
Abstract
The management of breast cancer depends on the tumor and patient's characteristics. Anthracycline-based regimens have been proven to decrease the risk of relapse and prolong survival time in breast cancer. Taxanes have been incorporated not only into metastatic breast cancer but also into adjuvant regimens. Capecitabine, an oral fluoropyrimidine carbamate, has good single-agent activity and, together with docetaxel, demonstrated preclinical synergy and a survival benefit in metastatic breast cancer. Recent analyses show that capecitabine/docetaxel dosing flexibility for managing side effects does not compromise efficacy, and define this combination regimen as an important treatment option for its efficacy, tolerability and cost-effectiveness.
Breast cancer is one of the leading causes of cancer-related mortality. Fortunately, mortality from breast cancer has recently been declining in western countries, owing to consistent protocols of primary management, including use of adjuvant systemic therapy, and possibly, in part, owing to screening.
Anthracycline-containing combinations are established as a component of adjuvant and first-line chemotherapy for breast cancer. In patients whose tumors have progressed despite anthracyclines, the taxanes, docetaxel and paclitaxel, are often the next preferred treatment in this setting. When the intention is to provide more aggressive therapy earlier in the disease course, typically in younger patients with life-threatening disease, combinations or sequences of anthracyclines and taxanes may be used as first-line chemotherapy for metastatic breast cancer (MBC). They have also been evaluated as adjuvant therapy for primary breast cancer. In the first-line setting, regimens including both anthracyclines and taxanes demonstrated response rates in the range of 50 to as high as 70% in selected patient populations [1–5]. One major drawback of combining anthracyclines and taxanes is the very high rate of myelotoxicity, manifested as neutropenia rates of 55–100% and febrile neutropenia rates of 23–34% [6,7].
In adjuvant treatment programs, the combination of docetaxel, doxorubicin and cyclophosphamide (TAC) has recently been approved in the UK by NICE. It is likely to lead to more use of docetaxel in the adjuvant setting, although owing to the aforementioned myelotoxicity problem, in the UK it is more likely that docetaxel will be used in sequence after anthracycline therapy rather than in combination [8,9].
The increasing use of anthracyclines and taxanes earlier in the disease course means that oncologists are now more frequently faced with the challenge of treating patients with recurrent disease that is resistant to these highly active agents. In this context, optimal palliation, maintenance of quality of life (QoL) and minimal interference with a normal lifestyle are particularly desirable in addition to the anticancer effect. Therefore, an ideal treatment in this setting should provide a reasonable prospect of response with minimal toxicity, reduce tumor-related symptoms, maintain QoL, be suitable for outpatient/day-case administration, possibly in a home-based environment, and, ultimately, prolong overall survival.
Capecitabine, an orally administrated fluoropyrimidine, has proven efficacy in MBC through a comprehensive worldwide clinical trial program [10–13]. On the basis of data demonstrating consistent activity in Phase II studies, capecitabine was approved in the USA for the treatment of patients with metastatic disease resistant to paclitaxel and anthracycline-containing therapy, with later EU approval for single-agent capecitabine in patients with metastatic disease after failure of taxanes and an anthracycline-containing regimen or in whom further anthracyclines were not indicated. Furthermore, a randomized Phase III study demonstrated that the addition of capecitabine to docetaxel, compared with single-agent docetaxel, in patients with anthracycline-pretreated MBC resulted in superior overall survival (OS; with a 3-month improvement in median survival), superior time to disease progression (TTP), and a superior overall response rate (ORR), with a manageable safety profile [14]. Capecitabine/docetaxel (XT) combination therapy is indicated in the US and Europe for the treatment of MBC failing anthracycline therapy. The XT regimen is the first cytotoxic combination to improve survival over standard monotherapy in patients with anthracycline-pretreated MBC. QoL was maintained with XT combination therapy and compared favorably with docetaxel alone, which further supports the use of this regimen in patients with anthracycline-pretreated MBC [15]. Pharmacoeconomic modeling using data from the Phase III trial [14] has also shown that the XT combination is highly cost effective when compared with other cancer treatments that improve survival [16–18].
This article reviews the current place of XT combination therapy for breast cancer and its efficacy, tolerability and future applications in the context of the developing world of cancer therapy.
