
Abstract
Stroke has a greater effect on women than men owing to the fact that women have more stroke events and are less likely to recover. Age-specific stroke rates are higher in men; however, because of women's longer life expectancy and the much higher incidence of stroke at older ages, women have more stroke events than men overall. The aims of this prospective study in consecutive patients were to assess whether there are gender differences in stroke risk factors, treatment or outcome. Consecutive patients with ischemic stroke were included in this prospective study at four study centers. Disability was assessed using a modified Rankin Scale score (≥3 indicating disabling stroke) in both genders at 90 days. Outcomes and risk factors in both genders were compared using the χ2 test. Multiple logistic regression analysis was used to identify any independent predictors of outcome. A total of 1136 patients were included in this study; of these, 494 (46%) were female. Women were statistically older compared with men: 76.02 (± 12.93) and 72.68 (± 13.27) median years of age, respectively. At admission, females had higher NIH Stroke Scale scores compared with males (9.4 [± 6.94] vs 7.6 [± 6.28] for men; p = 0.0018). Furthermore, females tended to have more cardioembolic strokes (153 [30%] vs 147 [23%] for men; p = 0.004). Males had lacunar and atherosclerotic strokes more often (146 [29%] vs 249 [39%] for men; p = 0.002, and 68 [13%] vs 123 [19%] for men; p = 0.01, respectively). The mean modified Rankin Scale score at 3 months was also significantly different between genders, at 2.5 (± 2.05) for women and 2.1 (± 2.02) for men (p = 0.003). However, at multivariate analysis, female gender was not an indicator for negative outcome. It was concluded that female gender was not an independent factor for negative outcome. In addition, both genders demonstrated different stroke pathophysiologies. These findings should be taken into account when diagnostic workup and treatment are being planned.
Stroke is the third leading cause of death in Western countries, as well as being a leading cause of long-term neurological disabilities in adults, and a major cause of dementia, depression and epilepsy [1–3]. Overall, women have a lower stroke risk than men when matched for age. However, at 85 years of age, women's risk is significantly greater compared with men [4]. Women are more likely to reach and exceed this age and, as such, this female subgroup has become a specific healthcare issue for society [5]. In addition, there is evidence that even after adjusting for age, women tend to have poorer outcomes and greater pre- and poststroke dis-abilities [6], while in other studies, most reported gender differences in stroke have been explained by confounding factors [7].
The aims of this prospective study in consecutive patients were to assess whether there were any gender differences in stroke risk factors, treatment or outcome, and if female gender was an independent risk factor for negative outcome.
Methods
The methods of this study has been described elsewhere [8]. This study was designed to investigate different aspects of stroke care, such as hemorrhagic transformation, hyperglycemia, hypertension and gender differences. Briefly, consecutive, nonselected patients admitted to four Italian hospitals with objectively diagnosed ischemic stroke between 1 January 2006 and 15 April 2007 were included in this prospective cohort study.
Patients with cerebral venous thrombosis, sub-arachnoid hemorrhage or intracerebral bleeding on admission were excluded. All patients were assessed by a neurologist to determine the diagnosis of stroke (neurological deficits lasting >24 h) and its pathological and etiological subtypes [9]. On admission, stroke severity was assessed using the NIH Stroke Scale (NIHSS) [10]. Patients admitted within 3 h were evaluated for thrombolysis treatment according to Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST) criteria [11].
The four study centers provided standard stroke-unit care. All patients were monitored for blood pressure, temperature, glucose level, heart rate and blood gases in the first days after stroke.
