
Abstract
Cardiovascular disease represents the main health problem for women as it is the leading cause of death and morbidity. In recent years, technological advances and experience gained by surgeons and cardiologists has resulted in a significant improvement of percutaneous coronary procedures, which has been demonstrated to be safe and effective for both men and women. However, gender disparities in the management of coronary artery disease, specifically in the rate of use of these interventional procedures, as well as in the incidence of cardiovascular events have been reported. Treatment inequalities may also impact on outcomes. Possible reasons for treatment bias include a patient's preferences, a physician's decisions, biological and pathophysiological gender differences and inadequate evidence-based medicine among women.
Keywords
Worldwide, coronary heart disease (CHD) is responsible for the death of more than 7 million people each year; with half of these deaths occurring in women [1]. This alarming number does not include other cardiovascular (CV) deaths, cerebrovascular accidents (CVA), aortic aneurysms and deaths related to diabetes, hypertension and renovascular disease among others. All these arterial diseases, which are also related to long-term physical and/or mental disability, have the same pathological origin – atherosclerosis.
Undoubtedly, CV disease (CVD) represents the main health problem for women. In 2006, in the USA alone, 41.3 million women were affected by CV problems. In the last two decades, more women than men died each year owing to CV reasons [2]. An increase in ischemic heart disease mortality among women, especially in developing countries is predicted. In fact, the absolute number of deaths is higher in developing countries than in high-income countries [3,4]. It has also been reported that in 2009 CVD and stroke will cost US$475.3 billion [2].
Obstructions in any artery can generally be relieved through by-pass surgery or through endovascular procedures. Percutaneous coronary interventions (PCI) performed in patients with ischemic heart disease have been demonstrated to be beneficial as both diagnostic and therapeutic tools. Translating these data into clinical practice, between 1979 and 2005 the number of cardiac catheterizations increased 342% to 1,322,000 annually in the USA [5].
To date, coronary angiography is the gold standard for evaluating coronary artery disease (CAD) and PCI is the most frequently used technique for revascularizing the ischemic myocardium. Of the 1,313,000 PCI procedures performed in the USA in 2006, according to the data provided by the National Center for Health Statistics and the National Hospital Discharge Survey, 35% were performed on women [4]. Even if this proportion seems appropriate, since approximately 65% of CHD patients are male and 35% are female, several studies from different countries have documented gender disparities in the management of CAD and, specifically, in the rate of use of interventional procedures, an issue that is probably related to the fact that women with CAD present differently than men and less frequently with ‘typical angina’.
This review examines sex differences in demographics and outcomes of women undergoing PCI in several clinical scenarios and also analyzes gender aspects in the use of new drugs and devices in interventional cardiology.
ST-segment elevation myocardial infarction
It is well established that the main goal to achieve in patients with ST-elevation myocardial infarction (STEMI) is restoration of blood flow in the infarct-related vessel. Reperfusion therapy, both with thrombolytics and with primary PCI, have been demonstrated to be safe and effective among women.
The Fibrinolytic Therapy Trialist' meta-analysis, which included trials of more than 1000 patients each, assessed the efficacy and safety of thrombolysis in patients with acute myocardial infarction (MI). Among the 13,855 women included, thrombolysis, compared with placebo, was associated with a 12% reduction of 35-day mortality (
Female inclusion and outcomes in clinical controlled trials and registries.
C-SIRIUS: Canadian study of the sirolimus-eluting stent in the treatment of patients with long de novo lesions in small native coronary arteries; E-SIRIUS: Sirolimuseluting stents for treatment of patients with long atherosclerotic lesions in small coronary arteries; FRISC: Fragmin and Fast Revascularization During Instability in Coronary Artery Disease; FTT: Fibrinolytic Therapy Trialists'; GUSTO: Global Use of Strategies to Open Occluded Arteries in Acute Coronary Syndromes; MI: Myocardial infarction; NSTE ACS: Non-ST segment elevation acute coronary syndromes; PTCA: Percutaneous transluminal coronary angioplasty; RAVEL: Randomized Comparison of a Sirolimus-Eluting Stent with a Standard Stent for Coronary Revascularization; RITA: Randomized Intervention Trial of Unstable Angina; SIRIUS: Sirollmus-coated Bx Velocity balloon expandable stent in the treatment of patients with de novo coronary artery lesions; STEMI: ST-segment elevation myocardial infarction; TACTICS: Treat Angina with Aggrastat and Determine Cost of Therapy with an Invasive or Conservative Strategy; TVR: Target vessel revascularization.
