
Abstract
Angiographic evidence of thrombosis in more than one coronary artery at the same time is uncommon in patients with acute myocardial infarction, and this is hard to identify with routine electrocardiography. Patients may manifest with high-degree atrioventricular block, cardiogenic shock, or sudden cardiac arrest, all of which are potentially fatal outcomes. This case study focuses on a patient who experienced cardiogenic shock, high-degree atrioventricular block secondary to acute anterior-inferior ST-segment elevation myocardial infarction. During the coronary angiogram, thrombotic occlusions of the left anterior descending and right coronary arteries were observed. A patient was salvaged by the use of mechanical circulatory assistance in conjunction with prompt percutaneous coronary intervention of both the culprit arteries. Our case report emphasizes the importance of completing revascularization as soon as possible by opening the culprit arteries and ensuring appropriate mechanical circulatory support to the patient.
Keywords
Introduction
ST-segment elevation myocardial infarction (STEMI) caused by multiple coronary thromboses is rare. Left ventricular function rapidly diminishes when left untreated, resulting in cardiogenic shock and death if not treated promptly. 1 Those two coronary arteries that originate on opposing sides of a coronary tree (ie, the right coronary artery (RCA) and the left anterior descending artery (LAD) or the RCA and the left circumflex artery) are typically affected, and the clinical course is described as disastrous in the literature. 2 The optimal treatment for STEMI due to a number of culprit lesions is not defined by any guidelines or randomized controlled trials.
We present a patient with “double myocardial infarct syndrome,” defined as concurrent complete occlusions of the 2 major epicardial coronary arteries, who had immediate full revascularization and implantation of an intra-aortic balloon pump and had a favorable clinical course.
Case Report
A 48-year-old male physician with poorly managed diabetes came to the emergency department after noticing diaphoresis and retrosternal chest pain while doing outpatient examinations. The pain had been radiating to his left upper extremity for the past 8 hours. He self-diagnosed acute myocardial infarction at his own clinic with an electrocardiograph (ECG) and was taken to a local cardiac center for treatment. The ECG showed ST-segment elevations in the inferior (II, III, aVF) and antero-lateral leads (V1-6, qRBBB) with 2:1 atrio-ventricular block (high-degree AVB) (Figure 1A). His vital signs showed a heart rate of 36 beats per minute, a blood pressure of 70/40 mmHg, a respiratory rate of 22 breaths per minute, and an oxygen saturation of 86% in room air. He was administered with loading dose of dual antiplatelet treatment (325 mg of aspirin and 300 mg of clopidogrel), high-dose statin (80 mg), and injectable streptokinase (1.5 million units) by the attending cardiologist. To stabilize his vital indicators, an intravenous noradrenaline infusion, temporary pacemaker, and noninvasive ventilation were used. Echocardiography revealed mild left ventricular dilatation with regional wall motion abnormality of the anterior and inferior walls with ejection fraction of 25%. There was also moderate mitral regurgitation (MR), grade III diastolic dysfunction, normal right ventricular function, mild tricuspid regurgitation, and mild pulmonary artery hypertension (pulmonary artery pressure = 45 mmHg). Coronary angiography indicated occlusion of the proximal segment of the LAD before the origin of the first septal perforator and the distal segment of the RCA were both occluded (Figures 2A,D). There was also a borderline lesion in the ostial segment of the obtuse marginal artery and significant stenosis of the distal left circumflex artery. His laboratory parameters revealed abnormalities in the form of elevated troponin levels (80 ng/L; normal level 0-0.12 ng/L), N-terminal prohormone B-type natriuretic peptide levels (18,670 pg/mL; normal levels <450 pg/mL for age < 75 years), increased white blood cell count (22.3 × 10 9 /L), elevated liver enzymes (serum aspartate aminotransferase levels—133; normal range: 5-40 units/L; serum Alanine aminotransferase levels—155; normal range: 7-56 units/L).
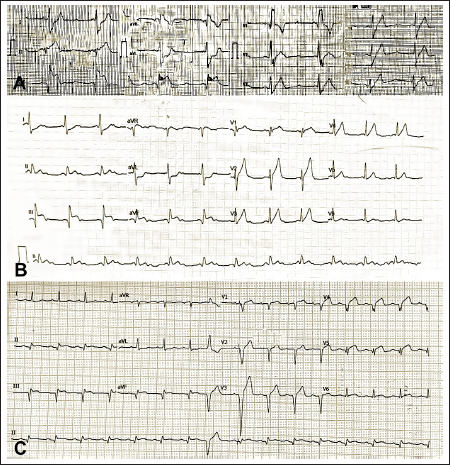
First electrocardiogram (ECG) demonstrated qRBBB pattern, ST-segment elevation in anterior and inferior leads with complete heart block (Panel A). In the emergency room, an ECG revealed 2:1 atrio-ventricular block and ST-segment elevation (STE) in the inferior leads, with more STE in lead III than lead II, as well as hyperacute STE in leads V2-4 and reciprocal ST-segment depressions in leads I, aVL (Panel B). Post procedure, ECG showed improvement in ST-T segments with establishment of normal sinus rhythm (Panel C).
