
Abstract
Adverse effects have been related to infertility treatments. Infertility in general, and female infertility in particular, is a well established risk factor for cancer development, especially ovarian, breast and endometrial cancer. This article addresses the possible association between infertility and cancer development, with an emphasis on the influence of infertility treatments, through a meticulous search of the literature published thus far. While results regarding the possible association of infertility, ovulation induction medications and invasive ovarian cancer show no increased risk and are reassuring, results for increased risk for breast cancer and endometrial cancer following exposure to ovarian stimulation medications are inconclusive. Larger population studies with longer periods of follow-up and better adjustment for confounding factors are needed.
Keywords
More than 15% of couples will face infertility problems during their reproductive years, and will seek treatment [1]. Adverse effects have been related to infertility treatments, many of which are short term, (i.e., multiple pregnancies [2,3], ectopic pregnancies [4] and hyperstimulation syndrome [5–7]). However, long-term adverse effects of infertility treatments are still controversial. While infertility in general, and female infertility in particular, is a well established risk factor for cancer development, with special emphasis on ovarian, breast and endometrial cancer [8–10], the role of infertility treatments as a possible risk factor for cancer development is less clear. Therefore, it is important to evaluate the possible additional risks associated with infertility medications, that could by themselves modify the hormonal environment and be cofactors towards cancer development [10].
Part of the problem in evaluating the possible association between infertility treatments and cancer development is to conduct a well-designed epidemiological investigation. Cohort studies are usually conducted for relatively rare exposures and frequent outcomes. The incidence of the investigated outcome will be compared between a group of exposed individuals and a group of unexposed individuals after a sufficient follow-up period and the relative risk (RR) for the outcome between these two groups will be calculated as the ratio between the incidences. This is the most direct method to calculate the risk. However, in the case of exposure to infertility treatments the recruitment of exposed individuals could be biased by the inclusion of only the patients who that approached infertility clinics. It will be even more difficult to assemble the group of unexposed individuals (i.e., infertile women that were not exposed to infertility treatments) and, therefore, some of the studies use the general population rates for comparison of cancer incidence. This compromise, while easier to investigate, only allows the calculation of a standardized incidence ratio (SIR), which is an underestimation of the actual risk, since the general population rates reflect both the infertile and the fertile population. In addition, comparison with the general population data, usually through linkage to registries, does not allow for complete control of a wide range of potential confounding factors, such as parity, menstrual factors, family history of cancer, oral contraceptive use, and other hormone use, that will be available from medical records. Moreover, due to the long latency period for cancer development, most cohort studies will be conducted as a historical cohort in order to avoid very long follow-up periods. Therefore, some of the individuals will have been exposed to treatment protocols that are no longer relevant. However, the most profound limitation of the cohort study design in evaluating cancer incidence following infertility treatments would be the fact that some of the investigated cancers are rare, such as ovarian and endometrial cancers, and therefore even a substantial sized cohort will yield only few cancer cases at the end of follow-up, which will not be enough to control for possible confounding factors. The insufficient number of cancer cases could be overcome by using a case–control designed study. While case–control studies are usually conducted for rare outcomes, such as cancer development, they may suffer from a recall bias on the information about infertility and infertility treatments. Since infertility treatments, especially in past decades, were relatively infrequent, only a few cases will actually report exposure. Moreover, owing to the fact that it is not possible to evaluate the true incidence for cancer development in a case–control design, only an estimation of the risk could be calculated as the odds ratio (OR).
This article addresses the possible association between infertility and cancer development with an emphasis on the influence of infertility treatments as presented by the various studies published thus far.
Ovarian cancer
Nulliparity represents a known risk factor for epithelial ovarian cancer. Therefore, the differentiation between the effect of infertility
However, most of these reports were related to women who were diagnosed with ovarian cancer during the infertility treatments or shortly after and, therefore, may be regarded as coincidental findings that are not related to the infertility treatments themselves. The possible link between exposure to ovulation-induction drugs and ovarian cancer development has biological credibility, given that ‘incessant ovulation’ and associated alternation in endogenous hormones during reproductive years are plausible explanations for several factors that alter ovarian cancer risk [26–28].
The association between infertility, ovulation-induction treatments and ovarian cancer development has been investigated in numerous case–control and cohort studies. As for invasive ovarian cancer development, all but one case–control study failed to demonstrate a significant excess risk of invasive ovarian cancer following treatments for infertility
Summary of case–control studies regarding ovarian stimulation and the risk for ovarian cancer.

OR: Odds ratio.