Stroke risk factors
Data were collected regarding stroke risk factors: age, gender, history of hypertension (blood pressure of >140/90 mmHg at least twice before stroke), or patients already under treatment with antihypertensive drugs), history of diabetes mellitus (glucose level >126 mg/dl preprandial on second examination; glucose level >200 mg/dl postprandial; glycosylated hemoglobin >8.5%, or receiving hypoglycemic treatment), current cigarette smoking, past smoking (cessation <5 years before), history of hyperlipidemia (total cholesterol concentration >200 mg/dl and/or triglyceride concentration >140 mg/dl the day after admission or already receiving lipid-lowering therapy), history of symptomatic ischemic heart disease (i.e., proven myocardial infarction, history of angina or the existence of multiple lesions on the thallium heart isotope screen or evidence of coronary disease on coronary angiography), history of symptomatic peripheral arterial disease (i.e., intermittent claudication of presumed atherosclerotic origin; ankle/arm systolic blood pressure ratio ≤0.85 in either leg and at rest; or history of intermittent claudication with previous leg amputation, reconstructive surgery or angioplasty), atrial fibrillation, alcohol abuse (>300 g consumed per week), obesity (BMI ≥30) or previous stroke/transient ischemic attacks. White matter changes (leukoaraiosis examined on admission by computed tomography as ill-defined and moderately hypodense areas of ≥5 mm according to previously published criteria) were also evaluated [12]. Leukoaraiosis in the deep white matter was dichotomized into absent versus mild, moderate or severe.
Other baseline variables that were obtained at admission included: fasting serum glucose, fasting serum cholesterol (total high-density lipoprotein and low-density lipoprotein), platelet count, international normalized ratios, activated thromboplastin times, systolic blood pressure and diastolic blood pressure.
Patients or proxies were surveyed to obtain information on medicines used before the event (e.g., antiplatelet agents, prophylactic doses of anticoagulants, therapeutic doses of anticoagulants [i.e., heparin or warfarin], antihypertension drugs, antidiabetic drugs and statins). Treatments performed during hospitalization (e.g., antiplatelet agents, prophylactic doses of anticoagulants alone or in combination with antiplatelet agents and therapeutic doses of anticoagulants [i.e., heparin or warfarin] or thrombolytics [i.e., intravenous or intra-arterial]), were also recorded.
Evaluation of outcome
Patients were followed up prospectively either in person or over the telephone. Study outcomes were 3-month mortality or disability. Disability was assessed using a modified Rankin Scale (mRS) score. Stroke was defined as either nondisabling (mRS: 0–2) or disabling (mRS: 3–5) [13].
Negative outcome was defined as disabled or dead (mRS: 3–6). Time of occurrence and cause of death were recorded. Causes of death were divided into the following categories: neurological (e.g., recurrence of stroke, status epilepticus, edema or herniation), cardiovascular (e.g., myocardial infarction, heart failure, sudden death or other cardiovascular diseases) and other causes (e.g., pneumonia, cancer, pulmonary embolus and other causes).
Statistical analysis
Baseline characteristics of women and men were compared using χ2 and t-tests, as well as Fisher's exact text when necessary. A p-value of less than 0.05 was considered significant. Logistic regression analysis was used to assess whether the relationship between negative outcome and gender was confounded by other risk factors. Given the high number of variables evaluated in both analyses, the stepwise forward conditional model [14] was used for the logistic regression analysis. The stepwise forward conditional model automatically selected and excluded the variables that were nonsignificant. Data were analyzed with the SPSS/PC Windows package 13.0 [15].
Results
Distribution of risk factors & significant clinical differences between genders
A total of 1136 patients were included in this study; of these, 494 (46%) were female (Table 1). Women were statistically older compared with men (median years of age: 76.02 [± 12.93] vs 70.07 [± 12.95], respectively; p = 0.0018). There were no differences in pretreatment between genders regarding drugs for the treatment of hypertension, as well as statins, hypoglycemic treatments or anticoagulants.
Distribution of risk factors in genders.
