
Abstract
Breast cancer is the most common malignant tumor in women. Increasing survival rates after breast cancer, new reproductive techniques and growing interest regarding the quality of life after cancer have brought the possibilities of fertility-preserving treatment to the center of attention of oncologists and affected patients. Many of these women suffer from infertility and premature menopause as a result of chemotherapy. Several measures, for example gonadotropin-releasing hormone analogs, hormonal stimulation to cryopreserve oocytes, ovarian tissue cryoconservation or a combination of the methods, can be undertaken depending on the hormone receptor status of the tumor, and the patient's age and partner status. Embryo cryopreservation is currently the most promising fertility preservation option. Early counseling on fertility-preserving strategies is of utmost importance, so that the fertility-preserving method can be integrated into the oncologic therapy regime.
Keywords
Breast cancer is the most common malignant tumor in women [1], and has an incidence of approximately 45 cases per 100,000 women during the reproductive years [101]. As a result of improved diagnosis and treatment, the 5-year survival rate after breast cancer is over 88% [2], which means that the number of long-term survivors after breast cancer is increasing.
Because the age at delivery of the first child is rising [102,103], family planning in young women who are affected by breast cancer is often not completed and they may have an intense desire to conceive after overcoming the disease [3].
Women whose family planning is not complete and/or who have a history of sterility have great concerns regarding their fertility, especially women under the age of 40 years. However, women who no longer have a prospective desire to conceive are also emotionally affected by their loss of fertility [4]. A web-based survey showed that only 51% of oncology patients had the feeling that their concerns regarding their fertility were adequately addressed [5].
Advances in reproductive medicine have made the development of various fertility-preservation techniques possible, which can be performed with the aim of protecting ovarian function and fertility prior to chemotherapy. Fertility preservation in young patients is now an important issue in oncology.
Consequences of chemotherapy on ovarian function & fertility
Tumors in young breast cancer patients often have more aggressive tumor characteristics, such as a higher proliferation index, a positive
The greatest numbers of follicles are present in the ovary during the fetal period. From this point, there is a steady decline in the number of follicles. A newborn baby girl has a ‘pool’ of 106 oocytes; this pool decreases to approximately 3 × 105 during puberty. Over the course of the reproductive phase, approximately 300–400 oocytes are normally ovulated [6]. The follicle pool diminishes exponentially with age, with a significant increase in the degeneration rate from an age of 37 to 38 years. The menopause is reached when there are 1000 follicles or less, and the low number of follicles can no longer sustain the hormonal cycle regulation [7].
It is presumed that the detrimental effect of cytotoxic agents to the ovary is caused by damage of the perioocyte granulose cells in the ovaries. Cyclophoshamide harms both resting and dividing cells, and studies on mice have shown that follicular destruction rises exponentially with increasing doses [8]. Modern chemotherapeutic regimes include mostly combined cytotoxic drug treatments, so it is difficult to determine the effect of a single substance. Damage to ovarian tissue is irreversible, and histological samples of ovarian tissue after chemotherapy have shown images that range from a reduction in the follicle count to complete failure with fibrotic remodeling of the ovarian tissue [9]. Therefore, chemotherapy-induced amenorrhea is not a consequence of impaired hypothalamic–hypophyseal gonadotropin secretion, but is due to a primary disorder of the ovarian function caused by the depletion of the follicle pool. The loss of follicles was shown by the significant drop of the anti-Müllerian hormone (AMH) levels after one or two series of chemotherapy [10].
There is a wide range of these functional disorders, from a transient luteal insufficiency and anovulatory cycles to permanent hypergonadotropic amenorrhea. The amenorrhea rates are not only dependent on the type and dose of chemotherapy used, but also on the patient's age.

In addition to a loss of fertility, consequences of ovarian insufficiency include hot flushes, night sweats, mood swings, depression, loss of libido, alopecia, loss of vaginal lubrication and a significantly increased risk of developing osteoporosis. Furthermore, the risk of developing a neurological or cardiovascular disease such as Alzheimer's or coronary heart disease is increased [11].