Whittemore
Summary of cohort studies regarding ovarian stimulation and the risk for ovarian cancer.
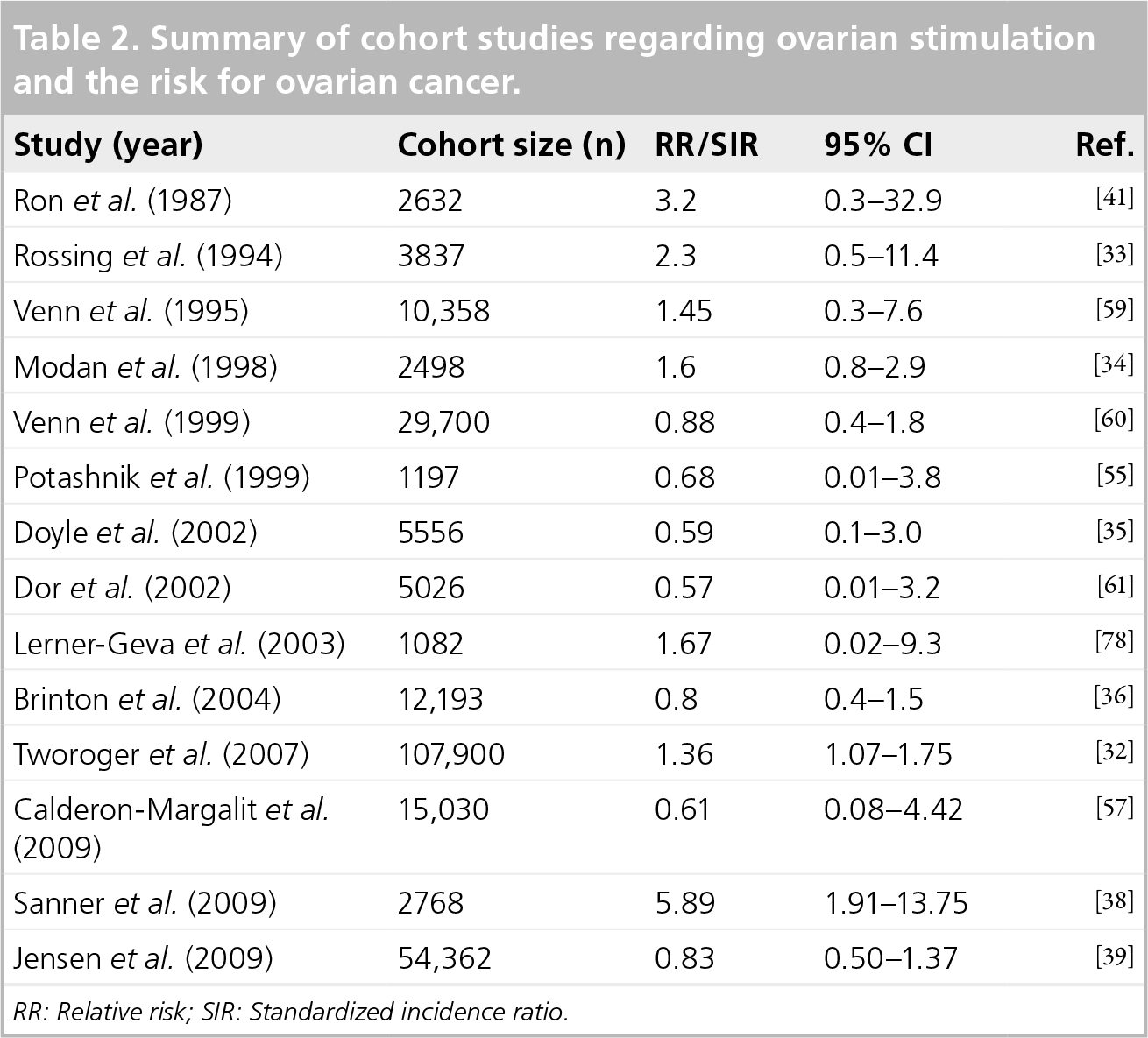
RR: Relative risk; SIR: Standardized incidence ratio.
Sanner
In a recent update for cancer development in a cohort of infertile women with more than 84,000 women and over 30 years follow-up, 18 ovarian cancer cases were observed compared with 18.1 expected with no excess risk for ovarian cancer that was evident (SIR: 1.0; 95% CI: 0.6–1.6) [40]. This cohort of infertile women, which was previously investigated by Ron
In contradiction to the results for invasive ovarian cancer, the risk for borderline tumors of the ovary in infertile women was found to be significantly increased in both case–control and cohort studies
Summary of studies regarding ovarian stimulation and the risk for borderline tumors of the ovary.
