
Abstract
The diagnosis and treatment of various medical conditions requires patients to wait for results that are potentially threatening to their wellbeing (e.g., breast biopsy results, pregnancy test results after fertility treatment and genetic screening outcomes). Little research has been carried out to document the psychological processes that unfold during such waiting periods. The aim of the present study was to document the course of anxiety, depression, positive affect and coping during the waiting period before a pregnancy test result in fertility treatment. Using a daily record-keeping chart designed for fertility treatment, 61 women undergoing IVF were monitored daily for emotional reactions (e.g., anxiety, depression and positive affect) and coping during 7 days of active treatment (stimulation), 7 days of waiting to find out whether a pregnancy was achieved (waiting) and 4 days of reacting to the pregnancy test results (outcome). The stimulation stage of treatment was characterized by positive affect with a lesser degree of anxiety, whereas the predominant emotions in the waiting stage were a combination of positive affect and anxiety symptoms versus depression. From the pregnancy test day onwards, the predominant emotion was depression. There was a significant increase in coping activity between the stimulation and waiting stages, with variable effects across coping strategies. It was concluded that whilst medical waiting periods have a clearly defined emotional trajectory, the coping pattern is less differentiated. This may explain why waiting for medical test results is so demanding. Healthcare professionals can assist their patients by facilitating coping strategies that better fit the demands of the waiting period and by offering support once outcomes are known.
Waiting for the results of medical tests and procedures can be a stressful experience for patients since the results can have significant implications for their future wellbeing. The aim of the present study was to describe the emotional reactions (anxiety, depression and positive affect) experienced by women in the waiting period between embryo transfer and pregnancy test during IVF treatment.
According to Osuna, psychological stress reactions build from the start of any waiting period and increase as a function of the time the individual has been waiting [1]. Lazarus and Folkman identify other characteristics that make situations stressful, and these are particularly applicable to medical waiting periods [2]. First, most medical waiting periods occur in relation to waiting for an outcome that can have negative consequences for the patient and their loved ones, meaning that the outcome of the tests really matter. Second, there is little, if anything, patients can do to change or control the outcome of the test they have already taken; any pathophysiology will have already occurred and the results will only confirm whether and to what extent the disease is present. Third, waiting periods provide little objective information to allow patients to accurately gauge the likelihood of positive or negative outcomes. The results of tests are therefore unknown and unpredictable, causing high levels of uncertainty that are difficult to cope with. Certainty that an unpleasant event will occur allows one to engage in anticipatory coping in order to help one deal with it when it eventually does occur [2], whereas uncertainty provokes rumination and intrusive thoughts as patients vacillate repeatedly between consideration of one possible outcome and then another. Such rumination may hamper anticipatory coping. It has been argued that individuals prefer to know what is going to happen, even (or especially) when that event could be unpleasant [3].
Folkman and Lazarus propose a close link between appraisals, emotions and coping during stressful situations [2]. Anticipatory emotions are those experienced before the outcome is known and could include threat (e.g., tension or worry) or challenge (e.g., encouraged or happy) depending on whether one is imagining a positive or negative outcome. Furthermore, there are emotions that manifest once the outcome is known (e.g., sadness or joy) depending on the nature of that outcome. With regard to coping, as the outcome of the medical tests or procedures for which patients are waiting cannot be changed or controlled, theory suggests that trying to change the situation would be ineffective and unhelpful. Instead, the individual would rely primarily on strategies aimed at regulating the negative emotions associated with medical waiting periods (i.e., the ‘goodness-of-fit’ hypothesis) [2–6]. Such emotion-focused efforts may include avoidant strategies such as distraction, and approach strategies such as acceptance or positive redefinition of the situation.
Despite the pervasiveness of waiting periods in medicine, very little research attention has been devoted to the delineation of emotional and coping processes that unfold at these times. However, what research does exist suggests that patients waiting for the results of medical tests or procedures, such as breast cancer diagnosis and cardiac catheterization, find the waiting period stressful, experience anxiety at clinical levels [7], and become more anxious as the day of diagnosis or treatment approaches [8–10].