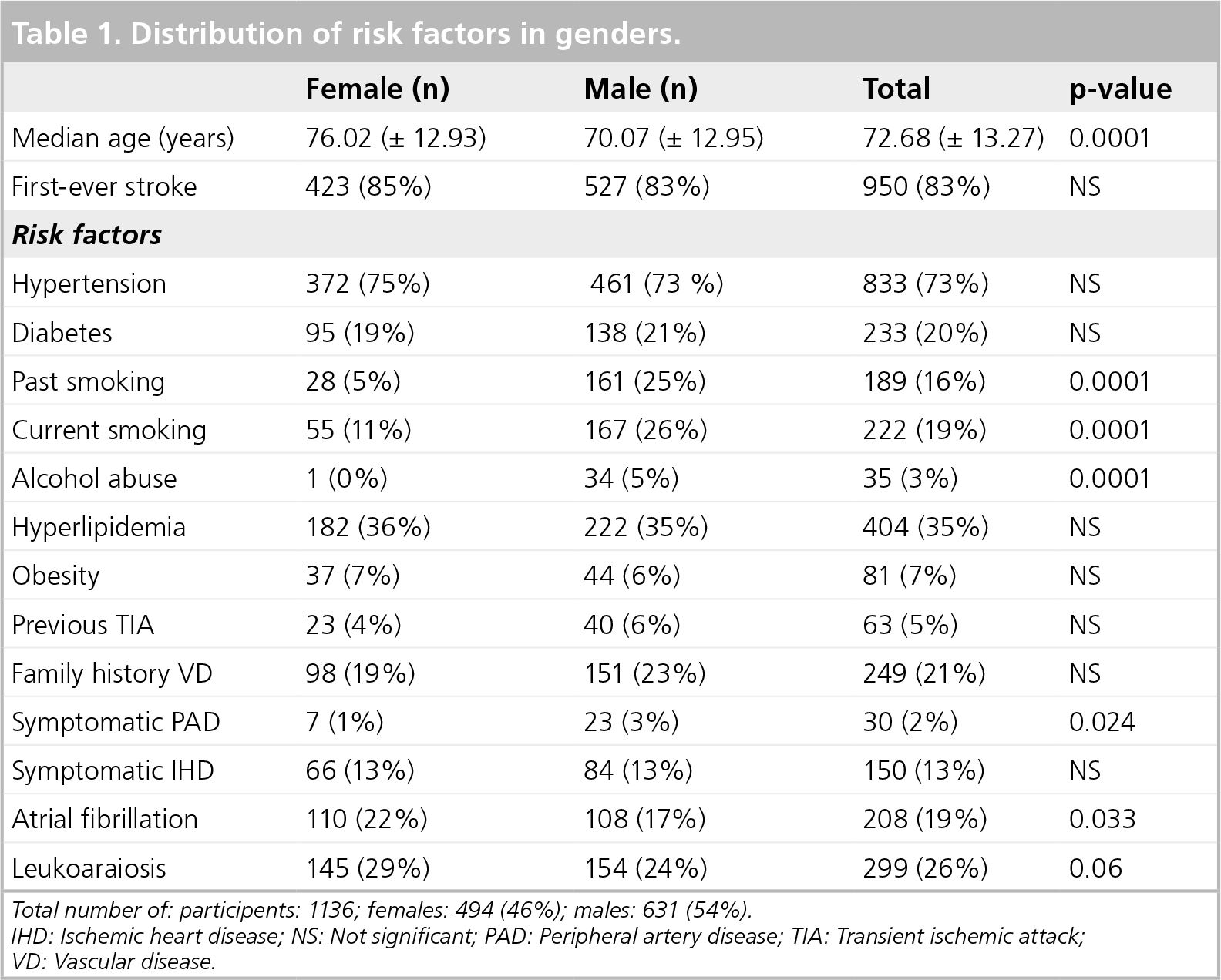
Total number of: participents: 1136; females: 494 (46%): males: 631 (54%).
IHD: Ischemic heart disease; NS: Not significant; PAD: Peripheral artery disease; TIA: Transient ischemic attack; VD: Vascular disease.