A mechanical reperfusion strategy with primary angioplasty has also been proven to be effective and safe in women [7]. The Global Use of Strategies to Open Occluded Arteries in Acute Coronary Syndromes (GUSTO IIb) trial compared the outcomes of patients treated with thrombolysis and those treated with primary PCI. The benefit conferred by angioplasty was higher in women than in men; in fact, the absolute risk reduction was 56 deaths prevented for every 1000 women treated with primary PCI, compared with 42 deaths prevented for every 1000 men treated with primary PCI [8,9]. These results were also confirmed in elderly women, in whom primary PCI compared with thrombolysis was associated with a significant reduction of mortality at day 30 (10.4 vs 15.4%; p < 0.0001) and at 1 year (16.9 vs 21.0%) [10].
In the setting of acute MI complicated by cardiogenic shock, the Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock (SHOCK) trial demonstrated that in terms of death, early revascularization was similar to medical stabilization at day 30, but the mortality rate improved at 6 months, reducing the overall mortality independently of gender (50.3 vs 63.1%; p = 0.027) [11].
It has been demonstrated that women who do not receive any reperfusion therapy have a poor prognosis, with an in-hospital mortality rate of almost 18% [12].
However, data provided by observational registries demonstrate that women are less frequently treated with reperfusion strategies compared with men and delays in administering such therapies are longer among women [13].
The National Registry of Myocardial Infarction (NRMI)-2 identified 84,663 patients eligible for reperfusion therapy, of which 24% did not receive any form of such therapy. In the multivariate analysis, female sex was independently associated to the clinical decision not to use reperfusion therapies, a finding also reported in the Global Registry of Acute Coronary Events (GRACE) population (odds ratio [OR]: 1.32; 95% CI: 1.20–1.46) [14,15].
Female sex was also found to be an independent variable associated with longer door-to-balloon times in patients transferred for primary PCI [16]. Moreover, even when trend analyses of door-to-balloon times in the USA from 1994 to 2003 described a drop from 120 to 106 min, delays in specific subgroups of patients, such as women and the elderly, showed no improvements [12].
The last survey of STEMI, conducted in Argentina, demonstrated that the median time from symptoms onset to hospital arrival was almost 2 h longer in women compared with men (330 vs 220 min, respectively) and that women were less frequently referred for primary PCI [17].
A recent report of the Get With the Guidelines – Coronary Artery Disease database, confirmed that, at present, compared with men, women with STEMI are still receiving less reperfusion therapies (adjusted OR: 0.78; 95% CI: 0.65–0.92) and timely reperfusion (door-to-needle time of ≤30 min: adjusted OR: 0.78; 95% CI: 0.65–0.92; door-to-balloon time of ≤90 min: adjusted OR: 0.87; 95% CI: 0.79–0.95). Women also reported reduced use of cardiac catheterization and revascularization procedures after MI compared with men [18]. The Minnesota Heart Survey also demonstrated a gender bias in the referral of patients for coronary angiography, but not in the subsequent use of coronary revascularization [19].
The underutilization of reperfusion strategies could be attributed to different factors. One such factor is that, on average, most women presenting with STEMI are older than men and often have many more comorbidities, such as diabetes, hypertension, congestive heart failure and severe noncardiac disease, which can lead physicians to be reticent to aggressively treat women. It is also true that women have a higher proclivity than men to suffer intracranial hemorrhage with thrombolytic drugs [20].