With regards to coping, qualitative and quantitative studies of patients waiting for medical tests and procedures suggest that patients do report emotion-focused coping strategies, such as denial, venting, distraction, avoidance, depressive coping and resignation/acceptance during medical waiting periods [7,9,11–13]. However, although these studies give an insight into emotion and coping during medical waiting periods, the emotions examined were limited to negative ones (e.g., distress, anxiety or depression) and assessment occurred only twice at most. This means that the findings do not comprehensively document the dynamic nature of coping and emotion over the extended duration of most medical waiting periods (i.e., often weeks) compared with less stressful stages of treatment. In order to understand and support patients during medical waiting periods, more in-depth analysis of emotions and coping at this time is needed.
In the present study, a longitudinal and indepth assessment of women's emotional reactions and coping during the waiting period between embryo transfer and pregnancy test in IVF was conducted. IVF is a fertility treatment that can help couples with a range of fertility problems to achieve a pregnancy. Pharmacologic interventions in the first stage of treatment (stimulation) cause multiple follicles to mature, from which oocytes are retrieved, placed in a culture dish and fertilized with sperm. If fertilization is successful then embryos (typically two) are transferred to the uterus. The second stage of treatment (waiting) then begins, until women can take a blood test in order to determine whether they are pregnant. The objective probability of success per initiated cycle of IVF is 20–25% [14], meaning that the majority of women will not become pregnant during an IVF treatment cycle. IVF is an ideal context in which to study the medical waiting period. First, it has all the elements associated with appraising a situation as stressful (i.e., uncontrollable, unpredictable and potentially negative). Second, the experimental context is homogeneous across patients (e.g., procedures, success rates or length of treatment) so that all patients are coping with the same situation. This is not always the case with other medical conditions that vary in severity or prognosis. Third, the potential for a desired positive outcome (i.e., pregnancy) means that people may also experience positive emotions whilst waiting. Fourth, the initial stage of treatment (stimulation) is considered to be relatively low-stress by patients, therefore providing an inbuilt control for the emotions and coping of the more stressful 2-week waiting stage [15].
In the present study, patients monitored emotional reactions and coping daily during the stimulation and waiting stages. Proponents of daily monitoring methodology argue that this is a more comprehensive method of assessing responses to a situation compared with asking individuals to assimilate their responses over a protracted period of time or retrospectively [16], as has been carried out previously [17]. In addition, daily monitoring has an advantage over pre- and post-test experimental designs because it captures the dynamic nature of the ongoing coping process between those assessment points.
In line with theoretical predictions [2] and prior research [18], it was expected that there would be significant decreases in women's reports of positive reactions and significant increases in negative reactions in the waiting compared with the stimulation stage. It was also expected that more coping effort would be employed in the waiting stage compared with the stimulation stage, with particular increases in emotion-focused coping in order to deal with the more negative emotionality engendered by uncertainty. Although the aim of this paper is to delineate emotions and coping processes over time during IVF treatment, a full explication of the links between these constructs using frequent assessments is beyond the scope of the current article.
Method & materials
Participants
The final sample included 61 women who were about to begin IVF treatment at the assisted reproduction unit of a large urban hospital in the UK from September 1995 to June 1997. The selection criteria for the study were that women were accepted onto the IVF program, started and completed the IVF cycle, spoke and understood English sufficiently to complete study materials and that pregnancy test outcome was known.
The mean age of the women was 33.28 years (standard deviation [SD]: 3.61) and all but one had completed at least some secondary education. The majority (82.0%; n = 50) were employed. In terms of reproductive history, the women had been infertile for an average of 7.36 years (SD: 3.0), more than half (62.3%; n = 38) were experiencing primary infertility (i.e., had never had a pregnancy, whether it resulted in an ectopic pregnancy, abortion, miscarriage or live birth) and approximately a third (32.8%; n = 20) had previously experienced one or more cycles of IVF treatment. IVF had previously been successful for two of these women.
Women in this study were recruited from 287 women with scheduled appointments at the IVF clinic, of whom 211 (75.3%) attended their appointment and were interviewed as potential participants. Of these, 150 women were not included in the final sample because: their IVF cycle was not yet scheduled (10.9%; n = 23); they did not meet medical requirements for IVF (18.0%; n = 38); their cycle was cancelled before the pregnancy test owing to poor response or failed fertilization (14.22%; n = 30); they were not invited into the study after interview due to not meeting language or education criteria (9.95%; n = 21); or they did not complete all study materials (13.27%; n = 28). Ten women (4.74%) were not included in the final sample because full information about their biological variables was not available.