No difference in in-hospital thrombolysis treatment was observed. The distribution of stroke risk factors was different between males and females.
In fact, females had a statistically higher frequency of atrial fibrillation (110 [22%] vs 108 for men [17%]; p = 0.033) while males presented a statistically higher frequency of smoking (either past: 161 [25%] vs 28 for women [5%]; p = 0.0001; or current: 167 [26%] vs 55 for women [11%]; p = 0.0001). Men also demonstrated a significantly higher frequency of alcohol abuse (34 [5%] vs 1 for women [0%]; p = 0.0001).
Females had higher NIHSS scores at admission (9.4 [± 6.94] vs 7.6 for men [± 6.28]; p = 0.0018) (Table 2). Females tended to have a statistically higher frequency of cardioembolic stroke (153 [30%] vs 147 for men [23%]; p = 0.004). In addition, males tended to have more lacunar (146 [29%] vs 249 for men [39%]; p = 0.002) and atherosclerotic strokes (68 [13%] vs 123 for men [19%]; p = 0.01).
Significant clinical differences between genders.

Number of female participants: 494 (46%); number of male participants: 631 (54%).
mRS: Modified Rankin Scale; NIHSS: NIH Stroke Scale.
Gender influence on adverse outcome
At 3 months, seven patients were lost to follow-up, 326 patients (29.2%) were disabled and 129 had died (11.5%). The causes of death were neurological in 58 patients, cardiovascular in 24 patients, attributable to other causes in 20 patients and unknown in 27 patients. A total of 58 of these deaths were among women: 14 from neurological causes, 23 from nonneurological causes and 21 from unknown causes.
Female sex was found to be a determinant for negative outcome (n = 229 [51.4%] vs 264 for men [39.8%]; p = 0.001), as well as the presence of hypertension (n = 369 [81.1%] vs 460 for men [69.4%]; p = 0.0001) (Table 3).
Characteristics of the patients alive/nondisabled (mRS: 0-2) or dead/disabled (mRS: 3–6) (univariate analyis).

IHD: Ischemic heart disease; mRS: Modified Rankin Scale; NA: Not applicable; NS: Not significant; PAD: Peripheral artery disease; TIA: Transient ischemic attack; VD: Vascular disease.
In addition, the presence of atrial fibrillation was also found to be a determinant for negative outcome (n = 112 [24.6%] vs 106 [16.0%]; p = 0.0001) along with leukoaraiosis (n = 298 [26.6%] vs 129 [19.4%]; p = 0.0001). Hyperlipidemia was found to be a protective factor against negative outcome (n = 143 [31.4%] vs 259 [36.1%]; p = 0.009). First-ever stroke was found to be a protective factor for negative outcome (n = 944 [84.4%] vs 363 [79.8%]; p = 0.0001). Concerning nondicotomic variables, median age in years was found to be a strong predictor for negative outcome (n = 79.00 vs 70.07; p = 0.0001) (Table 3).
In addition, at logistic regression analysis, after entering age, high NIHSS score, history of diabetes, atherosclerosis and first-ever stroke, it was found that gender was not significantly associated with stroke outcome: age (odds ratio [OR]: 1.07; 95% CI: 1.05-1.09), high NIHSS- score (OR: 1.35; 95% CI: 1.30-1.41), history of diabetes (OR: 2.10; 95% CI: 1.38-3.19), atherosclerosis (OR: 1.84; 95% CI: 1.15-2.93) and first-ever stroke (OR: 0.50; 95% CI: 0.31-0.79).
Discussion
This study evaluated the existence of gender differences in clinical presentation, management and outcome in a large sample of Italian stroke patients. Female gender was not an independent factor for negative outcome after adjusting for confounding variables, thereby confirming recent findings of other authors [7].