Consequences of antihormonal treatment on ovarian function & fertility
Not all premenopausal women require chemotherapy. Adjuvant hormonal treatment in the form of ‘hormone withdrawal’ as oncological adjuvant therapy can be planned for a total duration of 5 years in some patients with a hormone receptor-positive tumor, instead of adjuvant chemotherapy. The medication for adjuvant hormonal therapy could vary, corresponding to the guidelines of each county. In Germany, gonadotropin-releasing hormone (GnRH) analogs are administered for 2 years [104]. After an initial short ‘flare-up’ effect, GnRH analog (GnRH-a) leads to a drug-induced hypogonadotropic hypogonadism with consequent amenorrhea and menopausal symptoms. The antihormonal treatment is continued in years 3–5 with the antiestrogen drug tamoxifen. Tamoxifen, a selective estrogen modulator, does not typically cause suppression of ovulation. Amenorrhea, which may occur with tamoxifen, is usually reversible [12], and does not indicate damage to the ovaries. However, there is an age-related reduction in fertility because of the 5 years of continuous hormonal treatment and the increasing age of the patient [13]. As well as the quantitative loss from the physiological degeneration rate of the oocytes in the ovaries, there is also a qualitative loss. This is shown by the reduced ability to form an egg cell that is capable of being fertilized. Because of the sometimes long storage period in the follicle pool, the oocytes and granulosa cells are subjected to aging process-related changes. Most theories regarding the aging process of tissues say that the side effects of normal metabolism lead to irreparable damage to the cell structure [14]. These factors can have a negative effect on the chances of pregnancy after the end of treatment for breast cancer.
Counseling of young patients prior to chemotherapy
Knowledge about the possible loss of fertility caused by chemotherapy can influence oncological treatment options, especially in women under the age of 40 years, women with no children or only one child, and/or women with a history of sterility [5,15]. A longitudinal study (which admittedly only included 13 women under the age of 40 years) found that the biggest regret concerning decisions made about treatment was that the possibility of performing fertility-preservation treatment before the start of chemotherapy was not made use of [16]. Data collected from counseling of breast cancer patients on fertility-preservation methods prior to chemotherapy have shown that more than 60% of all counseled patients under the age of 40 years decided to undergo treatment with one or more fertility-preservation methods [17].
The fears and concerns of young women with breast cancer are often not adequately addressed by the responsible doctors. The consequence is that a potential loss of fertility and the possibilities of fertility preservation are not sufficiently discussed. If the patients are suitably informed, and if they include these aspects in their decision-making, it can be expected that the psychosocial outcome for the patient is better [4].
This highlights the need for early and comprehensive counseling for patients who are affected by breast cancer about the effects of chemotherapy on fertility. This need has also been emphasized in publications by the Ethics Committees of both the American Society for Reproductive Medicine and the American Society of Clinical Oncology (ASCO) [18,19].
The FertiPROTEKT network was established in Germany in 2006 to improve the care of young women prior to chemotherapy [105]. Its aim was the systematic establishment, optimization and synchronization of fertility-preservation methods. From a launch meeting with 30 university centers, a network covering Germany, Switzerland and Austria has now been developed, where young girls and women under the age of 40 years can be counseled regarding fertility-preservation methods prior to receiving chemotherapy, which would probably cause disruption to their ovarian function. Counseling and treatments, including complications occurring, are recorded and scientifically analyzed [20]. A special interest group on this subject was founded by the European Society for Human Reproduction and Embryology (ESHRE) in November 2009, which adopts the principles of the FertiPROTEKT network [21].
