in the area. In pathologic clot formation, as in stroke, the inherent t-PA is unable to dissolve the FIa networks at a faster rate than they are being created. This eventually leads to vascular occlusion and infarct.
Platelet surface receptors
Across the phases, platelet surface receptors play an important role in thrombus formation. Both platelet aggregation and thrombus formation result from activation of platelet surface receptors subsequent to activation of coagulation pathways. Each of the platelet receptors illustrated in
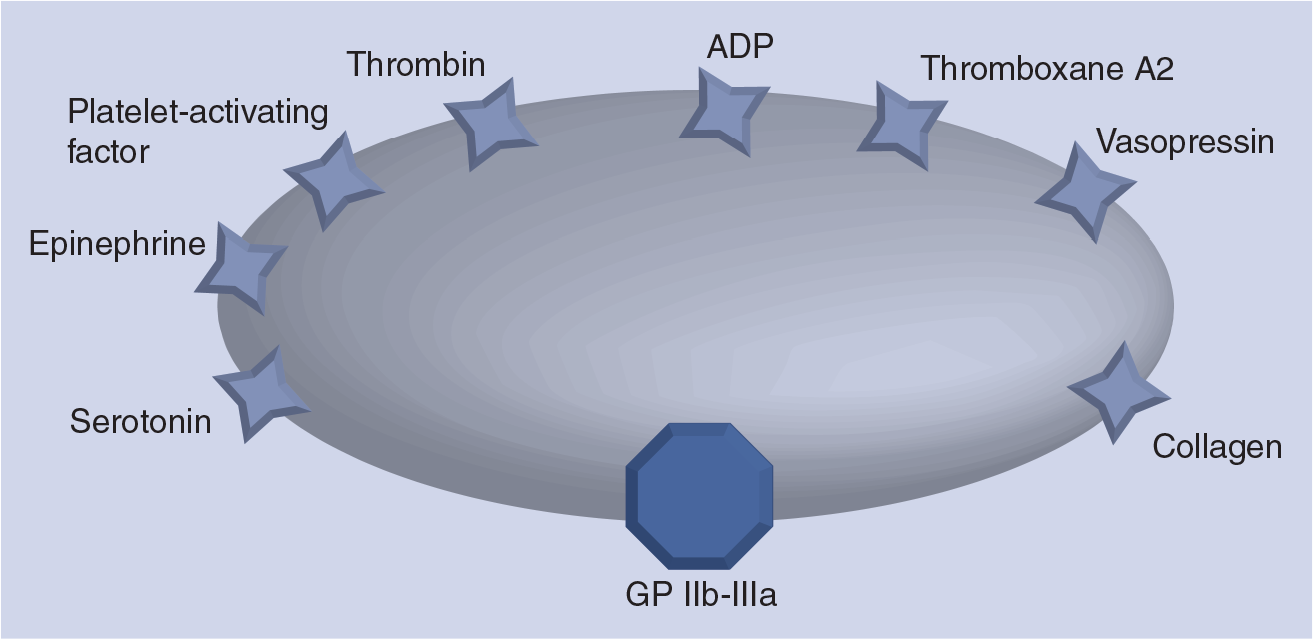
Platelet surface receptors.
Estrogen & its effect on cerebral ischemia & platelets
Sex hormones exert differential effects on platelet function, with testosterone enhancing platelet activity and estrogen inhibiting it. Estrogen is a natural steroid that is formed from androgen precursors, secreted chiefly by the ovaries, placenta, adipose tissue, and testes, and that stimulates the development of female secondary sex characteristics and promote the growth and maintenance of the female reproductive system [15,16]. 17-β-estradiol (E2) is the predominant human estrogen that binds to an estrogen receptor (ER) expressed on the surface of target cells. Serum estradiol measurement in women primarily reflects the activity of the ovaries. As such it is useful in the detection of baseline estrogen in women and to determine reproductive stage. In humans, estrogen is measured by serum estradiol levels which generally range between: 13–166 pg/ml in the follicular phase; 86–498 pg/ml in the ovulation phase: 44–211 pg/ml in the luteal phase; <65 pg/ml in postmenopause; <43 pg/ml in males; and <25 pg/ml in prepubescent males and females [17].