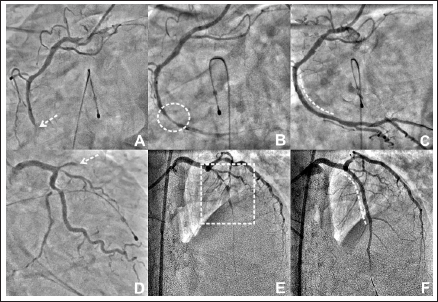
Coronary angiography revealed thrombotic occlusions of the proximal segments of the left anterior descending artery (dashed white arrow; Panel A ) and the distal segment of the right coronary artery in the presence of a temporary pacemaker insertion (dashed white arrow; Panel D ). Thrombolysis in myocardial infarction (TIMI) III flow with discrete 90% stenosis of the distal segment (dashed white circle; Panel B ) was discovered during percutaneous coronary intervention of the RCA. The stenosis was deployed with a drug-eluting stent (Panel B ), which resulted in no residual stenosis and brisk TIMI III flow (dashed curved white line; Panel C ). There was also the establishment of TIMI II flow to the LAD with critical stenosis of its ostio-proximal segment (dashed white rectangle; Panel E ), which was stented using drug-eluting stent (dashed curved white line) following predilatation, resulting in TIMI III flow (Panel F ).
He referred him to our facility for additional advanced medical therapy, including revascularization. When he arrived at our ER, his vital parameters revealed sinus tachycardia (heart rate—112 beats per minute), blood pressure of 90/60 mmHg on a low dosage of noradrenaline, and oxygen saturation of 93% on 4 liters per minute of oxygen using a mask. The ECG showed that the qRBBB pattern had resolved, but there was persistent simultaneous STE in the antero-inferior leads and complete heart blocks (Figure 1B). The same findings from the initial echocardiogram were seen in the repeat examination. Due to simultaneous obstruction of 2 coronaries and cardiogenic shock, he was transported to the catheterization laboratory for percutaneous coronary intervention (PCI) after receiving a loading dose of ticagrelor (180 mg). Instead, an intra-aortic balloon pump was used through the right femoral route to stabilize his hemodynamic status. The left femoral approach was employed for the PCI, and the RCA was initially engaged using Judkin’s right guiding catheter. Direct stenting of a 2.75 x 33 mm everolimus drug-eluting stent was performed in the distal portion of the RCA, which was shown to have thrombolysis in myocardial infarction (TIMI) 3 flow with tubular 90% stenosis on angiography. After an implantation of the stent, a slow-flow phenomenon occurred, which was treated with intracoronary nicorandil, but it caused temporary hypotension with sinus bradycardia, which was restored by supportive measures in a hemodynamic crisis (Figures 2A-C). With RCA revascularization, hemodynamics improved, allowing for a lower dose of ionotropic support and enhanced IABP.
After RCA stenting, there was no collateral flow from the RCA to the LAD, suggesting an acute blockage of the LAD. To access the LAD, an EBU guiding catheter was utilized, and angiography revealed severe stenosis with TIMI 2 flow. Following predilatation with a 2.5 x 12 mm balloon, an everolimus 3.0 x 48 mm drug-eluting stent was implanted, and the ostio-proximal segment was post-dilated with a 3.5 x 12 mm balloon, resulting in TIMI 3 flow (Figures 2D-F). His ECG following the intervention showed that the ST-T abnormalities in the antero-inferior leads had been resolved, that he had normal sinus rhythm, and that he had infrequent ventricular premature complexes, indicating reperfusion (Figure 1C).
Noninvasive ventilation was started to assist his respiration in the advanced medical care unit, and hemodynamic support in the form of IABP and inotropic infusion was sustained and eased off after 2 days. With the help of dual anti-platelet therapy (aspirin and ticagrelor), high-dose statins, beta-blockers, empagliflozin, eplerenone, diabetes control, and further supportive care, his clinical state and laboratory parameters improved, and on day 5, he was discharged from the hospital. He has now finished 6-months of follow up with no symptoms and left ventricular ejection fraction improved to 50%, mild MR.
