
Abstract
Hypoactive Sexual Desire Disorder (HSDD) is the most common female sexual dysfunction. The diagnosis of HSDD requires the existence of personal distress or interpersonal difficulties associated with low sexual desire, that cannot be explained by any other psychiatric affection and that is not exclusively due to a disease or substance. HSDD can have a serious effect on emotional wellbeing and interpersonal relationships, and it occurs in premenopausal and postmenopausal women. The Decreased Sexual Desire Screener is a shortened diagnostic method designed to help doctors who are not specialized in female sexual dysfunction to diagnose acquired HSDD in women. There is evidence that treatment with androgens or with estrogens is effective in HSDD; however, important unanswered questions still exist. Presently, new therapeutic strategies to combat HSDD are being researched, including novel methods of testosterone provision and drugs that act upon the CNS.
Keywords
 : Continuing Medical Education Online
: Continuing Medical Education Online
This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Medscape, LLC and Future Medicine Ltd. Medscape, LLC is accredited by the ACCME to provide continuing medical education for physicians.
Medscape, LLC designates this Journal-based CME for a maximum of
All other clinicians completing this activity will be issued a certificate of participation. To participate in this journal CME activity: (1) review the learning objectives and author disclosures; (2) study the education content; (3) take the post-test and/or complete the evaluation at www.medscapecme.com/journal/wh; (4) view/print certificate.
Learning objectives
Upon completion of this activity, participants should be able to:
Describe the epidemiology of HSDD
Evaluate risk factors for HSDD
Diagnose HSDD effectively
Analyze treatment options for HSDD
Female sexual dysfunction (FSD) involves a group of sexual problems experienced by women; among these are low desire or motivation to engage in sexual activity, a reduction in vaginal lubrication or arousal, a decreased ability to achieve orgasm and sexual pain [1]. In order to accurately diagnose FSD, the sexual problem has to cause personal distress or difficulties in interpersonal relationships [1]. Sexual disorders were recognized in the Diagnostic and Statistical Manual of Mental Disorders of the American Psychiatric Association, second Edition (DSM-II) [2] in 1968, although the term sexual disorder was not used until 1987 (DSM-III-R) [3]. Since then, sufficient progress in understanding FSDs has been made. The International Consensus Development Conference on Female Sexual Dysfunction gave rise to the Consensus-based Classification of Female Sexual Dysfunction in 1998 [4]. These FSD definitions, revised in 2004 [5], establish a difference between those disorders that have an effect on the principal elements of sexual response: desire, arousal and orgasm, and those that include intercourse-related pain. The Diagnostic and Statistical Manual of Mental Disorders of the American Psychiatric Association, 4th Edition, Text Revision (DSM-IV-TR 2000) [1] recognizes the existence of various types of sexual activity disorders in women, including Sexual Desire Disorders (Hypoactive Sexual Desire Disorder [HSDD] and sexual aversion disorder), female anorgasmia, female sexual arousal disorder and sexual pain disorders. It is quite difficult in practice to differentiate desire and excitement and in the future it is probable that these will no longer be classified separately.
This article aims to offer a present-day overview of the physiopathology, tools, diagnostic treatments and the treatment of HSDD by means of a review of the most important articles on the topic.
What is HSDD?
In 1968, a group of experts on the International Consensus on Female Sexual Health suggested that the definition of HSDD should be amplified to include the lack (or absence) of receptiveness to sexual activity given that sexual desire in some women is especially provoked more than it is spontaneous. The DSM-IV-TR 2000 recognized HSDD as a persistent or recurrent lack (or absence) of sexual fantasies and desire for sexual activity that causes marked distress or difficulty in interpersonal relationships and is not caused exclusively by another psychiatric disease, affectation or substance, for example, medications [1]. HSDD may or may not be associated with another physical or mental illness [1,6]. Upon diagnosis, the doctor should determine whether the disorder is life long or acquired (e.g., if the disorder has existed since the onset of sexual activity or if it has developed after a period of normal activity). One should also take into account whether the disorder is generalized or situational (e.g., whether or not it is limited to specific types of stimulation, situations or partners) [1].
