
Abstract
In this article we will describe our proposed changes to the breast cancer tumor node metastasis (TNM) classification which, while retaining TNM structure to ensure backwards compatibility, will render it more useful and better able to accommodate future developments. We propose changing T to specify exact tumor size (a tumor of pathological diameter 1.7 cm would be pT1.7); changing N to specify the number of metastatic lymph nodes over the total number removed (e.g., pN5/21); adding suffixes to M to indicate metastatic site; removing in situ neoplasms from the classification, since they are not carcinomas and are incapable of metastasizing; and removing the terms ‘infiltrating’ and ‘invasive’ since they are redundant. Finally, we would include hormone receptor, HER2, and other biological indicators of prognosis, as they are verified, in a placeholder system appended to the TNM. These proposals shift the emphasis from the quantity of tumor present to the quality of the cancer.
Keywords
The need for a unified and internationally accepted cancer staging system was recognized in the first half of the 20th century and led to the publication of the first International Union Against Cancer (UICC) [1] staging system in the late 1950s. This was followed by the International Federation of Gynecology and Obstetrics (FIGO) classification of women's cancers [2] and the first edition of the American Joint Committee for Cancer (AJCC) classification, published in 1977 [101]. These classifications consider the size of the primary (T), regional lymph node status (N) and presence of distant metastases (M) as fundamental disease characteristics that are used to assign a disease stage at diagnosis, which defines disease extent, correlates with prognosis, and at least to some extent, indicates treatments.
The AJCC and UICC cooperate in updating the tumor node metastasis (TNM) cancer classification, the 7th edition of which was published at the end of 2009 [3,4]. This new edition is notable for its use of international datasets to drive classification changes and for the marked increase in the use of nonanatomic prognostic factors for defining disease stage.
In this article we wish to represent our proposals for changing the TNM system for breast cancer [5–7] so as to render it more flexible and useful today, and better able to accommodate inevitable future developments. We believe it is important to re-present our proposals, since they were first published when the 6th TNM classification was still current and the 7th TNM classification was in the final stages of preparation, meaning it was too late for our suggestions to have been seriously considered by the revision committee.
The specific aims of our proposed TNM system are: to eliminate confusing terminology; to introduce a simple system for more precisely specifying T, N and M information (thus increasing the prognostic value of that information and rendering it more amenable to statistical elaboration); and to introduce a simple, yet flexible placeholder system, to allow the inclusion of biological data relevant to cancer staging.
Information on breast cancer biology at the molecular level is expanding rapidly and is becoming increasingly important in refining the prognosis and indicating the treatment for the disease, particularly in relation to new pharmaceutical agents. The placeholder system we propose will make it possible to add biological information to the mainly pathological information provided by the current TNM.
Language & terminology
Psychological problems are present in approximatley 20–40% of patients diagnosed with cancer [8]. Words such as ‘invasive’, ‘infiltrating’ and ‘malignant’ have a strongly negative emotive valence, conjuring up images of pain, suffering and death. The fears and uncertainty that a cancer diagnosis generates may motivate the person to put her faith in the treating physician, ask questions about the illness, and to research/refer to the Internet. However, the opposite reaction of withdrawing into oneself and experiencing the diagnosis as a death sentence, is common [9]. The way the diagnosis is communicated, by the physician or the diagnostic report, can markedly influence how the patient reacts. The terminology used by the current TNM classification can exacerbate these problems and make it more difficult for the patient to come to terms with her disease [10].
When a patient is told she has ‘carcinoma in situ’ she will usually become extremely anxious, thinking that she has an incurable cancer. The situation appears much worse for the woman who is told she has ‘infiltrating carcinoma.’ The already traumatic effect of the word carcinoma is worsened by its qualifier ‘infiltrating.’ This woman understands that, even though her illness may have been diagnosed at an early stage, it has already infiltrated her organs and will surely kill her. One consequence may be that she does not have the hope and fortitude necessary to face up to her treatment program; she asks how long she has to live; and is beside herself with the thought she will not see her children grow up.