Another possible explanation for the gender disparities in the treatment of CAD/CHD is the fact that women can experience more vague symptoms than men; women are less likely to have typical chest pain and they commonly experience dyspnea, nausea, fatigue, indigestion or palpitations [21–23]. This can be, in part, the reason for longer delays in diagnosis and treatment.
Aside from this explanation, it has been demonstrated that most women do not consider themselves to be at risk of CHD. A survey conducted by the American Heart Association, and replicated by the Argentine Cardiology Foundation, demonstrated that women were unaware of CVDs as the main cause of death and, instead, perceived cancer as their primary health problem [24,25]. A possible consequence of these findings is that women may interpret symptoms as being caused by reasons other than CV factors.
Furthermore, evidence on benefits regarding reperfusion therapies among women is conclusive: both thrombolytics and primary PCI increase survival and are safe. Therefore, women presenting with STEMI should be referred early for diagnostic angiography and, possibly, PCI.
Non-ST-segment elevation acute coronary syndromes
Several randomized trials in patients with non-ST-segment elevation acute coronary syndromes (NSTE-ACS) have compared risks and benefits of a routine invasive strategy, including coronary angiography followed by revascularization, and a more conservative strategy with referral for intervention only if symptoms recur or there is evidence of inducible ischemia [26–30]. While the Treat Angina with Aggrastat and Determine Cost of Therapy with an Invasive or Conservative Strategy – Thrombolysis in MI-18 (TACTICS TIMI-18) study demonstrated that the invasive strategy was beneficial regardless of gender, Fragmin and Fast Revascularization During Instability in Coronary Artery Disease (FRISC II) and the Randomized Intervention Trial of Unstable Angina (RITA 3) suggested that such an invasive approach was associated with an increased risk of death or infarction in the female population (
The type of vessel involvement, smaller coronary vessel size and lower BMI may also represent features related to women's less favorable risk profile for surgery and greater periprocedural complications due to technical difficulties [35]. Aside from this, some authors have argued that women may demonstrate poorer outcomes after CABG owing to lower rates of arterial use compared with men, specifically internal thoracic or mammary artery use [36].
A recently published meta-analysis on this issue confirmed, with positive biomarkers, that invasive management has comparable benefit in men and high-risk women for reducing the composite end point of death, MI or rehospitalization caused by ACS [37]. However, women at low risk receive no benefit from an invasive approach and they should be managed with a more conservative strategy.
Different large-scale registries demonstrate the management patterns of NSTE-ACS during the last years: the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the American College of Cardiology/American Heart Association Guidelines (CRUSADE) trial, with 40,912 patients included at 391 hospitals in the USA between 2000 and 2002; GRACE, with more than 20,000 patients referred for coronary angiography in several countries from 1999 to 2006; and the Register of Information and Knowledge about Swedish Heart Intensive Care Admissions (RIKS-HIA), which included 53,781 patients in Sweden between 1998 and 2002 [38–40]. These observational studies demonstrated that although women were older and had a higher prevalence of risk factors, such as hypertension and diabetes, they were less likely to be referred for cardiac catheterization and revascularization than men. Registries also found a greater proportion of normal or mild obstructive coronary disease among women.
In the CRUSADE trial, more women were at higher risk for unadjusted in-hospital mortality, reinfarction, heart failure, stroke and red blood cell transfusion compared with men; however, after adjustment, only transfusion was higher in women [41]. Outcomes analyses in the GRACE trial revealed that even after adjustment for age and severity of the disease, the incidence of MI, stroke and rehospitalization was higher in women compared with men [42].
Recent evidence suggests that high-risk women should be referred for an early invasive management. On the contrary, women with low or intermediate risk should be approached with a conservative strategy, since it has been demonstrated to be safe and effective [43].
Drugs & devices
The advances in PCI have been linked to the improvement of techniques with better devices, to an increasing operator' experience and to the excellent quality of the angiograms.