Materials
Daily record-keeping chart
Daily emotional reactions during IVF were monitored using a modified version of the daily record-keeping (DRK) chart that was designed for patients undergoing fertility treatment [19]. The emotional subscale of this chart contains affective reactions that are averaged to produce anxiety (e.g., tense, nervous and worried), depression (e.g., angry, frustrated and sad) and positive affect (e.g., happy, content and fulfilled) ratings. Emotional reactions were rated on a scale of 0 (not at all) to 3 (extremely), with higher scores representing greater emotion. The psychometric properties of these subscales were examined in two previous infertility studies [19,20] in which it was found that: internal reliability for the subscales was high; the sum of the items correlated moderately with other measures of distress; the subscale total fluctuated across the treatment cycle in a manner consistent with expected changes; and participants reported that the scale was neither difficult nor stressful to complete. In the present study, reliability coefficients were also high (0.77, 0.82 and 0.77 for anxiety, depression and positive affect, respectively). The women reported optimism regarding the imminent pregnancy test outcome on the same scale.
The women also indicated their use of five coping strategies from Stone and Neale's daily coping measure [16]. ‘Distraction’ referred to turning attention to other activities; ‘positive redefinition’ was defined as trying to view the treatment in a different light that made it more bearable; ‘problem-focused’ coping involved making an effort to try to positively influence the outcome of treatment; ‘seeking emotional support’ involved turning to loved ones and/or professionals for support; and ‘acceptance’ referred to accepting that nothing could be done. Strategies were rated on a scale of 0 (not used at all) to 3 (used frequently), with higher scores representing greater use of the strategy.
Instructions on the reverse side of each DRK chart explained when to complete the form (same time every day, preferably in the evening) and how to use the rating scales. Each sheet of the DRK chart collected 7 days of daily monitoring (i.e., seven columns). In each column, women filled out the day and date of treatment, and whether they had received a medical intervention that day (e.g., stimulation or oocyte retrieval). In this study, we report on reactions during three stages of one IVF treatment cycle. The stimulation (active) stage of treatment was the last 7 days of ovarian stimulation when women receive injections and undergo blood tests and ultrasound scans. The waiting stage was the last 7 days of the waiting period prior to the pregnancy test. Emotions and coping on the day of the pregnancy test and 3 subsequent days were also reported, allowing examination of the impact of the pregnancy test (outcome stage). Women completed the DRK chart on a daily basis and mailed the form every week in the provided stamped, preaddressed envelopes.
Treatment outcome
The outcome of IVF was the result of a blood test 14 days after embryo transfer (i.e., pregnant or nonpregnant), which was determined by a review of the women's medical records.
Procedure
The study received ethical approval from Bro Taf Local Health Authority, which receives applications from medical clinics governed by the NHS in the area in which participants were recruited. Approximately 3 months before commencing IVF (mean: 2.84 months; SD: 1.58), women had an initial appointment with the medical consultant, at which time medical procedures for IVF were outlined and preliminary blood tests were carried out in order to assess suitability for treatment. A complete description of the study and its requirements was given to patients at this time. Those interested in participating signed a consent form, were interviewed to obtain demographic and medical information and were provided with DRK charts to complete at home. The women were asked to complete questionnaires privately each day in the evening just before bed, and to recall emotions and coping experienced that day. Women underwent the routine IVF treatment protocol for the clinic and returned DRK chart sheets in the prepaid envelopes provided at the end of each 7 days of monitoring.
Data analysis
Data were examined to determine suitability for multivariate analyses. Missing values (<4 days) were replaced with group means according to pregnancy test result (i.e., pregnant or nonpregnant). Trend analysis was used to examine differences across the 18 days of treatment (stimulation: 7 days; waiting: 7 days; and outcome: 4 days). In the follow-up tests, linear, quadratic and cubic polynomials were fitted to emotions (e.g., anxiety, depression and positive affect) and coping strategies (e.g., distraction, positive redefinition, acceptance, problem-focused and seeking support). A probability value of p < 0.05 was considered significant.
Results
Nine of the 61 women had a positive pregnancy test (14.75%).