In accordance with other studies, female stroke patients were, on average, older then men in this study [6,16,17]. In addition, women presented both more severe neurological deficits and pre-and post-stroke disabilities [6]. Eriksson et al., observed an impaired level of consciousness at admission in women, which is an expression of large cerebral lesions [18]; in addition, another recent systematic review by Appelros et al. found that stroke tended to be more severe in women, with a 1-month case fatality of 24.7% compared with 19.7% for men [19].
In our study, no data were collected on the type of discharge from hospital. However, other studies have confirmed that many women spend the last years of their lives in nursing homes, but this is not necessaily due to stroke. Their institutionalization can be due to either higher prestroke disabilities or stroke itself [6].
Regarding vascular risk factors, the higher presence of atrial fibrillation in the women in this study has already been evidenced by Marini et al. [20]. Considering that women with atrial fibrillation tend to have higher annual rates of thromboembolism than men (3.5 vs 1.8%; adjusted rate ratio: 1.6; 95% CI: 1.3–1.9), it can therefore be said that female sex is an independent risk factor for thromboembolism. This fact should influence any decision concerning whether to use anticoagulant therapy in women with atrial fibrillation [21]. In addition, in our study, men tended to have other risk factors, such as peripheral vascular disease, were more likely to be smokers and to abuse alcohol more often [22].
In our study, there were no data regarding diagnostic investigations. A recent study has demonstrated that women tend to undergo less diagnostic workup than men [16], while other studies have failed to demonstrate this [7,23]. It is likely that in-hospital stroke management for the two genders has been more or less uniform over the last few years owing to an increasing awareness of the ‘petite difference’ [22]. In fact, in our study there was no in-hospital treatment difference regarding gender [23]. This was especially true when considering thrombolysis treatment.
Nonetheless, the principle problems for women regarding stroke care begin before admission. It has been shown in a recent article that women had a 10% lower chance of being admitted within the first 3 h compared with men (OR: 0.902; 95% CI: 0.860-0.945; p < 0.001) [24]. This ‘just-in-time access’ to treatment further decreased in elderly women.
However, for patients admitted within the 3- h time window, the administration rate of thrombolysis was the same for women and men (OR: 0.915; 95% CI: 0.809-1.035; p = 0.156).
Much of the admission delay can be attributed to the ‘surviving spouse disadvantage’ [24]. This is one of the numerous factors that are believed to interact in determining the gender differences in clinical outcomes of stroke patients [25].
In this study, the variables that were independent risk factors for negative outcome included high NIHSS score, history of diabetes and atherosclerosis. These data are not particularly surprising, given that a high NIHSS score is an expression of severe stroke and an extension of cerebral infarct [26,27]. In our study, women had more severe strokes than men, and stroke severity adversely affected outcome; however, it must be remembered that this should not result in the conclusion that gender, ipso facto, is an independent factor for outcome.
In conclusion, the two genders had different pathophysiologies of stroke. These differences should be taken into account during diagnostic workup and when treatments are being planned. However, in our study, female gender was not an independent factor for negative outcome.
Future perspective
Life expectancy is longer in women compared with men. Lifetime epidemiological studies have reported increases in stroke severity and fatal stroke in women, causing death in one in six women compared with one in 12 men. In patients who survive from stroke, women will have a higher probability of being disabled, as well as being discharged to nursing homes. This means that the overall burden of stroke is becoming a prevalent female health problem, with enormous costs for healthcare systems worldwide. This report aims to alert physicians working in stroke prevention and stroke care in women.
Executive summary
Female stroke patients tend to be older compared with males.
Females tend to have a higher NIH Stroke Scale score at admission, and a higher modified Rankin Scale score at discharge than males.
Females tend to have a higher frequency of atrial fibrillation than males.
No difference in in-hospital stroke treatment was observed between genders.
In the logistic regression analysis, female gender was not an independent determinant of negative outcome.
Footnotes
Acknowledgements
We are grateful to Alessandra De Leo and Elisa Manfredi for their contribution to collecting data and following patients at the Research Center of Varese, Italy.
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.