Since the introduction of the coronary stents, which are mainly endovascular metal tubes, problems, such as acute occlusions and subacute elastic recoil of the dilated segment commonly observed with balloon angioplasty, have been overcome. However, bare-metal stents do not stop the biological mechanism of restenosis, which runs from 8 to 60%, according to variable extension and severity of the coronary obstructions. A significant reduction of the incidence of restenosis has been achieved with drug eluting stents (DESs), which are metal stents covered by a polymer or other compounds used as carriers for citostatics or similar drugs that inhibit the proliferative mechanism of restenosis. DESs with sirolimus and also with paclitaxel have been demonstrated to be safe and effective both in men and women, mainly by reducing the rate of target lesion revascularization (
Although it is clinically proven that the benefits from DESs are independent from gender, compared with men, women receive DESs less frequently. The National Heart, Lung and Blood Institute (NHLBI) Registries, which assessed the standard use of DESs in 3129 patients as well as the off-label use among 3422 patients, found that 68.8% of men received a DES while only 31.2% of women had DESs during their PCI procedures [48]. This was also the case in other large registries, such as e-Cypher, the Swedish Angiography and Angioplasty Registry (SCAAR) and Registro AngiopLastiche dell’Emilia Romagna (REAL) (
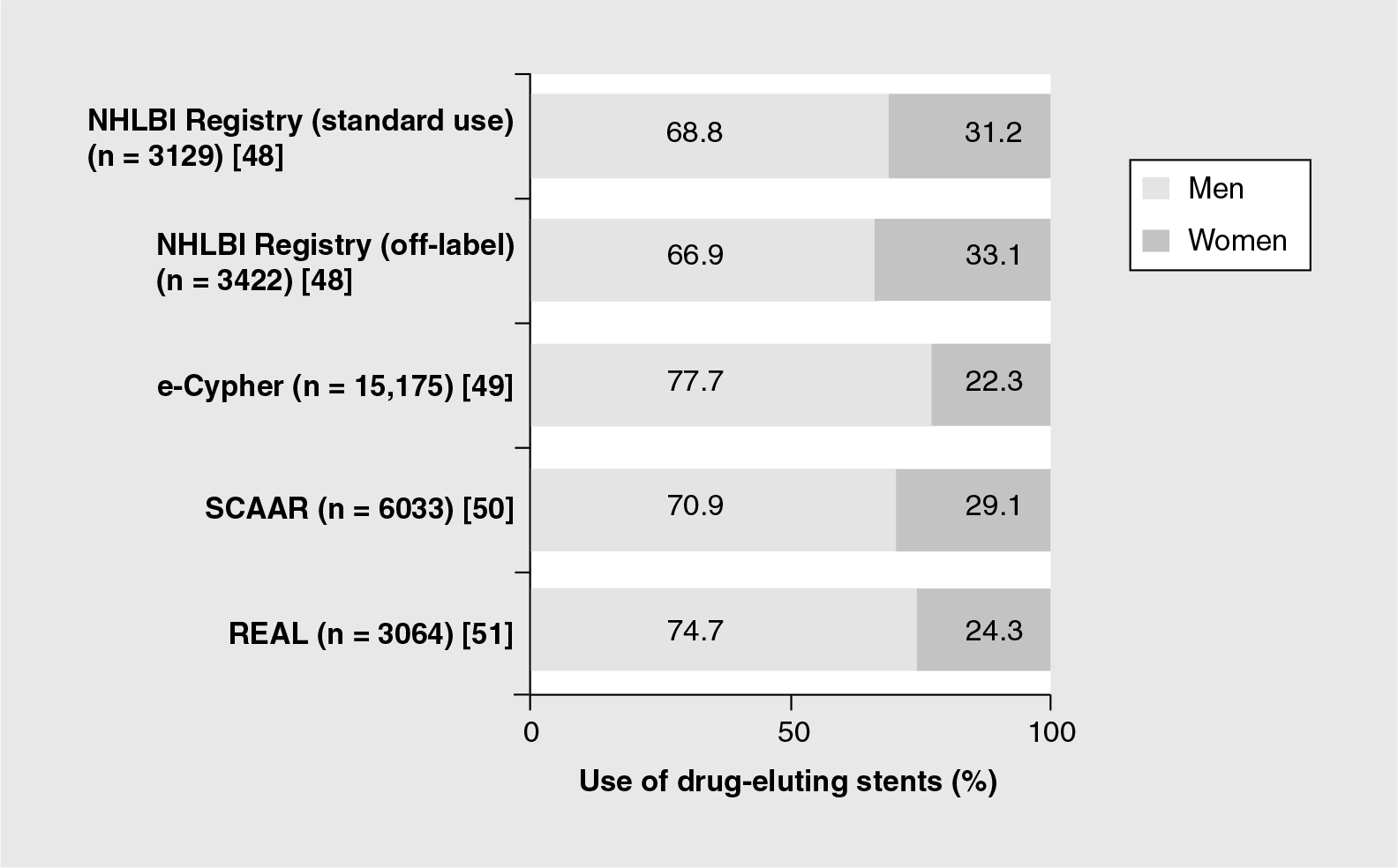
Proportion of drug-eluting stents use in different registries.
Female population in PCI registries and clinical trials usually demonstrate a greater prevalence of comorbidities, such as diabetes, hypertension and older age (average 5–6 years), but a lower prevalence of smoking, prior MI, prior by-pass surgery and, also, multiple vessel disease [44,46,52]. In spite of the significant increase in the diabetic population, among women at risk for higher rates of restenosis, clinical outcomes were independent from gender. In multivariable analyses, female gender was not associated with increased clinical events [44,46].
In conclusion, in terms of PCI procedures women have a similar magnitude of treatment effect achieved with DESs compared with men; however, at present, the evidence is that the use of these devices are much less frequent among women with the possible increased need for new revascularization procedures.