Emotional reactions
Figure 1 shows mean anxiety, depression and positive affect in the last 7 days of ovarian stimulation (stimulation stage; S1–S7), the last 7 days of the waiting period (waiting stage; W1–W7) and the pregnancy test and 3 subsequent days after the pregnancy test (outcome stage; P1–P4). Trend analysis revealed that the day main effect was significant for anxiety (F[,1020]: 11.54; p < 0.001; mean square error [MSE]: 0.25) and the most significant trend for this emotion was cubic (F[1,60]: 31.97; p < 0.001; MSE: 0.45), showing a gradual increase in anxiety leading up to the day of the pregnancy test, a precipitous decline when results were known and slower decrement on the fourth day after the pregnancy test. The day main effect was significant for depression (F[17,1020]: 27.52; p < 0.001; MSE: 0.25) and the most significant trend was quadratic (F[1,60]: 43.95; p < 0.001; MSE: 0.61), showing that depression was stable for most of the cycle until the day of the pregnancy test, when a significant increase occurred followed by some remission by the fourth day of the outcome stage. The day main effect for positive affect was significant (F[17,1020]: 9.99; p < 0.001; MSE: 0.14). The most significant trend was linear (F[1,60]: 27.52; p < 0.001; MSE: 0.75), showing that positive affect declined consistently across the days of the cycle. The nonoverlapping error bars in Figure 1 show that the predominant emotion in the stimulation (active) stage was positive affect followed by anxiety, whereas the predominant emotions in the waiting stage were a combination of positive affect and anxiety symptoms versus depression (until the day before the pregnancy test). Once the results of treatment were known, the main emotion in this largely unsuccessful sample was depression.

Anxiety, depression and positive affect during the stimulation, waiting and pregnancy outcome stages of IVF.
Until the pregnancy test, pregnant and nonpregnant women would be comparable in terms of the nature of the stressor (i.e., uncertainty regarding treatment success). This is reflected in comparable optimism about the imminent pregnancy test result in pregnant and nonpregnant women in the 7 days prior to the test. This varied from 0.48 to 0.50 and from 0.43 to 0.67 for the nonpregnant and pregnant groups, respectively. By contrast, after the results of the pregnancy test were known, the emotional experience becomes differentiated by pregnancy outcome. To illustrate this differentiation, Table 1 shows means and SDs for anxiety, positive affect and depression on the day of the pregnancy test and the subsequent 3 days for pregnant and nonpregnant women.