Discussion
STEMI is caused by a complete blockage of a single coronary artery, known as the culprit vessel, as a result of plaque rupture, thrombus formation, or vascular obstruction. Acute thrombosis of many coronary arteries at once is a rare cause of STEMI in clinical practice.1 Acute coronary thrombosis in numerous arteries was identified in only 2.5% of 711 patients diagnosed with STEMI and treated with primary PCI, while Maage et al reported an incidence of 1.3% of patients who were provided primary PCI.3,4
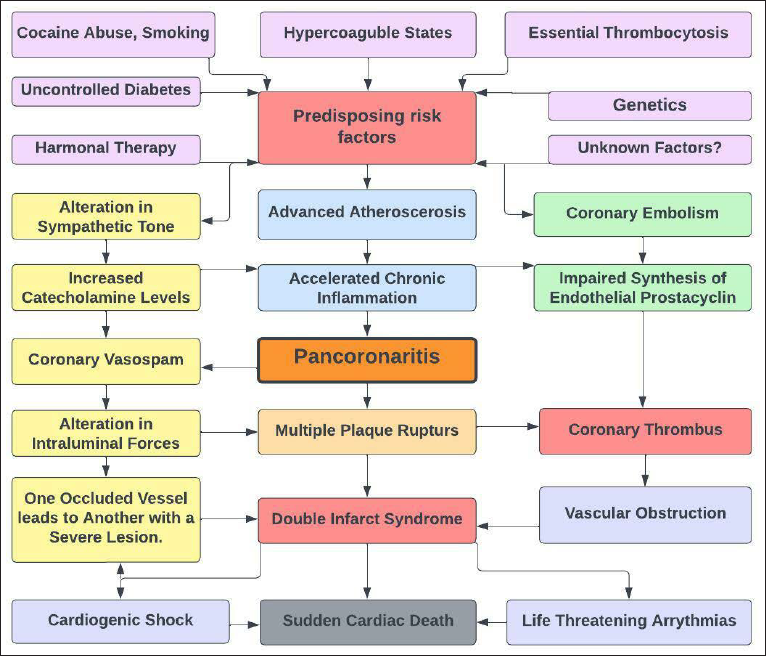
Many coronary plaques may be destabilized at once by an inflammatory response that does not target a specific lesion as the source of the problem. Because atherosclerosis is a chronic inflammatory disease that frequently manifests as an acute coronary syndrome that can be multifocal, rupturing numerous coronary plaques, the word “Pancoronaritis” appropriately represents the condition, as illustrated in the flow diagram (Figure 3). According to the research that was conducted by Goldstein et al., well over 30 percent of patients who had STEMI had many plaque ruptures with overlying thrombi. 5 According to Burke and Virmani’s research, numerous thromboses were found in the coronary tree of even half of patients (50%) who died from “fatal double myocardial infarct syndrome.” In a case series published by Pollak et al, simultaneous occlusions of the LAD and RCA were detected in 49% of the cases, as in our instance. 3
Flow diagram showing the pathophysiology of “double myocardial infarct syndrome.”
Hypercoagulable states, cocaine use, smoking, essential thrombocytosis, the use of oral contraceptive pills, tamoxifen, clopidogrel resistance from CYP2C19 polymorphism may play a role in the development of multivessel coronary artery thrombosis, while the exact cause of this condition in many cases remains unknown. 7 Long-term uncontrolled diabetes is associated with multiple coronary thromboses, as in our case, which is addressed in just a few case studies, including one by Ikeda et al. 8 They documented 2 patients with type 2 diabetes and concomitant LAD and RCA occlusion. According to the author, it is induced in part by a proclivity for hypercoagulability in diabetics who have experienced consecutive decreases in coronary blood pressure and restriction in coronary blood flow.
If high-degree AVB and STEMI are present, temporal pacing may be required because the majority of AVB patients with inferior STEMI are of supra-Hisian origin, implying a link to AV nodal ischemia that resolves after revascularization, as in our instance. 9 The most common cause of RBBB following an anterior STEMI is ostio-proximal occlusion of the LAD and impaired septal artery circulation to the bundle branches. ECG findings indicated simultaneous occlusions of the RCA and LAD including ST-segment elevation (STE) in leads III greater than in lead II with concomitant STE in leads V3-4. Leads V3–4 are spared in the event of an acute dominant RCA blockage, but STE frequently occurs in the inferior and posterior leads and occasionally in leads V5 and V6. Leads V3 and 4 typically show the highest STE in individuals with acute LAD occlusion.
Cardiogenic shock (36%) or sudden cardiac death are common among patients with concurrent coronary artery occlusion. 3 Unfortunately, the admission ECG could not help identify the artery that caused the infarction. Our patient had an acute inferior-anterior wall STEMI, as well as cardiogenic shock and high degree AVB. As a result of these challenges, Pollak et colleagues used an intra-aortic balloon pump in 32% of their cases, as we did, or other mechanical circulatory support devices, such as Impella, were used by Saito et al.1,3 Myocardial revascularization has been found to increase survival prospects in patients suffering from cardiogenic shock due to acute STEMI, and after thorough consideration of all of the options, we have decided that PCI is the best course of action for our patient. 10 As a result, it is critical that patients receive an early diagnosis and immediate PCI to improve their chances of life. During coronary angiography, we noticed that both the proximal segment of the LAD and the distal segments of the RCA had blocked. Once coronary flow was restored to both arteries, the patient’s clinical and hemodynamic state markedly improved.
Conclusion
Acute thrombi that occur simultaneously are a rare cause of STEMI, according to meta-analyses and case-control studies. Many culprit STEMI lesions have not been the subject of therapy recommendations or randomised controlled trials. Therefore, recommended case management is not articulated clearly. Overall, more retrospective and prospective research into STEMI cases with various acute causes is needed to better understand outcomes and therapeutic options. More information means it can become apparent that some clinical circumstances are not as uncommon as once imagined, and that individualized pharmacological and interventional therapy can improve patient outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from the participant included in the study.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.