Fertility-preservation methods
The following methods of fertility preservation are available:
Ovarian protection using GnRH-a (GnRH protection)
Removal of ovarian tissue for cryoconservation
Hormonal stimulation to collect oocytes with cryoconservation of fertilized or unfertilized oocytes
A combination of the various methods
GnRH protection
By administering a GnRH-a before the start of chemotherapy, one hopes to put the ovaries into a drug-induced ‘retirement’ to protect the follicles, as observations have shown that young girls who received chemotherapy before entering puberty still developed normal cycles during puberty [22]. Follicles under early gonadotropin stimulation have an especially high risk of falling victim to apoptosis as a result of chemotherapy. Administration of a GnRH-a leads to an initial flare-up followed by downregulation of the gonadotropins FSH and LH, and therefore no further follicle stimulation [23]. A downregulation of FSH and LH can be expected to occur 7–14 days after administration of GnRH-a. If chemotherapy is planned to be started earlier, parallel administration of GnRH-a can be considered to reduce follicle stimulation as a result of the flare-up effect. However, there are still insufficient data on the last approach.
The efficacy of GnRH-a use to protect the ovaries is the subject of many studies, with inconsistent data: current work [24,25] and a meta-analysis by Clowse
As a consequence of the inconsistent data, administration of a GnRH-a should not be offered as the only method of ovarian protection.
The advantage of giving GnRH-a is that it does not require postponement of the start of chemotherapy.
It is still unclear whether GnRH protection of the ovaries can adversely affect the oncological treatment in patients with hormone receptor-positive breast cancer. The source of this concern is that administration of tamoxifen leads to a tamoxifen-induced arrest of cancer cell proliferation, whereby the sensitivity of the cancer cells to chemotherapy is reduced [31]. The GnRH-related suppression of the estrogen level could lead to a similar effect [32], and the consequence could be a reduction in the efficacy of the chemotherapy. For this reason, the ASCO recommends that women should only be treated with this method of fertility preservation as part of a study [19].
Ovarian tissue removal for cryoconservation
One treatment option that does not affect the estrogen level is the removal of ovarian tissue with subsequent cryoconservation. This method is usually performed as a minimally invasive surgical procedure and, with sufficient planning, can be combined with breast surgery. Removal of the tissue should be performed without trauma or thermal damage to the tissue if possible, as the ovarian cortex is rich in primordial follicles. Electrosurgical removal of the tissue for cryoconservation damages the tissue and the primordial follicles, and less vital tissue will be available for later retransplantation as a result.
If a spontaneous menstrual cycle does not occur after chemotherapy is completed, retransplantation of the ovarian tissue could re-establish the patient's ovarian function and fertility.
Theoretically, there are three options available to use ovarian tissue:
A future possibility could be the process of
Xenografting of tissue, the transplantation of the ovarian tissue to, for example, immunodeficient mice, with subsequent hormonal stimulation of the mice to collect oocytes, is ethically very controversial.
Heterotopic retransplantation under the skin has the advantage that no new intra-abdominal procedure must be performed. After hormonal stimulation of heterotopically retransplanted ovarian tissue, oocytes were retrieved and a fertilized oocyte developed into a four-cell embryo, but no pregnancy was achieved [35]. Physiological conditions are restored with retransplantation in the adnexal space, so a pregnancy occurring spontaneously is possible. This option has been performed successfully and nine known pregnancies in eight women after retransplantation are mentioned in the literature [36]. However, this is still an experimental procedure, which patients should be explicitly informed about [19].
Ovarian function can be re-established, up to a certain extent, after transplantation of ovarian tissue; however, the efficacy of using cryoconserved ovarian tissue is reduced compared with when using ‘fresh’ noncryoconserved tissue [36]. In monozygotic twins, discordant for premature ovarian failure, transplantation of heterologous ‘fresh’ ovarian tissue led to successful pregnancies [37]. Proof of long-term efficacy and life expectancy of the ovarian transplant is not yet available. The risk of retransplantation of malignant cells after overcoming breast cancer must be discussed with the patient. This problem has been addressed by Sanchez-Serrano
An important aspect of tissue removal is that chemotherapy need not be postponed because of the surgical procedure required to remove the tissue. A follow-up study after ovarian tissue removal showed that removal of ovarian tissue did not affect cancer treatment [39].
As significant experience in the field of cryoconservation and retransplantation is expected to be gained over the next few years, this method is especially suitable for young patients prior to chemotherapy.