Means (standard deviations) for anxiety, depression, positive affect and overall coping effort in pregnant and nonpregnant women on the day of the pregnancy test (P1) and 3 days thereafter (P2–P4).
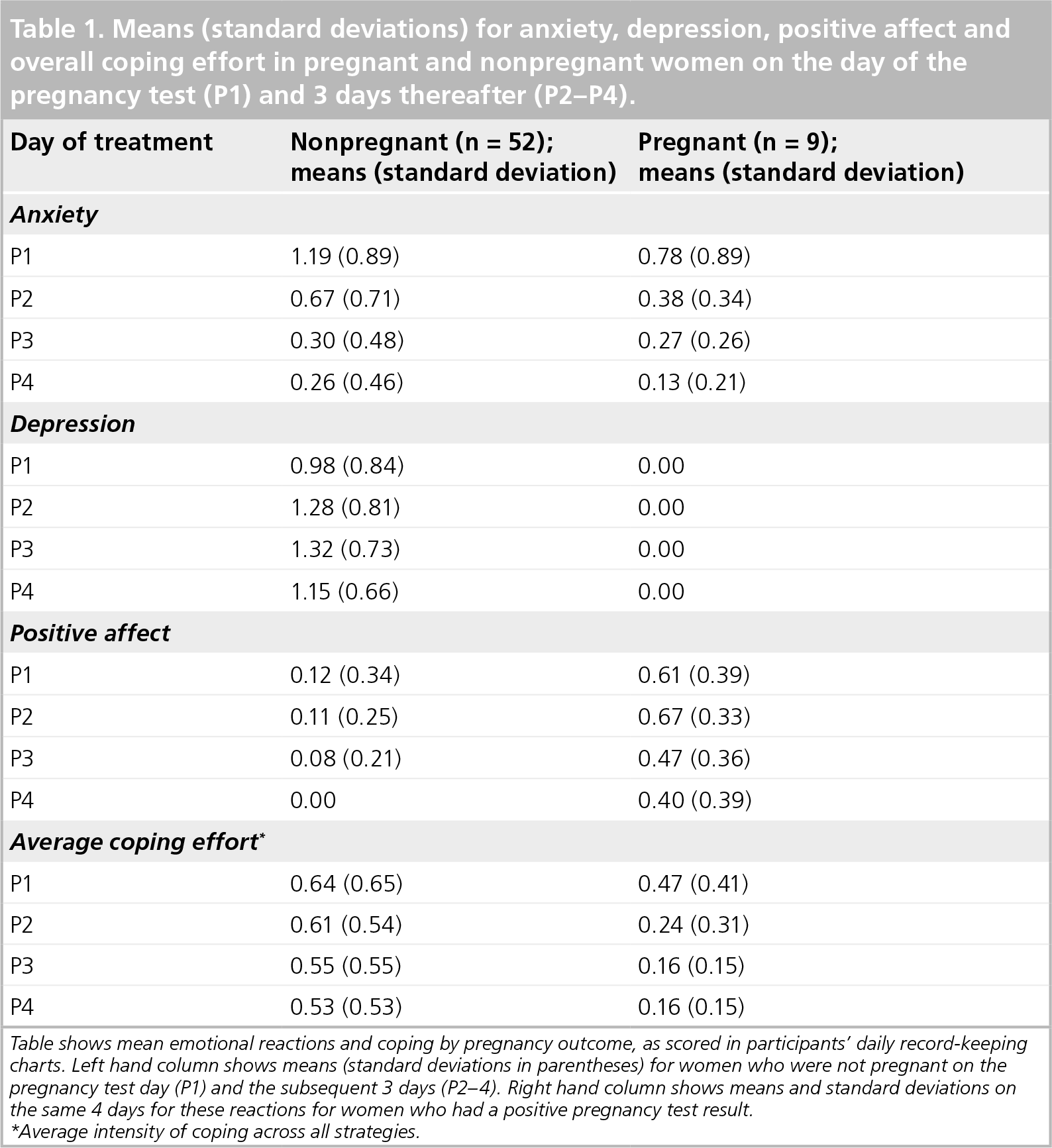
Table shows mean emotional reactions and coping by pregnancy outcome, as scored in participants' daily record-keeping charts. Left hand column shows means (standard deviations in parentheses) for women who were not pregnant on the pregnancy test day (P1) and the subsequent 3 days (P2–4). Right hand column shows means and standard deviations on the same 4 days for these reactions for women who had a positive pregnancy test result.
Average intensity of coping across all strategies.
Coping
Figure 2 shows coping in the last 7 days of ovarian stimulation (stimulation stage; S1–S7), the last 7 days of the waiting period (waiting stage; W1–W7) and the pregnancy test and 3 subsequent days after the pregnancy test (outcome stage; P1–P4). The day main effect for seeking support was significant (F[17,1020]: 4.11; p < 0.001; MSE: 0.38), and the most significant trend was cubic (F[1,60]: 10.11; p < 0.01; MSE: 0.60). The day main effect for acceptance was significant (F[17,1020]: 6.93; p < 0.001; MSE: 0.38), with a significant linear upward trend (F[1,60]: 27.14; p < 0.001; MSE: 1.42). The day main effect for distraction was significant (F[17,1020]: 2.60; p < 0.001; MSE: 0.50), with a significant cubic trend (F[1,60]: 6.22; p < 0.05; MSE: 0.62), demonstrating that distraction decreased linearly during treatment, with fluctuations after the pregnancy test. The day main effect for problem-focused coping was significant (F[17,1020]: 2.94; p < 0.001; MSE: 0.29), with the most significant trend being cubic (F[1,60]: 3.96; p < 0.05; MSE: 0.41). The trend showed an increase during the waiting stage, followed by fluctuations after the pregnancy test result. The day main effect for positive redefinition was not significant (F[17,1020]: 1.01; p < 0.44; MSE: 0.24).

Coping during the stimulation, waiting and outcome stage of IVF.
Discussion
The results of this study suggest that medical waiting periods have a clearly defined emotional trajectory; however, the results also suggest that the coping pattern is less differentiated at this time. Medical waiting periods involve both the demands of waiting itself and the anxiety engendered by the unknown test result and its possible consequences for wellbeing. Undifferentiated but elevated coping activity may simply reflect women's concerted efforts to deal with these demands using whichever strategies can be deployed from their coping repertoire. Health professionals can assist their patients by facilitating coping strategies that better fit the demands of the waiting period and by offering support once outcomes are known.