Epidemiology of HSDD
In 1998, the International Consensus Group calculated that FSD affects over 20% of all women [4]. A cross-sectional survey of women from the USA and Europe (Women's International Study of Health and Sexuality (WISHeS) evaluated the prevalence of HSDD [7,8]. The European sample consisted of 2467 women aged between 20 and 70 years from France, Germany, Italy and the UK. In women aged between 20 and 49 years, the prevalence of HSDD (defined as the decrease in desire linked to distress) was 6% in premenopausal women and 16% in women with surgical menopause. In women aged between 50 and 70 years, the prevalence was 9% for women with natural menopause and 12% in women who had undergone surgical menopause [7]. The proportion of women with low desire increased with age whilst the proportion of women distressed about their low desire decreased with age.
The Prevalence and Correlates of Female Sexual Disorders and Determinants of Treatment Seeking (PRESIDE) study appraised the prevalence of sexual problems and distress derived from sexual relations in 31,581 women aged between 18 and 102 years in the USA [6]. The prevalence of a decrease in desire associated with distress was 8.9% in women aged between 18 and 44 years, 12.3% in women aged between 45 and 64 years and 7.4% in women aged 65 years or older. After adjusting the cross section for age in women in the USA, the prevalence of HSDD was 9.5% [6].
Women who suffer from HSDD may have problems at the time of initiating or maintaining stable sexual relations, feel unsatisfied and have problems with their partners. The studies have demonstrated that women with FSD (little desire, little arousal or sexual pain) clearly associate this with negative feelings in relation to their physical and emotional satisfaction much more negatively than those women with a normal sex life [7,9]. During a study conducted on 1042 women with symptoms of HSDD in Germany, Italy and the USA, a link was found between the reduction in desire and the increase in negative attitudes towards sexual interactions (caresses, talking about sexual relations) as much as towards nonsexual ones (talking about feelings, sharing daily tasks) [10].
Factors that affect sexual desire
There are a number of physiological, psychological and sociological factors that can affect sexual desire. Problems related to the couple and the dynamics of the relationship contribute to sexual dysfunction [11]. The association between sexual activity, factors related to the couple, such as the ability to communicate with their partner and the length of the relationship, were evaluated in an Australian survey conducted on 356 randomly selected women aged between 20 and 70 years [12]. The study demonstrated that women who were not depressed and who could better communicate their sexual needs to their partners, had a lower probability of experiencing any type of sexual affection. Women who said they were more satisfied with their relationships, as well as those who placed more importance on sex, were shown to have a lower probability of experiencing low desire. Women who were in a relationship lasting 20–29 years had a greater probability of experiencing a reduction in their sexual desire than those who had a relationship lasting under 5 years [12].
Physiological factors such as age and menopause can also exert an effect on sexual desire [6,7,9]. A secondary analysis in patients that participated in the WISHeS study showed that the proportion of women whose desire diminished, rose with age; meanwhile, the proportion of women affected by the diminishing of their sexual desire lowered with age [13]. The epidemiological data demonstrate as well that worrisome lowering of sexual desire is found to be directly related to such medical affections as depression, thyroid problems and to women reporting urinary incontinence [6,14]. There are also a few drugs associated with the diminishment of sexual desire, such as selective serotonin reuptake inhibitors that are usually prescribed for depression [15].
Sexual function has a significant global decline during pregnancy, particularly in the third trimester, and this persists for 3–6 months following delivery. The lack of adequate information, breast-feeding, dyspareunia and postpartum pelvic floor dysfunction were reported as possible causes [16].
Physiopathology of HSDD
The role of sexual hormones
Sexual hormones interact with neurotransmitters in the CNS, where the equilibrium between excitatory and inhibitory factors can control sexual functioning [17,18]. It has been confirmed that HSDD is due to disequilibrium between these excitatory and inhibitory factors.