Antithrombin drugs and their dose regimens also deserve a special mention when considering women's health since women represent a particularly vulnerable group to hemorrhagic outcomes. Data from the CRUSADE registry demonstrated that women had higher rates of major bleeding, were or not treated with glycoprotein (GP) IIb/IIIa inhibitors and were three-times more likely to receive excess doses of GP IIb/IIIa inhibitors compared with men (46.4 vs 17.2%, respectively) [53]. Moreover, as the impact of excess dose on the risk of bleeding was worse in women compared with men (OR: 1.72 vs 1.27, respectively), the proportion of bleeding attributable to excess dosing was fivefold higher among women compared with men (25.0 vs 4.4%, respectively). In the Harmonizing Outcomes with Revascularization and Stents in Acute MI (HORIZONS-AMI) trial, which included patients with STEMI undergoing PCI, bivalirudin monotherapy was associated with a lower risk of major bleeding compared with heparin plus GP IIb/IIIa inhibitors in both genders, which was also reflected in a significant lower mortality. However, even with bivalirudin, women suffered more hemorrhagic complications than men at day 30 and at 1 year [54,55].
Outcomes of coronary interventions in women
The NHLBI collected demographic and outcomes data on consecutive patients undergoing PCI at multiple US centers in several enrollment waves. The NHLBI-funded Dynamic Registry, including 15 clinical centers and a coordinating center, was designed to evaluate three separate cohorts of approximately 2000 patients. Of the clinical centers, 11 were participants in the Percutaneous Transluminal Coronary Angioplasty (PTCA) registries.
Data from 1985 to 1986 demonstrated that mortality was tenfold higher in women compared with men during their hospital stay (2.6 vs 0.3%, respectively) and almost twice as high in the 4-year follow-up (10.8 vs 6.6%, respectively; p < 0.05) [56]. More recent analysis, from 1997 to 1998, reported smaller differences between women and men in in-hospital mortality (2.2 vs 1.3%, respectively; p = 0.07) and in 1-year mortality (6.5 vs 4.3%, respectively; p=0.02). Moreover, after controlling for other significant factors, female gender was not a significant predictor of death (risk ratio [RR]: 1.26; 95% CI: 0.85–1.87) or death and MI (RR: 1.14; 95% CI: 0.86–1.50) [57].