The strengths of this longitudinal evaluation are that daily emotions and coping were reported during a naturalistic, evolving and multiphasic stressor that was homogeneous across patients. This allowed us to capture the dynamic nature of emotions and coping during the waiting period, and to delineate profiles during this period versus the active (stimulation) and pregnancy test (outcome) stages of treatment. The prospective nature of assessment, and its frequency, meant that self-report was not contaminated by assimilation processes or recall bias, and our use of the last 7 days of stimulation and waiting and the first 4 days of pregnancy outcome meant that we could anchor daily reactions to the start and end of each stage. The sample size and repeated measures design yielded good power (p > 0.88 based on final sample size and power parameters [21,101]) to detect any significant effects, and follow-up analyses allowed the characterization of trends across emotions and coping strategies. Finally, the outcome of treatment was verified by medical chart review, allowing comparison of emotional reactions between positive and negative outcome (although the modest success rate precluded further analysis of these descriptive data).
The IVF waiting period was associated with a well-defined and, for the most part, nonoverlapping sequence of emotional reactions that were in keeping with treatment demands. IVF represents an opportunity to achieve a long-desired pregnancy, and, in the initial active stage of treatment (stimulation), this is reflected in relatively high positive emotions and low negative emotions. However, the uncertainty of waiting for the pregnancy test result was characterized by increasing anxiety and depression as the day of the pregnancy test approached. Lazarus and Folkman maintain that the imminence of an important event is one of the critical dimensions that can make people appraise situations as stressful, and our results support this contention [2]. However, it should be noted that negative emotions did not exist in isolation of positive emotions in the present study. In fact, the emotional profile whilst waiting was a combination of anxiety and positive emotions. Leiblum
One may question whether early optimism is a risk for higher rebound distress when treatment fails, and whether efforts should therefore be made to temper optimism in active (stimulation) stages of treatment. However, it has been shown that reducing optimism by providing veridical feedback regarding the likelihood of pregnancy only creates more distress at the point of giving feedback along with the same amount of distress at the time of actual failure, because the medical feedback available is not failsafe [23]. Optimism may also be protective because positive states may sustain coping processes in the face of ongoing stress and associated negative emotions. Even in the most trying of circumstances (e.g., caregiving and bereavement), positive affect is evident, coexists with negative affect and may have a vital role in motivating people to renew coping efforts during a chronic, persistent and distressing experience [24–26]. We suspect that it may be unwise to interfere with patients' optimism, especially as even unrealistic optimism may be adaptive in instances where negative feedback is given or the individual is threatened [27].
The pregnancy outcome stage was associated with a precipitous decline in anxiety and sustained depressive symptoms once pregnancy outcome was known. This pattern supports the work of Folkman and Lazarus regarding the nature of anticipatory versus outcome emotions, and confirms that different situational demands have different emotional corollaries [2]. The implication of this emotional profiling is that interventions to support patients must be as dynamic as the emotions patients are likely to experience. Moreover, the active elements of an intervention (e.g., stress management versus catharsis) need to address the specific emotions (e.g., anxiety versus depression) elicited by the different situational demands across medical experiences.
The interplay between coping and emotions affords another entry point by which to intervene and so assist people during medical waiting periods. The stimulation and outcome stages of treatment were associated with higher use of some coping strategies and reduced use of others, suggesting differential selection and implementation. There is much evidence to show that people do adapt their coping strategies in order to fit the demands of the situation and that such goodness-of-fit is necessary for effective coping and management of distress [17,28,29]. By contrast, there was considerable overlap in strategy use during the waiting period in the present study, and no one particular strategy asserted itself except for an increase in seeking support in the last few days before the pregnancy test. This diversity of coping is surprising at one level because, of the three stages observed (stimulation, waiting and outcome), the waiting period is most defined in terms of what women are coping with (i.e., uncertainty). They neither know which outcome they will need to cope with (as they do at the outcome stage) nor can do anything to increase the likelihood of becoming pregnant (as they can do in the stimulation stage). As such, coping theory would prescribe the use of emotion-focused strategies such as distraction, positive redefinition and acceptance during the waiting stage [2,4–6]. While these were used, they were not used exclusively, and problem-focused coping (considered less adaptive in such situations) was used more than positive redefinition.
Lazarus and Folkman proposed that coping can become ‘immobilized’ in situations where one cannot predict the outcome, because one does not know whether to deploy strategies for coping with a positive or negative outcome [2]. However, the findings of the present study suggest more of a state of confusion in the waiting stage in which all strategies were tried rather than none, and this could have implications for wellbeing, as indicated by the increase in negative emotions during the waiting stage. However, the causal link between coping and emotions (or vice versa) cannot be ascertained from the present experimental design, since emotions and coping were rated simultaneously on any given day. We believe, however, that future research should continue to explicate the causal links between coping strategies and emotional reactions [4–6], and we hope to contribute to this in a future paper.