After an interview with the physician, the patient with in situ carcinoma is reassured, learning she has ductal or lobular carcinoma in situ and that this type of disease differs biologically from infiltrating carcinoma. She also learns that she is likely to be completely cured.
The second woman – the one with infiltrating carcinoma – will also benefit from more precise information about the nature of her disease. If her cancer is small, she will learn that the prognosis is good, notwithstanding the terrifying term ‘infiltrating’ (or its alternative ‘invasive’). Infiltrating is an old pathological term referring to the situation where tumor cells breach the basal membrane of the duct or lobule.
The first innovation of TNM classification that we propose is to eliminate the inaccurate ‘in situ carcinoma’, and the emotionally charged ‘infiltrating and invasive’ and replace them with a more logical and accurate terminology [5–7].
Ductal carcinoma in situ (DCIS) and lobular carcinoma in situ (LCIS) are included within the T part of the current TNM classification. However, these neoplasms are noninvasive by definition, and are incapable of metastasizing to distant sites. They should not, therefore, be considered either malignant or carcinoma, and should be excluded from the TNM classification. We propose adopting the classification of Tavassoli [11], which disregards the terms DCIS and LCIS and instead replaces them with ductal intraepithelial neoplasia (DIN) and lobular intraepithelial neoplasia (LIN)
TNM breast staging comparison guide: 6th International Union Against Cancer versus Tavassoli classification (primary tumor).

DCIS: Ductal carcinoma in situ; LCIS: Lobular carcinoma in situ; pTis: In situ tumor; TNM: Tumor nodal metastasis; UICC: International Union Against Cancer.
With regard to ‘infiltrating’ and ‘invasive’, it is clear that these terms are redundant, particularly in the phrases of infiltrating carcinoma and invasive carcinoma, carcinoma is by definition infiltrating or invasive. Therefore, we also propose removing these terms, with their terrifying connotations, from the TNM classification.
New definition of T
The second major innovation proposed by our TNM classification is to specify T and N more precisely, with the advantage of furnishing a more exact and useful indication of ‘disease stage’ and at the same time retaining compatibility with the older T and N categories, hence permitting statistical comparisons between older data and new data.