Platelets contain ERs on their surfaces which become upregulated in the absence of estrogen (i.e., menopause), thus lowering the threshold for platelet activation and increasing the propensity to clot formation via increased expression of adhesion molecules, and the ligand CD40 [18]. Rodent studies have shown that acute estrogen deficiency increases postischemic platelet reactivity and treatment with estrogen doses to physiologically premenopausal levels decreases this hypersensitivity [19]. A recent study of acute antiplatelet loading in a rabbit model of embolic stroke has shown that higher serum endogenous estrogen levels result in improved clinical outcome after stroke treatment [Meyer D, Compton P, Gylys K, Zivin JA, Eastwood J, Unpublished Data]. In the presence of postmenopausal, prepubescent endogenous estrogen levels, platelet reactivity is decreased and the affinity for platelet aggregation and thrombus formation reduced. Thus, it can be hypothesized that one of the neuroprotective effects of estrogen in relation to ischemic stroke is in the mediation of thrombus development. In addition, the neuroprotective effects of endogenous estrogen may further mediate the ischemic process by raising the threshold of exhaustion for infarction resulting in less ischemia and therefore less neurologic deficit. Conversely, the administration of exogenous estrogen (i.e., estrogen replacement therapy) has been show to increase the risk of stroke and myocardial infarction in postmenopausal women [20]. A possible explanation for this is that endogenous estrogen plays a molecular role in physiology that cannot be mimicked by synthetic hormones. The effect of estrogen on platelets is likely multifactorial and clear mechanisms of action must be delineated to improve ischemic stroke treatment and prevention in women.
A study of platelet aggregometry before and after two weeks of low-dose aspirin treatment showed that women exhibited the same or greater decreases in platelet reactivity after aspirin therapy compared with men, but women also retained slightly more platelet reactivity. No major differences were seen in women by menopausal status or use of exogenous hormone treatment. Of note, following aspirin intake both men and women had total suppression of the cyclooxygenase-1 pathway, which is the main pathway for vascular protection.
Sex differences with antiplatelets in ischemic stroke
Antiplatelet medications are currently and widely used for the secondary prevention of stroke. These medications serve to prevent the formation of thrombi in order to prevent further vascular occlusion and ischemia in at-risk individuals. The three mainstay antiplatelet medications currently utilized in secondary stroke prevention are aspirin, clopidogrel (Plavix®, Bristol-Myers Squibb/Sanofi Pharmaceuticals partnership, NY, USA), and extended release aspirin/dipyridamole (Aggrenox®, Boehringer Ingelheim, CT, USA). These antiplatelet medications prevent platelet aggregation by different mechanisms and data show significant decreases in the risk of secondary stroke, myocardial infarction and death with each drug [21–23].
An analysis of the Nurses' Health Study revealed that women who used aspirin long-term experienced significantly lower mortality rates, particularly cardiovascular mortality [24]. The only primary prevention randomized controlled trial of aspirin in women, the Women's Health Study (WHS), compared 100 mg of aspirin every other day versus placebo in healthy women over age 45 years [25]. The primary result of WHS indicated no overall benefit in the confated end point of first major cardiovascular event (nonfatal myocardial infarction, nonfatal stroke or death from cardiovascular disease) for the aspirintreated subjects, but there was a favorably lower rate of ischemic stroke events. A meta-analysis of randomized trials of primary prevention with aspirin focused on sex-specific outcomes showed that aspirin in women reduced the risk of overall stroke (HR: 0.83; 95% CI: 0.70–0.97) and ischemic stroke (HR: 0.76; 95% CI: 0.63–0.93), with a small increased risk of hemorrhagic stroke (HR: 1.07; 95% CI: 0.42–2.69), but had no stroke preventive benefit in men. On the other hand for myocardial infarction, there was a 32% risk reduction in risk observed in men but no significant benefit was seen in women. The precise factors contributing to these sex-specific differential effects are unknown but presumably differences in study timing, design and characteristics likely play a role. For secondary stroke prevention and early acute ischemic stroke management, aspirin appears to confer analogous benefits in men and women [26].