We have described emotion and coping as they occur spontaneously during a specific medical waiting period, that of IVF. We have demonstrated that women will be anxious during treatment despite efforts to cope and that although treatment affords them the opportunity for success, meaning that positive affect is evident, many will be emotionally hurt by a negative outcome. Does the reactive pattern of negative emotions during waiting and disappointment at failure warrant intervention in the waiting period? If so, what form of intervention should take place? The answer lies in the observed pattern of daily observations, which suggested some differences between women's spontaneous use of individual strategies and those that theory would prescribe as being an effective means of coping in situations characterized by uncertainty. Intervention should therefore be aimed at bolstering women's use of such coping strategies known to be effective at such times. Figure 2 shows that women spontaneously used distraction techniques during much of the treatment. Therefore, supporting the consistent use of these strategies with a distraction coping intervention may be as advantageous in IVF as it was for patients waiting for genetic screening results [12,30]. An intervention to promote positive reappraisal coping [31] may also be of benefit. This should be an adaptive strategy because it encourages women to redefine the IVF waiting period more positively, thereby helping to sustain positive emotions.
Both the distraction and positive reappraisal interventions are self-help coping interventions, which may be an appropriate method of intervention delivery for women after the result of their pregnancy test. The precipitous decline in seeking social support at this time may suggest that women withdrew from others after finding out the result of the pregnancy test, which may be a contraindication for face-to-face intervention, at least during the early days post-treatment failure. Furthermore, it should be kept in mind that the stressor in question (i.e., waiting for the pregnancy test) is relatively short-lived, meaning that any intervention has to be easily and quickly administered so that its effects are realized at the critical time. In other words, interventions should fit both the demands of the situation and the practical realities of the medical context. We believe that self-help coping interventions are a useful tool for supporting patients during challenging times in medical experiences.
The main weaknesses of this study were potential reactivity to the monitoring process and reliance on daily monitoring, which required compliance from women in terms of completing the DRK chart each day. Furthermore, it is possible that women might have had knowledge of their treatment outcome prior to the purported day of the pregnancy test (e.g., due to spotting [32] or a home pregnancy test). First, however, the pattern of emotional reactions was clearly consistent with the expected demands and stages of treatment. Positive affect, anxiety and depression were highest in the stimulation, waiting and outcome phases, respectively, as would be predicted by theory [2]. Second, the importance of monitoring reactions daily was stressed to the women at the start of the project and in the instructions on the DRK charts. Completed DRK charts were received weekly as instructed, indicating compliance, and although it is possible that women completed all ratings on the day they mailed their weekly form, there was no reason for them to do so; they could just as easily drop out of the study since we were not part of the clinical team. Finally, data published elsewhere demonstrate that women's reactions to the different stages of treatment were consistent according to the demands of treatment at those stages (e.g., physical reactions consistent with drug administration [15]) and that women reported more negative reactions on days that they received what they perceived as negative feedback than they did when receiving positive or no feedback [23]. In short, we believe that the DRK chart shows sensitivity and specificity across the IVF cycle, and we do not believe that the results obtained in the present study are influenced by methodological flaw.
A second limitation is that we observed reactions in a single medical waiting context, and replication in other contexts (e.g., genetic testing and cancer diagnosis) would be valuable. The fertility context differs from some other medical experiences, because the desired outcome is a positive addition to women's pretest state (i.e., pregnancy), whereas in other medical experiences a positive outcome represents a return to baseline state (i.e., absence of disease). Waiting for the removal of a potential harm may differ from waiting for the addition of a potential benefit, and this could make the implications of waiting periods in fertility treatment different from those in other medical experiences. However, past research is suggestive of more similarity than difference across medical contexts; extant research shows that breast cancer and cardiac catheterization patients are more anxious in assessments nearer to diagnosis or treatment [8–10].