Hormonal stimulation to collect oocytes
The most effective and most established method of fertility preservation is currently hormonal stimulation to collect oocytes, by vaginal follicle puncture, fertilization using IVF or intracytoplasmic sperm injection (ICSI) and final cryoconservation of the fertilized egg cell in the pronuclear stage. Patients without a long-term partner can have their unfertilized eggs frozen; however, the survival rates of the egg cells after thawing are reduced [40,41]. Vitrification of the oocyte improves survival rate after thawing and pregnancy rates [42]. The birth rate is now approximately 5–6% per thawed egg [43].
With the ‘classical stimulation protocol’, the time period required for stimulation is between 2 and 5 weeks, depending on the time since the last period. The aim is to keep this time period as short as possible. However, hormonal stimulation can also be started in the second half of the cycle, without a significant reduction in the number of oocytes collected, compared with patients receiving stimulation in the follicular phase [44]. Oocytes suitable for fertilization can almost always be collected in a time frame of 2 weeks.
In a recent study about fertility-preservation methods in breast cancer patients, Oktay
Collection of oocytes must be very carefully discussed with patients with hormone receptor-positive breast cancer because of the stimulation-induced increase in the estradiol level. A possible alternative is performing IVF/ICSI treatment in a ‘natural cycle’, without additional hormonal stimulation and consequent increase in estradiol levels. However, the oocyte yield in a natural cycle is low, and the effort and cost of this procedure cannot be justified.
Oktay
Combination of the fertility-preservation techniques
As the individual techniques only have limited efficacy, it is advisable to combine several techniques with one another. Whilst GnRH-a administration can be unproblematically combined with ovarian tissue removal (except for patients with hormone-dependent tumors), the evaluation of the safety and efficacy of combining ovarian tissue removal and hormonal stimulation is unclear because of a lack of data.
In principle, there are two approaches with this combination: performing hormonal stimulation and oocyte collection with subsequent ovarian tissue removal, or removal of ovarian tissue first, followed by hormonal stimulation. Alongside a high risk of bleeding because of the larger and well-vascularized ovaries, the first approach also carries the risk that when tissue is removed from the stimulated ovary, only ovarian tissue containing few primordial follicles can be removed. The chance that the tissue recovers its function and a pregnancy occurs would be low because of the low number of primordial follicles in the transplanted tissue.
By contrast, in a pilot study it was shown that removal of ovarian tissue and starting hormonal stimulation a mean of 2 days postoperatively can be performed without risks for the patient and without a reduction in the number of oocytes, their maturity and the fertility rate [49].
Which option for which patient?
As the decrease in the number of follicles present in the ovary (the ovarian reserve) can vary greatly between individuals, it is sensible to perform a measurement of the ovarian reserve in parallel with planning fertility-preservation procedures.
There are now clinical laboratory and sonographic parameters that can estimate the ovarian reserve. Measurement of FSH is the most frequently used test. An indicator of reduced function is a slightly increased FSH with a low estrogen level in the early follicular phase. The most significant parameter is AMH. It is produced in the granulosa cells, especially in the secondary, the preantral and the small antral follicles [50], and therefore accurately reflects the ovarian reserve. The AMH level also had good reproducibility from one cycle to the next [51]. A review by Domingues
Depending on the following points, fertility-preservation techniques that are possible and appropriate for the patient and her partner can be discussed, and can then be included in the treatment regimen with the oncologist's agreement:
Tumor characteristics
Oncological treatment
Time until first chemotherapy
Partner status
Age
Ovarian reserve
The hormone receptor status and the oncological treatment regimen in terms of adjuvant or neoadjuvant therapy are decisive for the planning or the combination of various fertility-preservation techniques. All fertility-preservation methods can be used in patients with a hormone receptor-negative tumor in the adjuvant situation; however, in the neoadjuvant situation, hormonal stimulation needs to be carefully discussed. Hormonal stimulation to collect oocytes in a patient with a hormone receptor-positive tumor must be extensively discussed with the patient and, in the neoadjuvant situation, ovarian tissue removal with cryoconservation is the only method available for use. The possible methods depending on tumor characteristics and oncological therapy are shown in
Recommendations of the FertiPROTEKT network: fertility-preserving strategies for patients with breast cancer.