Prevailing guidelines for cardiovascular prevention in women endorse aspirin therapy in doses of 75–325 mg per day for high-risk women unless contraindicated, and in women age 65 years or older, aspirin should be considered in doses of 81 mg daily or 100 mg every other day if blood pressure is controlled and the potential benefit of preventing ischemic stroke or myo cardial infarction is greater than the risk of gastrointestinal bleeding and hemorrhagic stroke [27]. In women less than 65 years of age, aspirin should be considered when the benefit for preventing ischemic stroke probably outweighs the adverse effects of treatment.
No studies to date have prospectively assessed the combined roles of endogenous estrogen and antiplatelets on stroke prevention and outcome despite evidence suggesting that endogenous estrogen levels and other sex hormones mediate antiplatelet pharmacotherapy. A meta-analysis of 18 placebo-controlled clinical antiplatelet trials found no sex differences regarding antiplatelet drugs [26]. However, sex differences with respect to aspirin including variability in absorption, bio-availability, and anti-inflammatory and antiplatelet effects have been described in the literature [28,29]. A retrospective analysis of sex-specific antiplatelet response demonstrated that in postmenopausal women taking oral aspirin as a secondary stroke-prevention measure, aspirin was less effective in inhibiting platelet aggregation in women than in men with a history of previous stroke or transient ischemic attack (TIA) [29]. However, it must be noted, that the women in this study had a higher incidence of diabetes and obesity, known risk factors. Owing to the level of platelet inhibition associated with increased risk for vascular occlusive events, a less robust response to aspirin may result in worse stroke outcome [30,31]. In turn, it is theorized that women in various menopausal states may require different doses of antiplatelets to provide adequate protection.
Sex differences have also been described in the use of antiplatelet medications in both the acute and outpatient settings. Studies from Sweden, Canada and the UK have demonstrated that fewer women than men were prescribed antiplatelet or antithrombotic therapy at discharge. No sex differences have been found in c omparable US studies [32].
While the incidence of stroke is highest amongst postmenopausal women, the etiology of stroke in premenopausal women requires intensive work-up and tailored treatment, specifically in the area of migraine and dysimmune syndromes. The increased incidence of ischemic stroke in women who experience migraine headaches when taking oral contraceptive pills who also smoke further suggests a role of estrogen in thrombus formation. Studies suggest that platelet activation and aggregation are associated with migraine in that thrombi can form and occlude cerebral microcirculation resulting in ischemia [33]. Endothelial dysfunction is also more common in women with migraine and leads to increased platelet aggregation. When associated with oral contraceptive use and smoking, there is an increased incidence of thrombus formation. However, studies have also found no interaction between migraine, reproductive status, and ischemic stroke risk [34]. Further studies are required to assess the mechanism of increased stroke risk in this patient population and target therapies to those at risk for thrombotic event. Although the current American Stroke Association guidelines for the secondary prevention of stroke do not include specific recommendations for antiplatelet use in these populations, therapy in this population should include surveillance, antiplatelet therapy and smoking cessation education.
In addition to migraineurs, increased risk of ischemic stroke has been seen in women with immune disorders such as systemic lupus erythematosus and antiphospolipid antibody (APL) syndrome. The Warfarin–Aspirin Recurrent Stroke Study (WARSS)/Antiphospholipid Antibodies and Stroke Study (APASS) collaboration compared warfarin (international normalised ratio: 1.4–2.8) with aspirin (325 mg) for the prevention of a second stroke in patients with APL antibodies [35]. No difference was found between the risk of the composite end point of death from any cause (ischemic stroke, myocardial infarction, deep vein thrombosis, pulmonary embolism and other systemic thrombo-occlusive events) in patients treated with either warfarin (RR: 0.99; 95% CI: 0.75–1.31; p = 0.94) or aspirin (RR: 0.94; 95% CI: 0.70–1.28; p = 0.71). The American Stroke Association recommends that in the case of ischemic stroke or TIA and positive APL antibodies, antiplatelet therapy is reasonable. However, for patients with ischemic stroke or TIA who meet the criteria for the APL antibody syndrome with venous and arterial occlusive disease in multiple organs, miscarriages, and livedo reticularis, oral anticoagulation with a target international normalized ratio of 2–3 is preferred [36].