In women, sexual stimulation provokes the liberation of vasoactive neurotransmitters such as nitric oxide (NO), in the female genitals. In addition to the local liberation of NO, it is postulated that the CNS and the spinal reflexes that control sexual response could be involved in the nitrergic neurotransmission. NO activates the soluble guanylate cyclase that stimulates the formation of cyclic guanosine monophosphate (cGMP). The physiological effects of the increase in the concentration of cGMP underlies the local excitation response observed during sexual stimulation. It is thought that not only estrogens, but also testosterone can promote the expression of NO synthetase [19,20]. Therefore, given that the production of cGMP is, to a great degree, a product of the NO synthetase expression, women require a minimum level of testosterone and estradiol to maximize their sexual response [21].
Levels of estrogens less than 50 pg/ml, are related to alterations in genital sensation and low vaginal lubrication, the result of which is an objective response, so it is necessary to ensure that the minimum levels of estradiol are above this amount [22].
Today, the therapeutic role of estrogens in the prevention and treatment of vaginal atrophy and that of androgens in sexual desire is well established, both playing an important role in arousal and orgasm, although it is a less well-studied topic and has no evidence-based protocols.
Role of neurotransmitters
Dopamine and serotonin, both neurotransmitters, are important to sexuality [23]. Dopamine carries out an essential function in the modulation of sexual desire [24]. It appears to augment sexual desire, the subjective sensation of arousal and the desire to continue sexual activity once the stimulation has begun [24]. On the contrary, serotonin signaling appears principally to carry out an inhibitor effect on sexual performance [23]. Although this negative feedback may be important during resolution (the period posterior to orgasm during which the body returns to its normal, prearousal state), an excessive or chronic serotonergic neurotransmission may reduce sexual desire. Other signaling factors that affect sexuality are norepinefrin and oxytocin, with qualities of excitation [25], and prolactin and opioids, with qualities of inhibition [26,27].
Diagnosis of HSDD
Until recently, a precise diagnosis of HSDD relied upon a medical specialist in female sexual disorders to carry out an over-lengthy exam. Several diagnostic tools have been developed to help identify the disorder during normal medical visits. The short test for HSDD was established to identify this disorder at the primary care level for postmenopausal women who present a decrease in sexual desire [28]. The Brief Profile of Female Sexual Function was also devised for use in post-menopausal women for the purpose of determining whether it could be useful to undergo a clinical examination for HSDD [29]. The Decreased Sexual Desire Screener (DSDS) is a new, short diagnostic method for acquired HSDD that can be used in women before and after menopause. It allows doctors who are not specialized in FSD to diagnose acquired HSDD [30]. The DSDS consists of five questions
It should be mentioned that DSDS is an abbreviated diagnostic method created for doctors and is not a test that women take on their own. An affirmative response in any of the parts of the fifth question (i.e., the factors that the woman believes contribute to her loss of desire) does not exclude the possibility of carrying out a diagnostic exam for HSDD. Any affirmative response in any parts of the question about all the factors that the woman feels may be contributing to her current decrease in sexual desire or interest
Recent studies have demonstrated the validity of DSDS [30–32]. A multicenter, prospective validation without treatment study performed in North America, in which 263 women participated, compared the acquired HSDD diagnoses carried out by a nonspecialist doctor who decided if it was necessary to perform a diagnostic exam for acquired HSDD. Afterwards, the participants carried out an extensive diagnostic exam with a specialist doctor and both diagnoses were then compared. The DSDS showed a diagnostic precision of 85.2% and the sensibility and specificity of the test were 83.6 and 87.8%, respectively [30].
The sensibility of the DSDS was confirmed in the test period of a randomized withholding of treatment study in North America that utilized a methodology similar to that of the validation without treatment study and showed that DSDS has a sensibility of 94.6% [31]. In the evaluation phase of a randomized treatment trial performed in 13 European countries, with placebo as the control, the sensibility was shown to be 95.6% [32]. These studies demonstrate that DSDS can be used by doctors who are not specialists in female sexual disorders in order to diagnose an acquired HSDD.