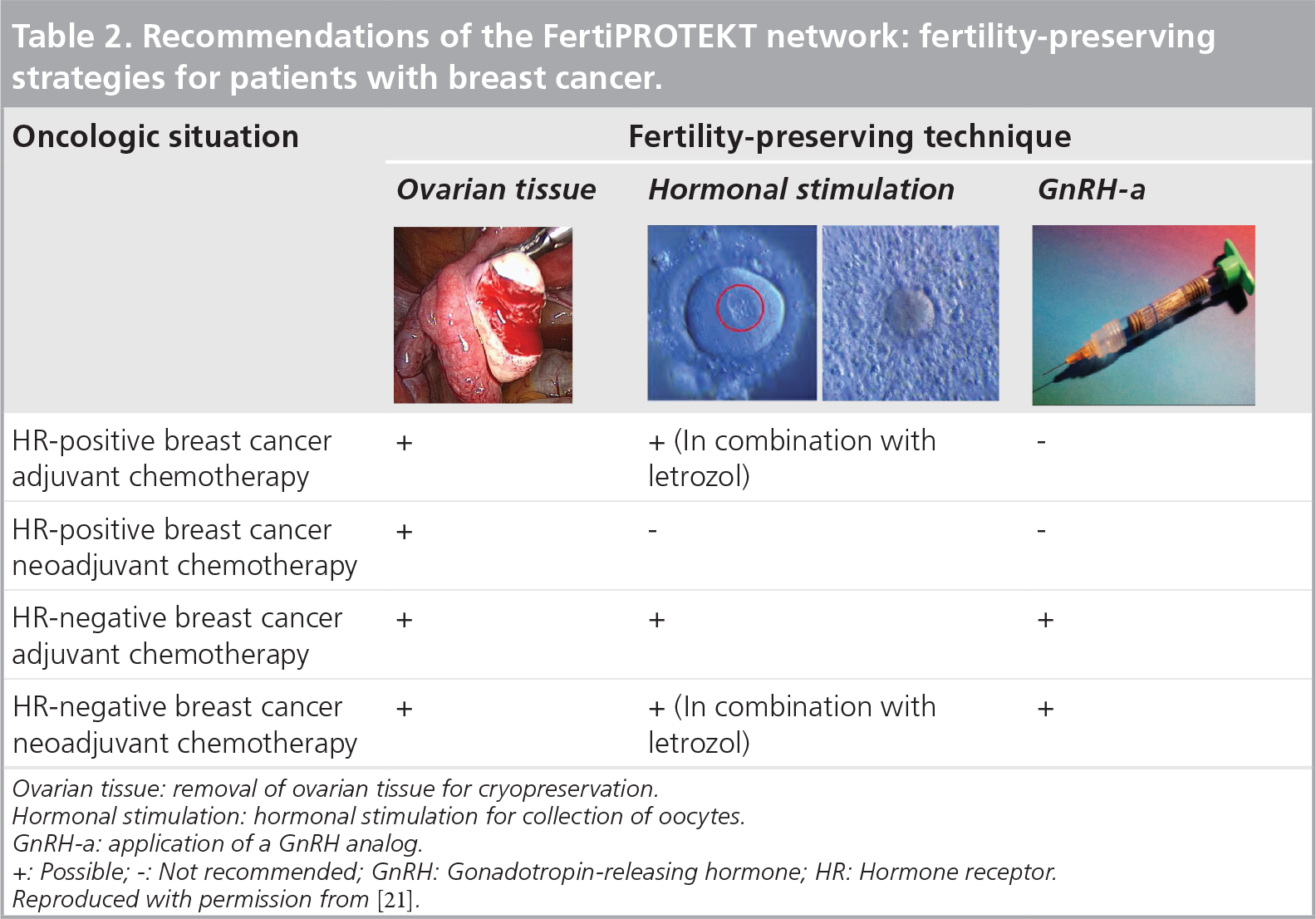



Ovarian tissue: removal of ovarian tissue for cryopreservation.