Estrogen-independent sex differences in cerebral ischemia
Despite compelling evidence for a neuroprotective role of estrogen in cerebral ischemia, complete examination of sex differences requires consideration of nonestrogen related physiologic differences. Some research has suggested that the difference in physiologic and behavioral outcome in rodent models of cerebral ischemia may be owing to genetic differences in the XX and XY cell rather than sex steroid influences [37,38]. Similarly, the role of progesterone in stroke has received increased attention. Recently, progesterone was shown to suppress the inflammatory response and inducible nitric oxide synthase expression in the brain after cerebral ischemia [39,40], while others report an increase in endotoxin-mediated induction of cyclooxygenase-2 and inducible nitric oxide synthase in rat cerebral blood vessels after chronic treatment with progesterone or medroxyprogesterone [41]. The coinciding fuctuation of endogenous estrogen and progesterone during the estrous cycle also appears to modulate inflammatory responses of cerebral vessels [41]. While no studies of exogenous progesterone without estrogen have been conducted in ischemic stroke patients, a randomized study in traumatic brain injury patients has shown promise. The Progesterone for the Treatment of Acute Traumatic Brain Injury (ProTECT) study found that administration of intravenous progesterone to adult trauma patients who arrived within 11 h of injury with a Glasgow Coma Scale (GCS) score of 4–12 resulted in lower 30-day mortality rate than placebo [42]. A total of 30 days postinjury, the majority of severe traumatic brain injury survivors in both groups had relatively poor outcome; however, moderate traumatic brain injury survivors who received progesterone were more likely to have a moderate-to-good outcome than those randomized to placebo.
The ProTECT II study is currently underway to further assess the benefits of progesterone in traumatic brain injury.
No studies have assessed the effects of genetic female and male differences or progesterone in mediating acute or preventative antiplatelet therapy in ischemic stroke. These mediating effects of genetic differences as well as novel sex steroids such as progesterone must be examined to fully model sex differences in ischemic stroke risk, treatment and outcome.
Conclusion
There is growing recognition of the personal and public health relevance of stroke in women. The disease burden of stroke in women is larger than in men given that women have more stroke events and are less likely to recover from those strokes. Since women tend to outlive men, this sex disparity will probably worsen in the years to come as the population continues to age. Bridging this disparity will involve a better understanding of sex-specific issues in cerebrovascular disease, including the differential response of women to various proven pharmacologic interventions. Antiplatelet therapy is currently a cornerstone in stroke preventive treatment as well as early management of acute ischemic stroke, however there remains a major gap in the literature regarding the actual effect of estrogen and other sex hormones on the efficacy of antiplatelet drugs for patients with or at risk for stroke. Specifically, little is known regarding the interactive effects of estrogen levels, antiplatelet therapies and stroke outcome. It is conceivable that future expert consensus guidelines may comprise sex-specific recommendations on stroke management but in the meantime more studies with stroke as the primary outcome, comprising adequate representation of women, and sufficiently powered to examine sex-specific differences will need to be conducted. Ultimately, clinicians should be vigilant in ensuring that women are receiving antiplatelet medications as part of a secondary stroke prevention regimen and the choice of the ideal antiplatelet medication in women requires further research.
Executive summary
Annually, 55,000 more women than men experience stroke.
Annual stroke deaths in women are predicted to increase from 32,000 excess deaths in 2000 to nearly 68,000 by 2050.
Women are more likely to be older, have worse prestroke disability, have cardioembolic stroke etiology, present with nontraditional symptoms, and are 30% less likely to be treated with tissue plasminogen activator than men.
Preclinical evidence suggests that the female hormone estrogen mediates the effects of ischemic stroke and stroke therapy in women.
Overall risk reduction seen in men is primarily driven by the reduction in myocardial infarction, while the female risk reduction is accounted for by a 17% reduction in stroke events.