Similarly, the Northern New England PCI Registry, as well as other studies, demonstrated an increased mortality rate in women, which became statistically insignificant after adjustment for baseline characteristics [58–60].
Available evidence supports the idea that higher unadjusted mortality rates are probably related to the fact that, on average, women presenting with STEMI are older and have an overall higher baseline risk profile than men; thus, when these multiple variables are taken into account, gender differences disappear or are attenuated. However, other studies demonstrating that there is still a prognostic gap by gender after adjusting for age and comorbid conditions, suggest that treatment inequalities impact on outcomes [61–63]. A simulation model performed with the National French Hospitals database found that age-adjusted mortality in women would be reduced if rates of interventions were the same in women and men [64].
One of the reasons that can be postulated to explain this treatment bias is a patient's preferences. It has been demonstrated that women are more likely than men to decline a major procedure [65]. Regarding physician' decisions, the fact that on average, most women presenting with STEMI are older than men and more often have other comorbidities and more vague symptoms, can lead doctors to believe that women could suffer more complications and receive less benefit from coronary interventions than men [66]. This is particularly applicable to surgery. Women have more complications, a more difficult recovery and benefit less from CABG compared with men [67,68]. It has been proposed that the higher operative mortality of women undergoing CABG may be explained by differences in referral patterns, with women considered for surgery at later stages in their disease than men [69].
Certainly, women have different biological characteristics than men, including vessel diameter and stiffness. Among women, a higher prevalence of vascular abnormalities, such as vasospastic disorders and Raynaud phenomenon, a more diffuse pattern of atherosclerosis and more frequent endothelial and smooth muscle dysfunction has also been described [70].
Furthermore, it is also true that evidence-based medicine is less strong among women compared with men [71]. In 1986, the NIH adopted a policy for the inclusion of women in clinical research, based on the Report of the Public Health Service Task force on Women's Health Issues [72]. In 1992, the General Accounting Office Report on Women's Health established that the ‘standard of representativeness is a comparison of the proportion of women among clinical trials participants with the proportion of women among those persons with the disease for which the drug is intended’ [101]. Despite this, at present, women are still often under-represented in clinical trials [73]. In the setting of STEMI, for example, the proportion of women included in observational registries, such as NRMI-2 and GRACE, was 30%, while the proportion of women randomized in Fibrinolytic Therapy Trialists (FTT) and GUSTO IIb trials was 23% (
Even if women do have worse prognosis than men, it is clear that women referred for interventional approaches have better outcomes than women who do not receive such strategies.
Temporal trends analyses of the NHLBI database demonstrated that women included in the last Dynamic registry were older and with more comorbid diseases than women in the earlier registries. Despite this baseline risk, recent adjusted data found a 50% reduction in 1-year mortality compared with the initial results. Therefore, it seems that as time goes by, interventional cardiology is treating women who are seeking treatment with significant improvements in outcomes [76].
Bleeding, as previously mentioned, represents a particular outcome that must be carefully considered among women. It is likely that one of the causes for increased bleeding among women is a poor management of antithrombotic drugs with no adjustment for body surface. Probably, overall results of PCI will improve by ensuring a better selection and management of antithrombotic drugs. Since bleeding is mostly related to the PCI procedure, and since women have smallersized vessels, improving and miniaturizing the devices, such as introducers, guiding catheters and femoral percutaneous closing devices, should also contribute towards diminishing the femoral access bleeding.
All of these measures are likely to result in better overall results of PCI in women.