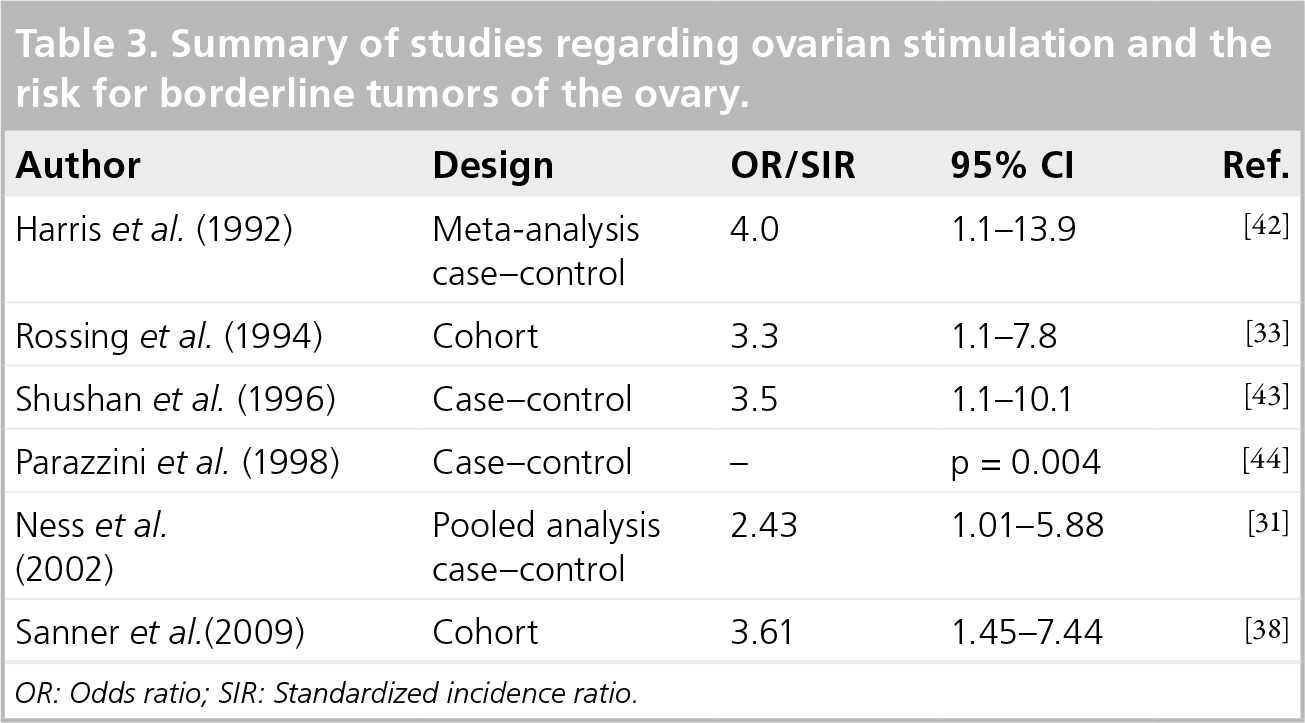
OR: Odds ratio; SIR: Standardized incidence ratio.
In conclusion, results regarding the possible association of infertility, ovulation-induction medications and invasive ovarian cancer demonstrate no increased risk and are reassuring. The possible excess risk of borderline tumors of the ovary may be due to intrinsic characteristics of these tumors or surveillance bias.
Breast cancer
Breast cancer is the leading cause of malignancy in women in developed nations with peak incidence at the age of 60–65 years [48]. Nulliparity, younger age of menarche, older age at menopause and late age at first birth and infertility are traditionally considered to be potential risk factors for breast cancer development [49]. However, the issue of the potential risk associated with exposure to infertility treatments is less clear. Specific concerns regarding the effects of fertility drugs have been raised by the recognized effects on breast cancer risk of ovulation and hormonal patterns related to estrogen levels, and, more recently, progesterone [28,50]. Several case–control studies
Summary of case–control studies regarding ovarian stimulation and the risk for breast cancer.

hMG: Human menopausal gonadotropin; OR: Odds Ratio; SIR: Standardized incidence ratio.
Summary of cohort studies regarding ovarian stimulation and the risk for breast cancer.

CC: Clomiphene citrate; HR: Hazard ratio; RR: Relative ratio; SIR: Standardized incidence ratio.