Hormonal stimulation: hormonal stimulation for collection of oocytes.
GnRH-a: application of a GnRH analogue.
+: Possible; -: Not recommended; GnRH: Gonadotropin-releasing hormone; HR: Hormone receptor.
Reproduced with permission from [21].
To avoid worsening the efficacy of adjuvant chemotherapy, chemotherapy should be started as closely as possible to the cancer surgery. Hormonal stimulation to collect oocytes delays the start of treatment when compared with breast cancer patients who did not decide on this method of fertility-preservation. However, the start of chemotherapy was always within a time frame of 12 weeks [48], and no detrimental effect as a result of a possible time loss was suspected. Laparoscopic removal of ovarian tissue can be combined with breast surgery so there is no loss of time. If the procedure is planned separately from the breast surgery, no more than 2 days are generally needed for planning and performance of the procedure. GnRH-a administration does not imply any loss of time.
For patients with a long-term partner, hormonal stimulation to collect oocytes, fertilization of the oocytes using the partner's sperm and subsequent cryoconservation of the pronuclear (PN) stage are the fertility-preservation methods that offer the best chances of pregnancy, as these are established methods of infertility treatment. If the patient and her partner choose this option, at least in Germany it must be carefully pointed out to the patient that the PN stage can only be retrieved by both partners together at a later date. In the case of a separation or of the death of a partner, the patient alone cannot have access to the PN stage. Depending on the national law, this situation may vary from country to country. The possibility of embryo donation does not exist in Germany.
Executive summary
Breast cancer is the most common malignant tumor in women. Long-term survival has increased as a result of improved diagnosis and treatment.
Chemotherapy can seriously damage the ovaries; the extent depends on the agent used and the age of the patient.
Antihormonal treatment does not damage the ovaries; however there is an age-related reduction in fertility, depending on the duration of treatment.
Patients affected by breast cancer require early and extensive counseling on the effects of chemotherapy on their fertility and methods of fertility preservation.
Gonadotropin-releasing hormone protection: the data on the efficacy of gonadotropin-releasing hormone analogue administration are inconsistent, therefore it should not be offered as the only method of ovarian protection.
Removal of ovarian tissue for cryoconservation: ovarian tissue removed prior to chemotherapy is cryoconserved and can be orthotopically retransplanted if there is ovarian insufficiency. However, this procedure is still seen as experimental.
Hormonal stimulation to collect oocytes: the most effective and best-established method of fertility preservation is hormonal stimulation to collect oocytes, and the cryoconservation of fertilized or unfertilized oocytes.
Hormone receptor status, oncological treatment and the partner status of a patient are decisive for the planning of fertility preservation methods and choosing which options are suitable for which patients.
If measurement of the ovarian reserve before the start of chemotherapy showed a significant reduction, the patient must be informed that hormonal stimulation to collect oocytes can result in a low or no response, which means that only a few or no oocytes can be collected. The chances of a later pregnancy are therefore significantly reduced. It must also be pointed out to patients with a proven reduced ovarian reserve that if ovarian tissue is removed as a fertility-preservation method, only a few primordial follicles, and therefore little functioning ovarian tissue, can be removed and cryoconserved.
Conclusion
The improved prognosis for young patients after being affected by breast cancer and awareness of fertility preservation as being an important part of their quality of life have brought fertility preservation to the attention of gynecologists, oncologists and the patients themselves. Early patient counseling on the effects of chemotherapy on ovarian function, as well as on fertility-preservation methods and their risks and the chances of a later pregnancy, are important.