Let us consider T first: we wish to abolish the T categories of the current TNM classification and replace them by the exact specification of tumor size in cm
TNM breast staging comparison guide: 6th International Union Against Cancer versus TNMIEO (primary tumor).
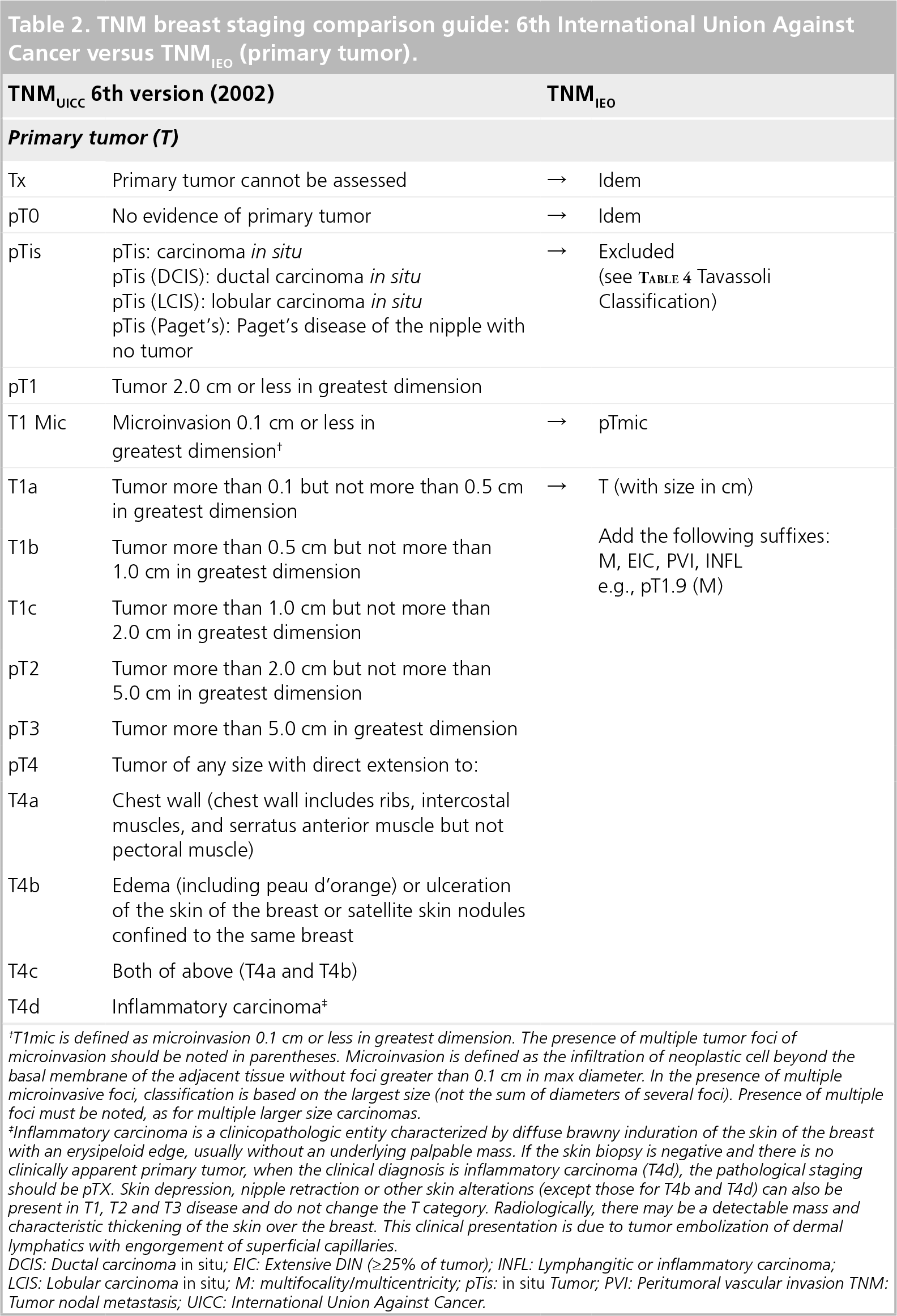
T1mic is defined as microinvasion 0.1 cm or less in greatest dimension. The presence of multiple tumor foci of microinvasion should be noted in parentheses. Microinvasion is defined as the infiltration of neoplastic cell beyond the basal membrane of the adjacent tissue without foci greater than 0.1 cm in max diameter. In the presence of multiple microinvasive foci, classification is based on the largest size (not the sum of diameters of several foci). Presence of multiple foci must be noted, as for multiple larger size carcinomas.
Inflammatory carcinoma is a clinicopathologic entity characterized by diffuse brawny induration of the skin of the breast with an erysipeloid edge, usually without an underlying palpable mass. If the skin biopsy is negative and there is no clinically apparent primary tumor, when the clinical diagnosis is inflammatory carcinoma (T4d), the pathological staging should be pTX. Skin depression, nipple retraction or other skin alterations (except those for T4b and T4d) can also be present in T1, T2 and T3 disease and do not change the T category. Radiologically, there may be a detectable mass and characteristic thickening of the skin over the breast. This clinical presentation is due to tumor embolization of dermal lymphatics with engorgement of superficial capillaries.
DCIS: Ductal carcinoma in situ; EIC: Extensive DIN (≥25% of tumor); INFL: Lymphangitic or inflammatory carcinoma; LCIS: Lobular carcinoma in situ; M: multifocality/multicentricity; pTis: in situ Tumor; PVI: Peritumoral vascular invasion TNM: Tumor nodal metastasis; UICC: International Union Against Cancer.
Thus, a tumor with a maximum diameter of 1.7 cm on pathological examination, would be pT1.7 and not pT1c. The result is a more intuitively comprehensible and information-rich characterization, with no increase in complexity.
The current T categories are a throwback to the situation when the first TNM classifications were developed 70 years ago. At that time it was only possible to diagnose a breast cancer large enough to be palpated. (In Italy surgeons then talked about ‘cherry sized’ lumps or depressingly often, ‘apricot’ or ‘apple’ sized masses.)