Conclusion
A study of the decrease in US deaths caused by CHD from 1980 to 2000 suggests that approximately 47% of the decrease was attributed to evidence-based medical therapies [77]. In this sense, coronary interventions in all the spectrum of CHD, as well as devices used in these procedures, have demonstrated their safety and efficacy in women. However, real-life data demonstrate that women are referred for diagnostic and therapeutic coronary interventions significantly less frequently than men. Biological and cultural hypotheses have been postulated to explain the reasons for this bias. Doctors, researchers and the entire team working for women's healthcare should deeply analyze these differences in order to improve outcomes in women and especially to offer women the best available treatments. It is also very important to increase the evidence on treatment risks and benefits of interventional procedures in women. There are strong enrollment biases in clinical trials that undermine efforts to provide evidence-based care to women.
Future perspective
Cardiovascular disease is expected to increase in the coming years. Diagnostic and therapeutic coronary interventions, especially PCI, will be the treatment of choice of most patients with coronary disease. The existing gender gap in access to these procedures should be minimized. It is also necessary to educate physicians and the community regarding the impact of CVD in women, in order to understand gender-related aspects of the disease, to increase sex-based evidence and to improve women-specific recommendations in order to achieve a better daily clinical practice offering women the best available treatments.
Executive summary
Cardiovascular disease represents the main health problem for women as it is the leading cause of death and morbidity.
Gender disparities in the management of coronary artery disease, and specifically in the rate of use of interventional procedures, have been reported.
Reperfusion therapy, both with thrombolytic drugs and with primary percutaneous coronary interventions, has been demonstrated to be safe and effective among women.
Women who do not receive any reperfusion therapy have a poor prognosis, with an in-hospital mortality rate of almost 18%.
However, women are less frequently treated with reperfusion strategies than men and delays in administering such therapies are longer among women.
The underutilization of reperfusion strategies could be attributed to different factors: on average, most women presenting with ST-elevation myocardial infarction are older than men and more often have many more comorbidities; women also have a higher proclivity to suffer intracranial hemorrhage with thrombolytics. Other possible explanations are that women can experience more vague symptoms than men and most women do not consider themselves to be at risk of coronary heart disease.
Results of clinical trials that consider the benefits of invasive strategy in women with non-ST-segment elevation acute coronary syndromes have been controversial.
A lack of benefit of the invasive management can be related to a poor outcome in women undergoing coronary artery by-pass surgery.
Different large-scale registries have demonstrated that women are less frequently referred for coronary angiography and revascularization than men.
A recently published meta-analysis confirmed, with positive biomarkers, that invasive management in men and high-risk women reduces the composite end point of death, myocardial infarction or rehospitalization caused by acute coronary syndromes. However, women with low risk receive no benefit from an invasive approach and they should be managed with a more conservative strategy.
Drug-eluting stents with sirolimus, and also with paclitaxel, have been demonstrated to be safe and effective both in men and women, mainly by reducing the rate of target lesion revascularization.
Registries demonstrate that women receive drug-eluting stents less frequently than men.
Antithrombin drugs, such as bivalirudin, and their dose regimens deserve a special mention when considering women's health since women represent a particularly vulnerable group to hemorrhagic outcomes.
Women are more likely to receive excess doses of glycoprotein IIb/IIIa inhibitors than men. Aside from this, the impact of excess dose on the risk of bleeding is worse in women than in men.
Unadjusted rates of cardiovascular events are higher among women, probably because women presenting with STEMI are older and have an overall higher baseline risk profile than men. However, most of the registries demonstrate no gender differences in outcomes after controlling for age and comorbidities.
Female gender is independently associated with risk of bleeding.
Treatment inequalities may impact on outcomes. Possible reasons for treatment bias include a patient's preferences, a physician's decisions, biological and pathophysiological gender differences and inadequate evidence-based medicine among women.
Temporal trends analyses of percutaneous coronary interventions demonstrate significant improvements in outcomes among women.
Although coronary interventions have demonstrated their safety and efficacy in both genders, real-life data demonstrate that women are referred for diagnostic and therapeutic procedures significantly less than men.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.