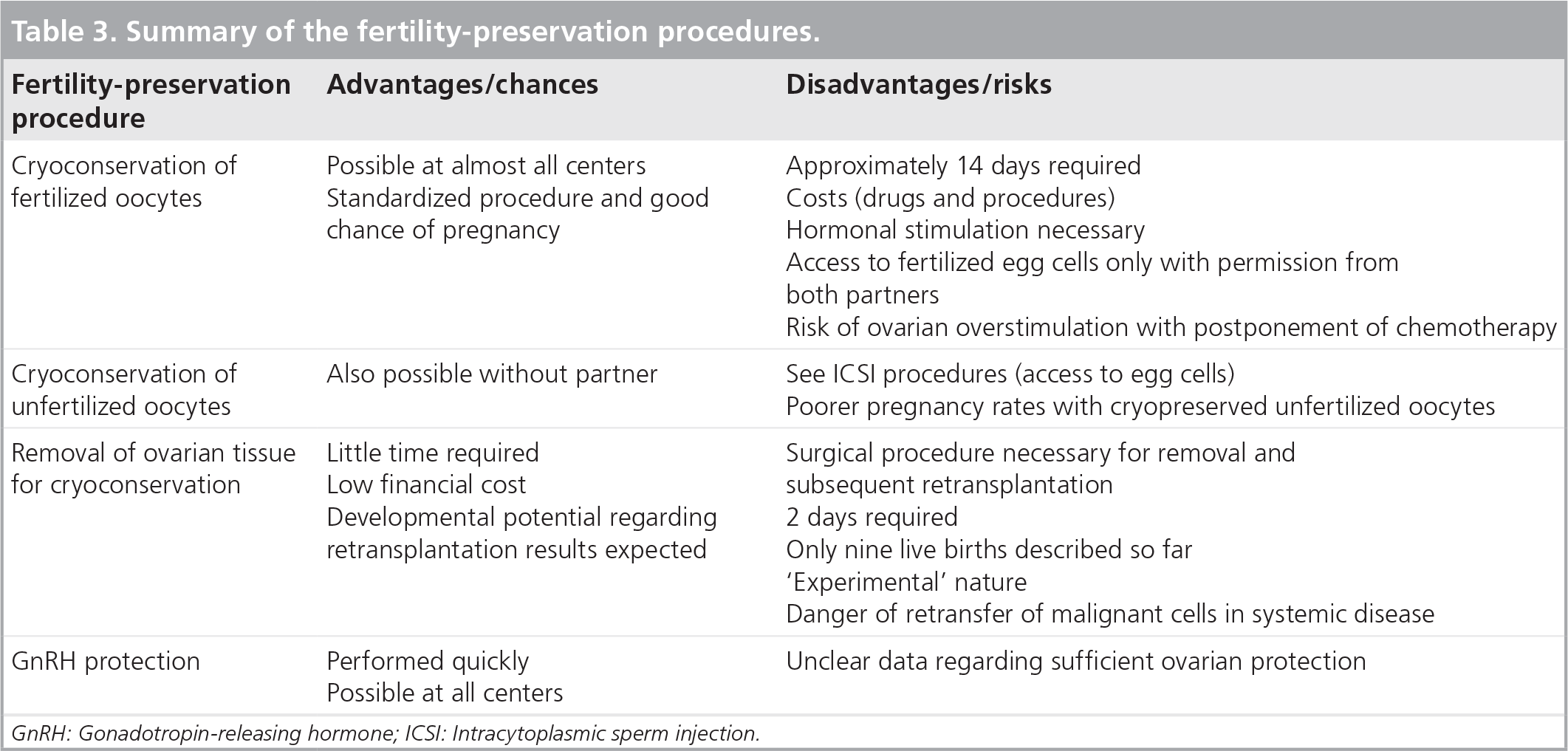
Summary of the fertility-preservation procedures.
Future perspective
The desire to preserve fertility has further increased as a result of the improved chances of curing breast cancer in young women. Ovarian stimulation to collect oocytes with subsequent cryoconservation is currently the best option for a later pregnancy. However, the long-term effects of hormonal stimulation on the patient are still unclear. As experience grows, removal of ovarian tissue for cryoconservation with the option of later retransplantation will gain acceptance, as this method does not require hormonal stimulation and, after successful transplant, it is possible that a pregnancy could occur spontaneously.
Footnotes