Given that the etiology of HSDD is multi-factorial, the therapeutic approach depends on the possible causes. The sexual counseling for the couple and the lifestyle ground rules should always be basic. In many circumstances, psychosexual counseling is necessary. In all cases in which a hormone deficiency is suspected, the administration of androgens, alone or in combination with estrogens is recommended. Finally, comorbidity needs to be taken into account, since it is a frequent cause of HSDD
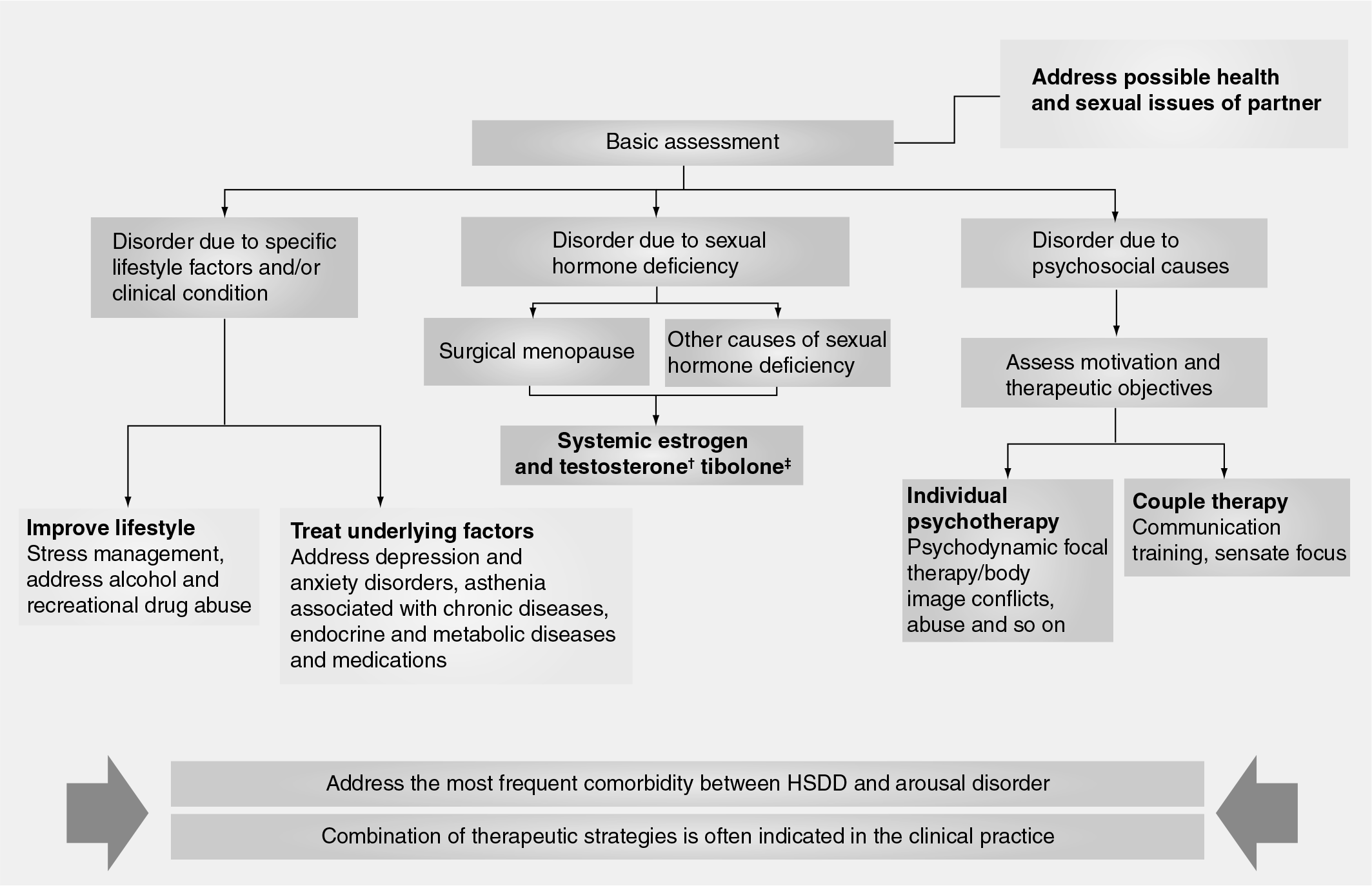
Therapeutic management of Hypoactive Sexual Desire Disorder.