Summary of studies regarding IVF and the risk for breast cancer.
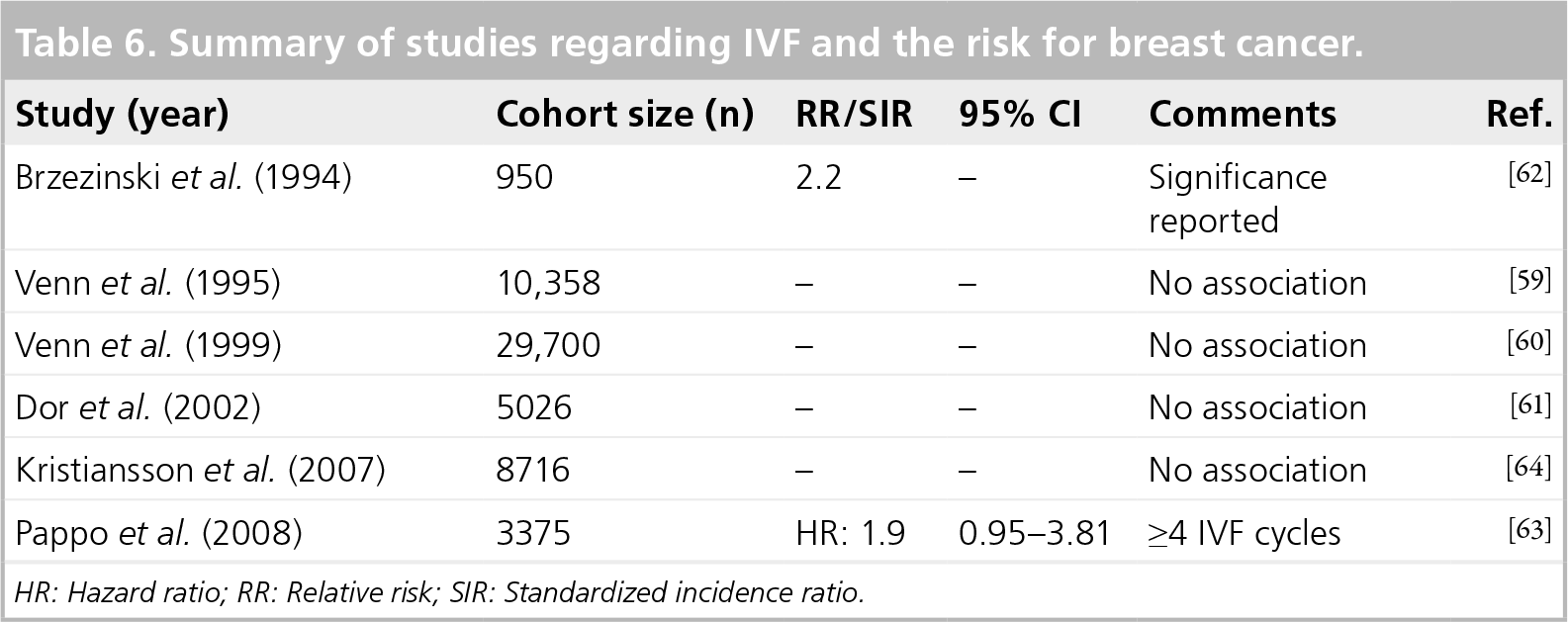
HR: Hazard ratio; RR: Relative risk; SIR: Standardized incidence ratio.
In a recent meta-analysis by Zreik
In conclusion, numerous studies regarding the possible association between infertility, ovulation-induction exposure and breast cancer have been conducted. Although these studies include significant sample sizes and sufficient follow-up for cancer development, results regarding effects of fertility drugs on breast cancer risk are still conflicting. Given that breast cancer is widely recognized as having a hormonal etiology, further assessment of the effects of ovulation-induction drugs should be undertaken [67].
Endometrial cancer
Endometrial cancer has been significantly associated with infertility in most studies published to date [10]. Compared with the general population rates of endometrial cancer, the risk was significantly increased by ninefold in infertile patients with normal estrogen levels and progesterone deficiency [41,34]. Venn
However, the association between exposure to ovulation induction and endometrial cancer development, independent of the infertility problem, is less clear.
Benshushan
Most studies
Summary of cohort studies regarding ovarian stimulation and the risk for endometrial cancer.