All organs require adequate blood flow to supply oxygen and nutrients for their specific tissues to function normally. If blood flow is compromised, cells suffer hypoxic injury, die, and can no longer perform their physiologic function. In the case of ischemic stroke, a thrombus disrupts normal blood flow to a part of the brain. This disruption in normal blood flow to the brain tissue leads to ischemia, neuronal injury and neuronal damage.
Endogenous estrogen (and possibly other sex hormones) play a mediating role in the ischemic process leading to neuroprotective effects.
Coagulation process has been reconceptualized as a cell-based process that functions to initiate, amplify and propagate formation of the thrombus.
Initiation phase: begins when injury to the subendothelium leads to expression of tissue factor. Occurs at the level of the tissue factor bearing cells and primarily functions to build a strong fibrin mesh network to form a stable clot.
Amplification phase: occurs on the activated surface of circulating platelets. The procoagulant properties of thrombin function as an agonist to increase platelet activation. Thrombin formed in the initiation phase activates factors Va, VIIIa, and factor XI on the platelet surface.
Propagation phase: occurs on the activated platelet surface. Final phase functions to recruit platelets to the site of vascular injury to form the platelet plug. The amount of thrombin produced at this step is responsible for producing a stable clot.
Platelet surface receptors: both platelet aggregation and thrombus formation result from activation of platelet surface receptors subsequent to activation of coagulation pathways. Each of the platelet receptors can independently activate platelet aggregation; however, activation of the platelet surface membrane glycoprotein integrin receptor is the final common pathway to platelet activation. Thromboxane A2 and ADP pathways, which occur in the amplification and propagation phase of coagulation at the platelet surface, are critical to final activation of the glycoprotein integrin receptor.
Platelets contain estrogen receptors on their surfaces, which become upregulated in the absence of estrogen, thus lowering the threshold for platelet activation and increasing the propensity to clot formation.
Rodent studies have shown that acute estrogen deficiency increases postischemic platelet reactivity and treatment with estrogen doses to physiologically premenopausal levels decreases this hypersensitivity.
A study in a rabbit model of embolic stroke has demonstrated that higher serum endogenous estrogen levels result in improved clinical outcome after acute antiplatelet loading treatment.
In the presence of postmenopausal, prepubescent endogenous estrogen levels, platelet reactivity is decreased and the affinity for platelet aggregation and thrombus formation reduced.
No studies to date have prospectively assessed the combined roles of endogenous estrogen and antiplatelets on stroke prevention and outcome.
A meta-analysis of 18 placebo-controlled clinical antiplatelet trials found no sex differences regarding antiplatelet drugs.
Reported sex differences with respect to aspirin include variability in absorption, bioavailability and anti-inflammatory and antiplatelet effects.
A retrospective analysis showed that aspirin was less effective in inhibiting platelet aggregation in postmenopausal women than in men with a history of previous stroke or transient ischemic attack.
Studies from Sweden, Canada and the UK have demonstrated that less women than men were prescribed antiplatelet or antithrombotic therapy at discharge.
No sex differences in antiplatelet use in stroke prevention have been found in comparable US studies.
It is theorized that women in various menopausal states may require different doses of antiplatelets to provide adequate protection.
Research has suggested that differences in physiologic and behavioral outcome in rodent models of cerebral ischemia may be due to genetic differences in the XX and XY cell rather than sex steroid influences.
Progesterone has been shown to suppress the inflammatory response and inducible nitric oxide synthase expression in the brain after cerebral ischemia.
No studies have assessed the effects of genetic female/male differences, progesterone or other sex hormones in mediating acute or preventative antiplatelet therapy in ischemic stroke.
Sex differences should be examined within all studies of acute stroke epidemiology, pathophysiology, treatment and outcome.
The role of bio-identical estrogens (e.g., estriol) and other sex hormones (e.g., progesterone and testosterone) should be examined for their usefulness in stroke treatment in both preclinical models and clinical studies.
Future antiplatelet preventatives may be based on endogenous sex hormone level or genetic female/male differences.
Footnotes
This work was sponsored in part by the NIH National Institute of Nursing Research Predoctoral Fellowship (1F31NR011120–01). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.