Pharmacotherapy of HSDD
Cognitive behavior therapy
Although this section concerns pharmacotherapy, cognitive behavior therapy (CBT) may be useful in some women who suffer from HSDD [34,35]. In an Australian study, couples who suffered from sexual dysfunction participated in a program comprised of 10 CBT sessions; the percentage of women who suffered from an inhibition of desire was 79.6% before therapy and 53.7% after [34]. A Canadian study investigated the effect of CBT in couples where the woman suffered from HSDD. The couples participated in 12 weekly sessions consisting of 2 h of group therapy, which led to an improvement in the variables associated with sexual, cognitive and conjugal conduct; 31% of the women thought that they no longer suffered from symptoms after 3 months of therapy, and that percentage rose to 38% after 1 year of treatment [35].
Androgen therapy
Over the last 50 years, the concept of the fundamental role of androgens in the maintenance of a good sexual response in women has become clear in the medical world. Nevertheless, although works have been published [36], they were few in number, consisted of a small number of patients and often using supraphysiological doses of androgens, so that it was not possible, on the one hand, to offer any recommendations founded in medicine and based on evidence and on the other hand, there was the opinion that there were important side effects.
It was not until the start of this century, that high-quality studies began to appear [37], that the attention paid to this semi-forgotten female dysfunction began to take off. In 2002, a group of experts developed a consensus about female androgen insufficiency, defining it and making a classification, increasing its value [38]. That notwithstanding, 4 years after this consensus, the (North American) Endocrine Society published a guide [39] that devalued the consensus on the existence of an androgen deficiency syndrome in women, pointing out the methodological deficiencies that existed for determining the small quantities of androgens in women's serum, aside from the lack of homogeneity in the methods and results of the different articles published, and ending with the necessity of having more data before confirming a diagnosis and treating these women.
This publication caused different scientific societies and groups to offer their opinions [40], coinciding with various publications of well-developed studies, and for the first time, a European health agency – European Medicines Agency (EMA) – approved an androgen for hypoactive sexual desire in women [101].
Androgen levels in women
Circulating levels of androgens in women arise from the ovaries, from the suprarenal gland, and from the peripheral conversion of androstenedione and dehydroepiandrosterone (DHEA) in testosterone. The most important androgens are testosterone, dehydrotestosterone, androstenedione DHEA and DHEA sulfate.
With respect to circulating testosterone, one-third comes from the ovary and the remaining two-thirds come from the peripheral conversion of other androgens. The suprarenals do not directly produce testosterone, but one could say that by adding up the direct production and the indirect production through precursors, the ovary provides 50% of the circulating testosterone.
The ovaries of postmenopausal women continue to produce and secrete testosterone. Judd
Average levels of hormones in plasma in pre- and post-menopausal women.

Detection threshold for the study: 20 pg/ml.
1 ng/dl = 10 pg/ml.
Androgens are present at circulation levels superior to those for estradiol. Androgen levels drop more acutely after the surgery. After menopause, the levels of androgens decrease by 50% in comparison to levels before menopause. DHEA: Dehydroepiandrosterone. Modified from [42].
Only 10% of the circulating testosterone is free; the majority of it is found bound to the sexual hormone transporter protein (sex hormone-binding globulin: 66%) or to albumin (33%) [43]. Everything that affects sex hormone-binding globulin influences the free testosterone levels.
Total testosterone, free testosterone, DHEA sulfate and androstenedione lower slightly with age; this lowering being greater in the first decades than in the last. When levels of androgens are analyzed in women aged between 45 and 54 years, no menopause-specific effect on these levels was observed [44].
The circulating testosterone levels are also altered by certain diseases and the intake of drugs
The Decreased Sexual Desire Screener (DSDS) used in the nontreatment validation study
In the past was your level of sexual desire or interest good and satisfying to you?
Has there been a decrease in your level of sexual desire or interest?
Are you bothered by your decreased level of sexual desire or interest?
Would you like your level of sexual desire or interest to increase?