Today, however, the lack of logic in T categories is evident, because they do not make full use of the information provided by modern diagnostic methods, which allow the identification of tumors much smaller than cherry sized. The T1 category ranges from a few mm to 2 cm, with a large difference in prognosis between extremes. These differences in prognosis are in part acknowledged by the T1 subcategories (T1a, 1–5 mm; T1b, 6–10 mm; and T1c, 11–20 mm), but these are essentially arbitrary and needlessly complex.
The prognostic variation within T2, which includes cancers from 2.1 to 5 cm, is even more marked. A tumor of diameter 2.1 cm has a volume of 4.5 ml (assuming it were spherical) while a 5 cm cancer has a volume of approximately 60 ml. The difference in prognosis between the two masses is marked.
It is clear that other pathological characteristics of the cancer have an influence on prognosis, including extensive intraductal component, perivascular invasion and multifocality. We therefore propose adding prognostically important suffixes such as eic (extensive intraductal component), pvi (perivascular invasion), m (multifocal) and inf (inflammatory) to the new T specification, which provide new information without compromising comprehensibility to either patient or clinician (e.g. pT1.5EIC or pT0.7PVI).
New definition of N
The classification of axillary lymph node involvement we propose follows the logic of our new T classification: it specifies the exact number of lymph nodes found to be metastatic over the total number removed; for example, pN5/21 states that five of the 21 lymph nodes examined were metastatic. Consider the utility of this: if three nodes of the 28 axillary lymph nodes removed and examined were positive, the current N stage would be N1b, but in our system it be simply pN3/28.
Over the last 15 years, sentinel node biopsy has completely revolutionized the approach to the axilla in breast cancer [12]. This revolution has been felt in the current TNM classification, but the modification we propose is simply to add sentinel node (SN). Thus: pN0/1SN
TNM breast staging comparison guide: 6th International Union Against Cancer versus TNMIEO regional lymph nodes (in situ).

The regional lymph nodes are: axillary (ipsilateral): interpectoral lymph nodes (Rotter's node) and lymph nodes along the axillary vein and its tributaries, which may be divided into the following three levels:
Level 1 (lower axilla): lymph nodes lateral to the lateral margin of the pectoralis minor
Level 2 (middle axilla): lymph nodes between the medial and lateral margins pectoralis minor and interpectoral lymph nodes (Rotter's nodes)
Level 2 (apex of the axilla): lymph nodes medial to the medial margin of pectoralis minor including those known as subclavicular, infraclavicular or apical.
Note: intramammary lymph nodes are considered axillary lymph nodes
– Ipsilateral infraclavicular (subclavicular)
– Mammary internal (ipsilateral): are situated in the intercostal space along the lateral edge of the sternum on the endothoracic fascia
– Supraclavicular (ipsilateral).
Classification is based on axillary lymph node dissection with or without sentinel lymph node dissection. Classification based solely on sentinel lymph node dissection without subsequent axillary lymph node dissection is designated (sn) for ‘sentinel node,’ e.g., pN0(i+)(sn).
Cases with only ITCs in regional lymph nodes are classified pN0. ITCs are defined as individual tumor cells or small cell clusters not greater than 0.2 mm, usually detected only by IHC or molecular methods but which may be verified on H&E stains. ITCs do not usually show evidence of metastatic activity (e.g., proliferation or stromal reaction).
RT-PCR.
If associated with greater than three positive axillary lymph nodes, the internal mammary nodes are classified as pN3b to reflect increased tumor burden.
Not clinically apparent is defined as not detected by imaging studies (excluding lymphoscintigraphy) or by clinical examination.
Clinically apparent is defined as detected by imaging studies (excluding lymphoscintigraphy) or by clinical examination or grossly visible pathologically. BLN: bunched lymph nodes; EXCP: Extracapsular invasion; IHC: Immunohistochemical; ITC: Isolated tumor cell; RT-PCR: Reverse transcriptase PCR; SN: Sentinel node; TNM: Tumor nodal metastasis; x: Number of pathological lymph nodes; y: Number of lymph nodes removed.