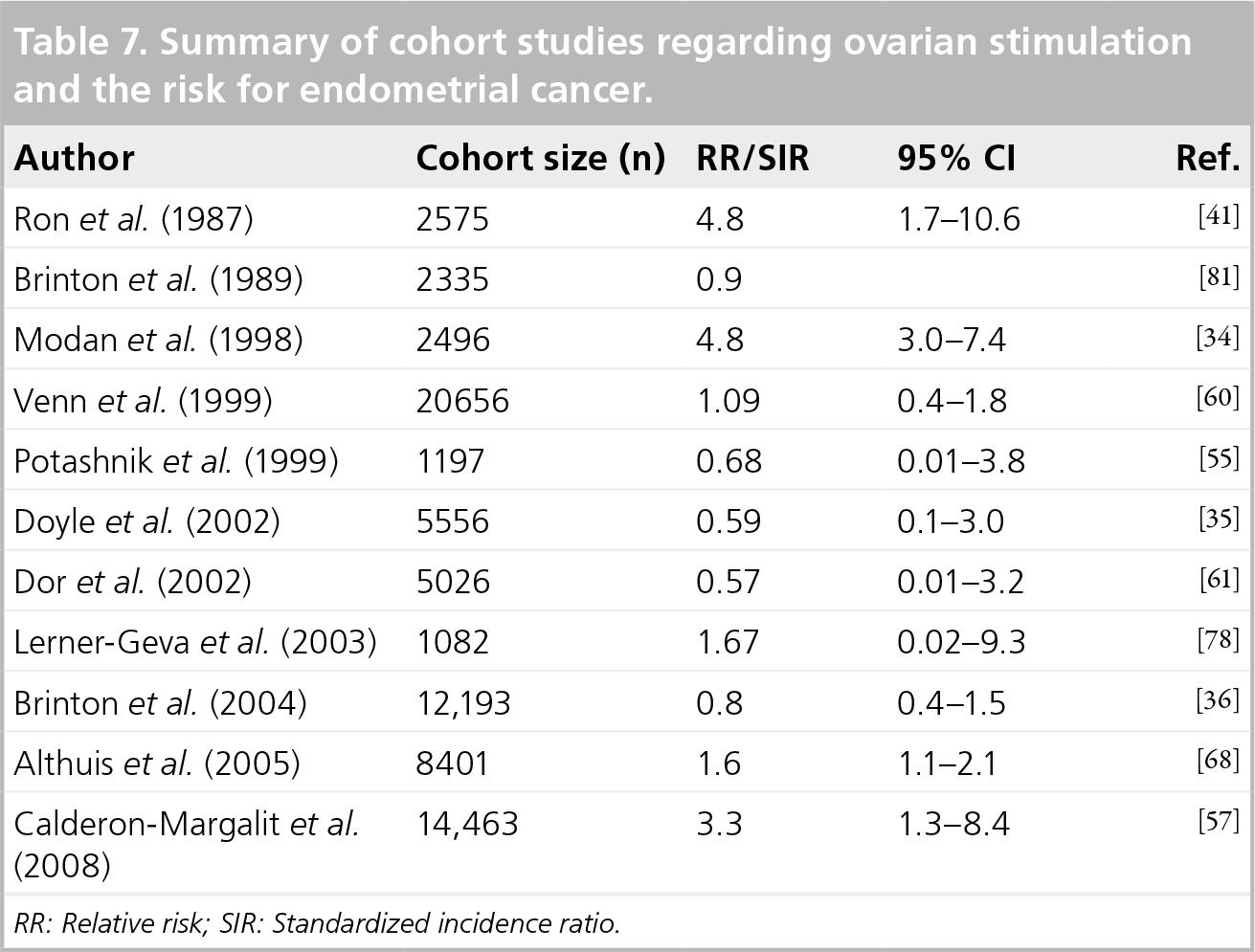
RR: Relative risk; SIR: Standardized incidence ratio.
In conclusion, the risk for endometrial cancer development in infertile women, and especially in women with unopposed estrogen state, is well established. However, data regarding the possible association to exposure of ovulation-induction drugs to endometrial cancer development is inconclusive.
Executive summary
Infertility in general, and female infertility in particular, is a well established risk factor for cancer development, especially ovarian, breast and endometrial cancer.
Results regarding the possible association of infertility, ovulation induction medications and invasive ovarian cancer show no increased risk and are reassuring.
The possible excess risk of borderline tumors of the ovary may be due to intrinsic characteristics of these tumors or surveillance bias.
Results regarding the effects of fertility drugs on breast cancer risk are still conflicting.
Increased risk for endometrial cancer following exposure to ovulation-induction medication is inconclusive.
Larger population studies with longer periods of follow-up and better adjustment for confounding factors are needed.
Footnotes