Please check all the factors that you feel may be contributing to your current decrease in sexual desire or interest:
– An operation, depression, injuries or other medical condition
– Medication, drugs or alcohol you are currently taking
– Pregnancy, recent childbirth, menopausal symptoms
– Other sexual issues you may be having (pain, decreased arousal or orgasm)
– Your partner's sexual problems
– Dissatisfaction with your relationship or partner
– Stress or fatigue
Verify with the patient each of the answers she has given
The Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision, characterizes HSDD as a deficiency or absence of sexual fantasies and desire for sexual activity, which causes marked distress or interpersonal difficulty and which is not better accounted for by a medical, substance-related, psychiatric or other sexual conditions. HSDD can be either generalized (not limited to certain types of stimulation, situations or partners) or situational, and can be either acquired (develops only after a period of normal functioning) or lifelong
If the patient answers ‘NO’ to any of the questions 1 through 4, then she does not qualify for the diagnosis of generalized acquired HSDD
If the patient answers ‘YES’ to all of the questions 1 through to 4, and your review confirms ‘NO’ answers to all of the factors in question 5, then she does qualify for the diagnosis of generalized acquired HSDD
If the patient answers ‘YES’ to all of the questions 1 through to 4 and ‘YES’ to any of the factors in question 5, then decide if the answers to question 5 indicate a primary diagnosis other than generalized acquired HSDD. Comorbid conditions, such as arousal or orgasmic disorder, do not rule out a concurrent diagnosis of HSDD
Based on the above, does the patient have generalized acquired HSDD?
DHEA
Men, like women, undergo a physiological lowering of the production of DHEA of up to 70% [44,46]. The testosterone derives, in part, from the peripheral conversion of DHEA and its sulfate (androgenic precursors produced by the suprarenal gland). The evolution of the role of the DHEA supplement has been analyzed in a study in patients with suprarenal insufficiency and low levels of DHEA [37]. In this randomized double blind study in 24 patients, DHEA clearly improved the visual analog scale of sexuality. Nevertheless, few data exist from studies and are contradictory.
Oral testosterone
In a recent randomized study conducted in 218 postmenopausal patients, with either natural or surgical menopause who received 0.625 μg of esterified estrogens (EE) daily, the addition of 1.25 mg of methyltestosterone (MT) improved both sexual response, as well as desire [47]. However, the two greatest concerns from this study are that women with natural menopause receive estrogens and androgens, but not gestagens and, that orally administered MT reduced the levels of high-density lipoprotein cholesterol.
Transdermal testosterone
The Intrinsa® testosterone patch is the only approved pharmaceutical treatment for HSDD in Europe, authorized for women who have undergone a bilateral ovariectomy or a hysterectomy and who follow a simultaneous estrogen treatment [101].
At present there are more than six randomized, placebo controlled trials underway (two Phase II studies and another four Phase III studies). In four of the studies, all patients had surgical menopause, and the efficacy and security of a patch that released 300 μg of testosterone daily in patients with HSDD [48–51]. All patients were treated with estrogens. In short, the women who received testosterone recounted 1.9, almost double the number of satisfying sexual relations per month, which is clearly superior to the 0.9 episodes for the placebo group. The different results on the questionnaires demonstrates a significant increase in sexual desire and sexual response and in three of the four studies the responses to the questionnaires reflected a significant reduction in the preoccupation about the problem of sexual dysfunction [49].
The efficacy and security of the testosterone patch for the treatment of HSDD in women with natural menopause receiving estrogens was also analyzed [52]. The results were very similar to those obtained for surgical menopause, leading to the conclusion that short-term treatment with patches that release 300 μg of testosterone daily in these women was well tolerated and significantly improved sexual activity and desire, and decreased preoccupation compared with placebo.
Results have been published recently on the effects of the transdermal testosterone patch in women with HSDD who were not treated with estrogens [53], noting that 300 μg of testosterone daily incremented the satisfying sexual episodes by 2.1 episodes per 4-week period, in comparison with 0.7 episodes in the placebo group (p > 0.001), with there being an increase in hair growth of 7% in the treated group compared with that with placebo (30 vs 23.1%).