Data collection in the present study took place between 1995 and 1997 from patients who had been infertile for a long time and under treatment in a clinic that had a long waiting list and a low success rate with techniques available at that time [33]. It is important to consider whether such issues would bias the conclusions we draw from the data and would be relevant to today's patients. We firmly believe that the results of the present study are valid since the differentiation of positive and negative emotions are as expected on the basis of theoretical proposals regarding negative anticipatory and outcome emotions and positive emotions [2] across the changing demands of this experience. There is also no reason to expect results to differ if women were older or infertile for a shorter time because these characteristics do not predict the uncertainty of waiting for results; IVF success can never be guaranteed. Indeed, female age and number of years of being infertile were not significantly related to distress during the waiting period in the present study (range = 0.010 to −0.177; average: 0.048). Finally, although time-related demographics and clinical characteristics might differ between our sample and contemporary samples, there is no reason to believe the psychological makeup and expectations of women would be different today than at the time of data collection. Indeed, mean trait anxiety scores for women in this sample [34] were 39.95 (SD: 10.02), similar to that of a more recently collected dataset in the same unit (mean: 38.21–40.07) [DEBORAH LANCASTLE, UNPUBLISHED DATA, 2005-2006] and to published norms for general medical patients (mean: 41.33) on the Spielberger State-Trait Anxiety Inventory Trait scale [35].
Waiting for potentially threatening medical test results will always be demanding. The importance of the outcome and uncertainty surrounding what that outcome might be engenders dynamic emotional reactions linked to the threat or promise of the eventual result. The demands of the medical waiting period are reflected in increased coping effort, but clear differentiation among strategies was not present. Interventions that sustain coping efforts would be a worthwhile endeavor that might bolster psychological wellbeing when dealing with this or other medical waiting periods [30,31].
Future perspective
We expect that in the next 5–10 years, health practitioners and researchers will move away from one-size-fits-all support interventions to tailored interventions that address the demands of specific medical situations. One experience common to almost all people is that of waiting for potentially threatening medical test results. Although many people consider this stage of a medical experience to be the most demanding (and our prospective results support this view), it is paradoxically when patients are least likely to be receiving formal interventions owing to the practical and cost implications of organizing support during the brief weeks of a medical waiting period. In such circumstances, patients are often told to ‘stay positive’ or ‘not think about it’ without evidence that doing so would help, or guidance about how one should go about achieving these states. We believe the future will bring much more focus on generating brief, selfadministered and cost-effective evidence-based interventions for these types of micro-healthcare situations, to bring about a more optimal treatment environment. Research by the authors and others [30,31] shows that theoretically derived coping interventions for the medical waiting period are well received by patients and have positive effects on their wellbeing.
Executive summary
Waiting for diagnoses and medical test results causes high levels of uncertainty that can be distressing and difficult to cope with.
The results of medical tests can have significant implications for future wellbeing.
Results, such as breast biopsy results, pregnancy test results after fertility treatment and genetic screening outcomes, are potentially threatening to patients' physical and emotional wellbeing.
The results of such tests are perceived as unpredictable until the day they are confirmed, even when people have received feedback regarding risks for particular outcomes.
Not knowing what one might be eventually coping with makes it difficult to prepare oneself effectively for the outcome, further heightening distress.
Little research has been carried out to document the psychological processes that unfold during medical waiting periods.
A total of 61 women undergoing
Ratings were made during 7 days of active treatment (stimulation stage), 7 days of waiting in order to ascertain whether or not they were pregnant (waiting stage) and the pregnancy test day plus 3 days (outcome stage).
The imminence and outcome of tests had a profound effect on emotions.
Demands of treatment had a significant emotional impact, especially in the 2-week waiting period before pregnancy test results were given.
Women reported cautious optimism (i.e., positive affect and anxiety) when actively involved in the medical interventions (e.g., hormone stimulation) that are required in order to have a chance at becoming pregnant.
By contrast, the 2-week waiting period before finding out whether treatment had been successful was characterized more by anxious optimism because women became increasingly anxious (e.g., tense and worried) and reported more intense depressive feelings (e.g., sad and frustrated) as the day of results approached, despite relatively unchanged positive affect scores.
In this largely unsuccessful sample (85% nonpregnant), the results of the pregnancy test were associated with a precipitous decrease in anxiety and a sustained level in depressive feelings, consistent with expected patterns for anticipatory and outcome emotions, respectively.
Women's use of coping strategies was less clearly defined in the waiting stage.
More distraction and social support seeking was used during the stimulation stage.
More acceptance and social support seeking was reported in the outcome stage.
The waiting stage was characterized by greater coping activity and use of all coping strategies.
Feelings of tension, anxiety and worry are very prominent in the days leading up to the results of medical tests.
An increase in depressive reactions is the likely psychological outcome of unfavorable medical outcomes.
Facilitating coping strategies that better fit the demands of the waiting period, and offering support once outcomes are known, would provide a more optimal treatment environment.
Footnotes