Sentinel node biopsy combined with more exhaustive pathological examination (sections every 50 μm) [13] has led to the frequent finding of micrometastases (<2 mm) or even of small clusters of cancer cells (isolated tumor cells). The current TNM classification designates these as NMIC and NITC – categories, which were used, for example, in trial 23/01 [13]. We also propose using the suffix isolated tumor cells (ITCs)
Distant metastases (M)
The current TNM classification uses M1 to indicate the presence of distant metastasis. However, we feel it is important to specify the site of distant disease spread, since different sites can be treated with different levels of success using new treatment modalities such as radiofrequency thermoablation [15], stereotactic radiosurgery (γ knife) [16], high-intensity focused ultrasound [17] and monoclonal antibodies [18,19]. We propose using suffixes to indicate the metastatic sites; for example pM1pul (metastases to lung) and pM1oss (metastases to bone).
TNM breast staging comparison guide: 6th UICC versus TNMIEO distant metastasis.

IEO: European Institue of Oncology; M: Metastases; TNM: Tumor nodal metastasis; UICC: International Union Against Cancer.
Biological factors
As the molecular and genetic understanding of breast cancer has increased, new biological characteristics have been identified as prognostic indicators, and new adjuvant treatments have been developed [20]. This has resulted in an increasingly personalized approach to breast cancer treatment that takes into account the diverse biological characteristics of the individual and their disease.
At present, estrogen and progesterone receptor status and HER2 overexpression, are the main biological variables used to provide an indication of the prognosis for breast cancer. However numerous factors can compromise these assays, giving rise to false-positive or false-negative results. These include imperfect fixation (the optimal fixative for breast cancer tissue is neutral buffered formalin; the optimal time varies from 6 to 48 h), incorrect choice of antibodies, inadequate antigen reactivation and errors in interpreting the results. It is important, therefore, that the assays are performed with care and according to internationally recognized standards and are interpreted by an experienced pathologist. It is also important that the pathology laboratory participates in quality control programs to check adherence to international standards and that the pathologist is actively involved in the interdisciplinary discussion of the therapy (particularly systemic therapy), to be given to each patient.
HER2 (also known as neu or erbB2) is overexpressed in approximately 20–30% of breast cancers, usually because gene duplication events increase the number of copies of the HER2 gene in each cancer cell. HER2 overexpression indicates an aggressive type of breast cancer, and the monoclonal antibody drug trastuzumab is able to inactivate HER2 and improve the prognosis for this type of breast cancer [21].
The way HER2 expression is measured in breast cancer samples can influence the indication for trastuzumab use. HER2 expression is most often assessed immunohistochemically (IHC), assigning a score of 0 to +3 according to the intensity and completeness of staining on the cancer cell membrane [22,23]. The second method, typically used if the IHC result is uncertain, employs fluorescent N hybridization (FISH) to estimate the number of copies of the HER2 gene per cancer cell. The HER2 gene is present on the long arm of chromosome 17 (17q21-q22) and the HER2 gene copy number is usually expressed relative to chromosome 17. Unfortunately, notwithstanding efforts to introduce a standardized and reliable HER2 assay method, the result may sometimes be uncertain, introducing uncertainties in the indication for trastuzumab use [23,24]. In the future, gene expression may prove a more robust way of identifying ER and HER2 expression [25].
We propose introducing ER, PgR, Ki-67 and HER2 status into the new TNM classification. For HER2, we would specify not only the IHC score (indication of percentage of cancer cells with highly positive staining), but also the result of the FISH analysis, if performed, specifying the amplification/nonamplification/polysomy of chromosome 17 and would also include the absolute or relative number of copies of the HER2 gene [26].
We also know that ER-positive lobular and ductal carcinomas can be of the luminal A or luminal B type based on gene expression profile [27]. Luminal B types have a worse prognosis than luminal A types, while the basal-like (triple negative) type has an even worse prognosis, irrespective of nodal status or tumor size [26,28]. We expect that subtypes characterized by gene expression profiles (as well as other factors such as p95 status, for example) will eventually need to be incorporated into the classification [27], athough those defined by Perou et al. are likely to undergo modification [29].
Cancer stem cells in a future TNM?