Causes for a decrease in testosterone levels
Age
Oophorectomy
Hypothalamic insufficiency
Hypopituitarism
Suprarenal insufficiency
Glucocorticoid therapy
Estrogen therapy
Hyperthyroidism
Depression
Cancer
Side effects
Cardiovascular disease
The randomized studies either have not had cardiovascular disease as an objective of analysis or have not had a sufficiently long duration to be able to draw concrete conclusions.
There is a prospective study lasting 19 years [54] in which the levels of androgen in serum and the risk of cardiovascular death or ischemic heart disease are analyzed, and no relation was found between the levels and cardiovascular death. However, data from postmarketing surveillance on the combination of oral esterified estrogens and MT did not find a relationship between taking androgens and cardiovascular risk in women [55].
Blood pressure & lipids
The results of cardiovascular risk markers are:
Blood pressure: in none of the clinical trials, either with oral MT or with testosterone implants or patches, was an increase in blood pressure found [48–53].
The effect of exogenous testosterone on lipids depends on the dose, on whether it is used with estrogens or with estrogens and progestagens and the means of administration. In the studies with MT and oral estrogens, total cholesterol increased and high density lipoprotein cholesterol decreased by approximately 26% [55].
Other markers: no significant changes were found in insulin resistance, in viscosity or the coagulation factors. The data also did not point to an increase in hemoglobin above physiological levels. Nevertheless, more studies are needed, especially those analyzing physiological doses and those condcuted over a longer time period [48–53].
Effects on the endometrium
Definitive conclusions cannot be made given that the studies were either short term or that testosterone was combined with estrogens or with estrogens and progestagens. Androgens do not stimulate the endometrium cells [56], but theoretically endometrial cancer cells could convert androgens into estrogens and increase their activity since they have aromatase activity [57,58].
Effects on the breast
In a recent review [59], no randomized studies with androgenic treatment that analyzed breast cancer were found. Those found were an observational retrospective study, two cohort studies and two case–control studies, which produced inconsistent results. As a result, their conclusions were that there is no evidence that androgen therapy increases the risk of breast cancer.
Androgenic effects
Hirsutism
This represents excessive hair growth in areas that respond to androgens, as a consequence of an overproduction of endogenous androgens or a supraphysiological exposure to exogenous androgens [60].
The percentage of women with hirsutism depended on the dose employed. In a double blind, randomized clinical trial, no differences in the development of facial hair were found between one group that received only estrogens (0.625 mg of EE) and another that received androgens with MT (0.625 mg EE and 1.25 mg MT), although the study lasted for only 4 months [47]. When doses well above the physiological range, such as intramuscular injections of 150 mg of testosterone with estrogens were used, no incidence of very elevated hirsutism were found (between 15 and 20%) [61], finding amounts of 21% when using subcutaneous implants of 50 mg of estradiol and 100 mg of testosterone [62] and drastically lowering this amount when using implants of 50 mg of estradiol and only 50 mg of testosterone [63].
When using testosterone patches that released 300 μmg/day, no increase in the incidence of hirsutism was observed in comparison to placebo [48–51], except for a small but significant increase in a Phase III research study of female sexual dysfunction in testosterone patch without estrogen (APHRODITE) [53] that did not find an increase with patches of 150 mg/day, but did with those of 300 mg/day.
These results indicate that a clear relationship exists between the doses of testosterone and hirsutism, which is minimal or nonexistent when using physiological doses.
Acne
As with hirsutism, acne is dose dependent. The incidence of acne after taking 10 mg/day, 2.5 mg/day or 1.5 mg/day of MT was clearly superior to that of the control group with estrogens [52]. Nevertheless, using a 300 mg/day testosterone patch did not produce an incidence superior to that of the control group [48–53].
Virilism
The most well-known signs of virilism are deep voice, clitoromegaly and alopecia. As with the other androgenic side effects, these are dose dependent, so that with 300 mg/day patches of testosterone, no significant increase was found in comparison to control groups [48–53].
New therapeutic strategies
At present, new therapeutic strategies to combat HSDD are being investigated, including novel methods for the release of testosterone and drugs that act on the CNS.
In reference to the last of these, the most advanced treatment is flibaserine, a new nonhormonal compound. Flibanserine acts predominantly at 5-hydroxy trip tamyra (5-HT[1A]) receptors as an agonist, only seen postsynaptically and secondarily at 5-HT(2A) receptors as an antagonist. Additional binding actions include weaker antagonist actions at 5-HT(2C) and 5-HT(2B) receptors, and less defined activity at dopamine D4 receptors [64]. Flibanserine development phase was completed and part of the program was presented at the last congress of the European Society for Sexual Medicine [65]. Three Phase III studies carried out in North America (DAISY, VIOLET and DAHLIA) and a Phase III study in Europe (ORCHID) were presented. The studies evaluated the security and efficacy of flibaserine 100 mg in premenopausal women affected with HSDD. The data obtained in the critical Phase III clinical trials demonstrate that flibanserine 100 mg administered once a day at bedtime significantly increased the number of satisfactory sexual events and for sexual desire, at the same time, there was a reduction in the distress associated with HSDD.
The results of the Phase III studies indicate that the 100-mg dose of flibanserine is effective and well-tolerated in the treatment of HSDD in postmenopausal women [66,67]. In June 2010, the US FDA Advisory Panel voted that the benefits of flibanserine did not outweigh the side effects, such as dizziness, nausea and fatigue [102] and the submission was withdrawn.
Future perspective
Hypoactive Sexual Desire Disorder is a female sexual disorder that exerts a negative impact on those who suffer from it. The etiology of HSDD can include hormone and neurotransmitter disequilibria, in addition to the psychosocial factors. Few women seek medical assistance for sexual problems, and doctors are usually reluctant to talk about these subjects with their patients.
In the next 5–10 years this should change. There should be an increase in the training of medical students along with medical internists and residents. The basic knowledge of sexual medicine will be necessary for all.
We know that androgens are fundamental, but there are enormous discrepancies in the results, especially in reference to blood level measurements. The development of new diagnostic techniques will bring us closer to understanding the physiopathology of this disorder and as a consequence, therapeutic approaches.
There is no doubt that androgens improve hypoactive sexual desire. But there are still unanswered questions, and among those is whether there is a subgroup that would especially benefit in the long term.
Many of these questions will be answered, facilitating the handling of dose, combinations and duration, as well as indications and contraindications.
New therapeutic strategies will strengthen this area of medical science, which up until now has been little developed. The role of neurotransmitters, their stimulation and inhibition will open up new approaches and new possibilities. We cannot forget that women will demand better sexual health and we need to respond, since the new aptitudes and new strategies will be the objectives to meet over the next few years.
Executive summary
Hypoactive Sexual Desire Disorder (HSDD) is a persistent and recurrent lack (or absence) of sexual fantasies and desire for sexual activity that causes marked distress or difficulty in interpersonal relationships.
The prevalence of HSDD is 6% in premenopausal women, 9% in natural menopause and 12% in women with surgical menopause.
There are a number of physiological, psychological and sociological factors that can affect sexual desire.
Sexual hormones interact with neurotransmitters in the CNS, where the equilibrium between excitatory and inhibitory factors can control sexual functioning.
Dopamine carries out an essential function in the modulation of sexual desire.
Several diagnostic tools have been developed to help identify HSDD during normal medical visits.
A transdermal testosterone patch is the only approved pharmaceutical treatment for HSDD in Europe, authorized for women who have undergone a bilateral ovariectomy or hysterectomy and who follow a simultaneous estrogen treatment.
Footnotes
Hypoactive Sexual Desire Disorder and current pharmacotherapeutic options in women
To obtain credit, you should first read the journal article. After reading the article, you should be able to answer the following, related, multiplechoice questions. To complete the questions and earn continuing medical education (CME) credit, please go to www.medscapecme.com/journal/wh. Credit cannot be obtained for tests completed on paper, although you may use the worksheet below to keep a record of your answers. You must be a registered user on Medscape.com. If you are not registered on Medscape.com, please click on the New Users: Free Registration link on the left hand side of the website to register. Only one answer is correct for each question. Once you successfully answer all post-test questions you will be able to view and/or print your certificate. For questions regarding the content of this activity, contact the accredited provider,