Intense research is currently being conducted to determine the role of cancer stems cells in cancer spread in the hope of refining prognosis and improving treatment. According to the cancer stem cell theory, a small number of cancer stems cells are present in most tumors [30]. These are relatively slow growing and divide asymmetrically to produce more self-renewing stem cells, but mainly the quickly dividing cells that form the mass of the tumor. Although these latter cells are variably differentiated they do not possess metastatic potential. According to this view, the cells in a cancer are hierarchically organized, as in normal tissue and the carcinogenetic process can be regarded as organogenesis gone wrong. The quantity of stems cells and their detailed properties are likely to vary between one cancer and another, accounting for differences in expansion kinetics. It has been suggested, for example, that the basal-like type of breast cancer has an elevated number of cancer stem cells [30,31] and may have greater metastatic potential, since cells shed from the primary tumor would be more likely to be stem cells. If histological markers of cancer stems cells can be found, the development of specific drugs to target and destroy them would also be feasible and we would then think of incorporating the characteristics of a tumor's stem cells into a future TNM classification.
Conclusion
Notwithstanding the fact that the latest extensively revised TNM classification was only published in December 2009 [3,4], we believe that further changes are necessary to the breast cancer TNM in order to accommodate the rapidly expanding knowledge of the disease. The changes we propose are radical: not only modifications to the specification of T, N and M – to reflect the more precise pathological characterization of tumors, which is routine today and new possibilities for treating metastatic disease – but also the addition of placeholders to specify the cellular and molecular characteristics of the tumor that are important for prognosis and treatment. The placeholder system will render the TNM classification flexible enough to accommodate new information about prognostic indicators for breast cancer, including gene expression profiles, as they are validated. Our proposals amount to a major shift of emphasis from the quantity of tumor present (main concern of the current TNM classification) to the quality of the cancer (as specified by biological and biomolecular characteristics) explicitly recognizing that breast cancer is a highly heterogeneous disease whose prognosis depends on the individual characteristics of each disease type. Finally, but of no less importance, we propose tidying up TNM terminology so that it is more rigorous and is less likely to increase psychological distress in the newly diagnosed patient.
Future perspective
The TNM (tumor, regional lymph node, metastasis) classification of cancer was developed in the second half in of the 20th century using mainly anatomical/pathological data to define disease stages of differing prognoses. The classification has developed continuously and the latest seventh edition, published in December 2009, is notable for the wide use of nonanatomic prognostic factors to define disease stage. However, as the pace of scientific discovery quickens and molecular characteristics (including gene profiles) are increasingly used to define prognosis and indicate treatment, we believe the TNM classification of breast cancer should be made ready to accommodate these advances. We propose major changes to the TNM classification of breast cancer so that it remains compatible with the old system, but provides more precise pathological information and is predisposed to accommodate new prognostic factors as they are validated.
Executive summary
We propose changing tumor node metastasis (TNM) for breast cancer to enhance its prognostic utility, rendering it more useful today and better able to accommodate future developments.
In situ carcinomas should be removed from the TNM system and classified separately as various grades of ductal and lobular intraepithelial neoplasia (DIN and LIN, respectively).
The terms ‘infiltrating’ and ‘invasive’ should be abolished as qualifiers of ‘carcinoma’.
T should specify exact tumor size: a tumor of 1.7 cm on pathological examination would be pT1.7.
Extensive intraductal component, perivascular invasion, multifocality and inflammatory disease should be specified as suffixes to T; for example, pT1.7eic.
N should specify the exact number of metastatic lymph nodes over the total number removed: for example, pN5/21 indicates that five of the 21 examined nodes were metastatic; pN/2sn-itc indicates that sentinel nodes contain isolated tumor cells only.
M should indicate the metastatic site; for example, M1oss indicates bone metastases.
Hormone and HER2 status should be specified using a placeholder system.
The same placeholder system could be expanded to include the status of biological/molecular biological prognostic factors as they are validated.
A future TNM might include an assessment of the cancer stem cells present in the tumor if these were shown to have prognostic significance.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
The authors thank Don Ward for help with the English, who was paid for his services by the European Institute of Oncology.