Capecitabine/docetaxel combination therapy Pharmacology
Capecitabine is an orally administered fluoropyrimidine that is metabolically activated preferentially at the tumor site through a three-step enzymatic process. The final step in the generation of 5-FU from capecitabine is catalyzed by thymidine phosphorylase, an enzyme expressed at up to five-times higher concentrations in tumor compared with healthy tissue [19,20]. Furthermore, capecitabine shows antineoplastic activity and synergy with other cytotoxic agents. The coadministration of capecitabine and docetaxel results in synergistic antitumor activity in mouse xenograft models bearing MX-1 human breast cancer compared with either agent alone [21,22]. This potent effect appears to be characteristic of the combination of docetaxel with capecitabine or its intermediate metabolite 5′-deoxy-5-fluorouridine (doxifluridine; 5′-dFUrd [21]). Docetaxel showed a potent effect in combination with 5′-dFUrd, but a much weaker effect was observed in combination with 5-fluorouracil or UFT, a fixed combination of tegafur and uracil [21]. One possible explanation for the possible synergy is that docetaxel upregulates tumor levels of thymidine phosphorylase, the enzyme essential for the activation of capecitabine and 5′-dFUrd to 5-FU. In fact, docetaxel upregulated the thymidine phosphorylase levels 1.9-fold in the MX-1 models [21]. Based on these observations and high single-agent activity, clinical studies with docetaxel and capecitabine/5′-dFUrd combination regimen were performed.
Introduction of capecitabine to breast cancer treatment
There is an increasing number of patients who have already been exposed to active agents, such as anthracyclines and/or taxanes, either in the adjuvant setting or as first-/second-line treatment for MBC. Unfortunately, many of these patients become refractory to these agents at progression. In Phase II trials in patients previously exposed to anthracyclines and/or taxanes, capecitabine demonstrated consistently high activity with disease control, defined by response and/or stabilization of disease, in approximately two thirds of patients and a median OS of approximately 1 year [10–13,23,24].
The efficacy of single-agent capecitabine as front-line therapy for MBC has also been reported in Phase II studies and in a randomized, Phase III trial [25–27]. Those studies demonstrated response rates of 21–37% (Table 1) [25–27]. This is comparable with other agents, including first-line doxorubicin, with response rates of 36–41% [2,28], docetaxel, with response rates of 23–42% in anthracycline-pretreated MBC [29–33], and paclitaxel, with response rates of 17–34% in anthracycline-pretreated MBC [2,28,31,34–36].
Phase II/III trials of single-agent capecitabine for advanced/metastatic breast cancer.

2000 mg/m2/day for 14 of every 21 days or 1300 mg/m2/day for 21 of every 21 days.
MBC: Metastatic breast cancer.
QoL was evaluated in 1683 women with anthracycline- and/or taxane-pretreated MBC receiving single-agent capecitabine using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire C-30, v3.0 and the breast cancer-specific module BR-23 [37]. Approximately 65–80% of patients had improved or maintained QoL for most scales during capecitabine treatment, including functional and symptomatic QoL. Patients receiving capecitabine also had a significant improvement (p < 0.0001, unless stated) in the following: global health status, role and emotional functioning, cognitive functioning (p = 0.0001), social functioning, physical functioning (p = 0.0091), fatigue, nausea/vomiting, pain, insomnia, appetite loss (p = 0.0001), constipation, financial problems, dyspnea (p = 0.0003), body image, future perspective, systemic therapy side effects, breast symptoms, arm symptoms, and hair loss [37].
Impact of capecitabine/docetaxel combination therapy in MBC
A pivotal Phase III trial of XT demonstrated significantly superior OS to single-agent docetaxel in anthracycline-pretreated MBC [14]. Patients, most of whom were receiving study treatment as second-line therapy, were randomized to 21-day cycles of oral capecitabine 1250 mg/m2 twice-daily on days 1–14 plus docetaxel 75 mg/m2 on day 1 or to docetaxel 100 mg/m2 on day 1. XT resulted in significantly superior TTP (p = 0.0001; median: 6.1 vs 4.2 months), OS (p = 0.0126; median: 14.5 vs 11.5 months) [38], and objective tumor response rate (42 vs 30%; p = 0.006) compared with docetaxel (Table 2).
Phase III trials of capecitabine/taxane for advanced/metastatic breast cancer.
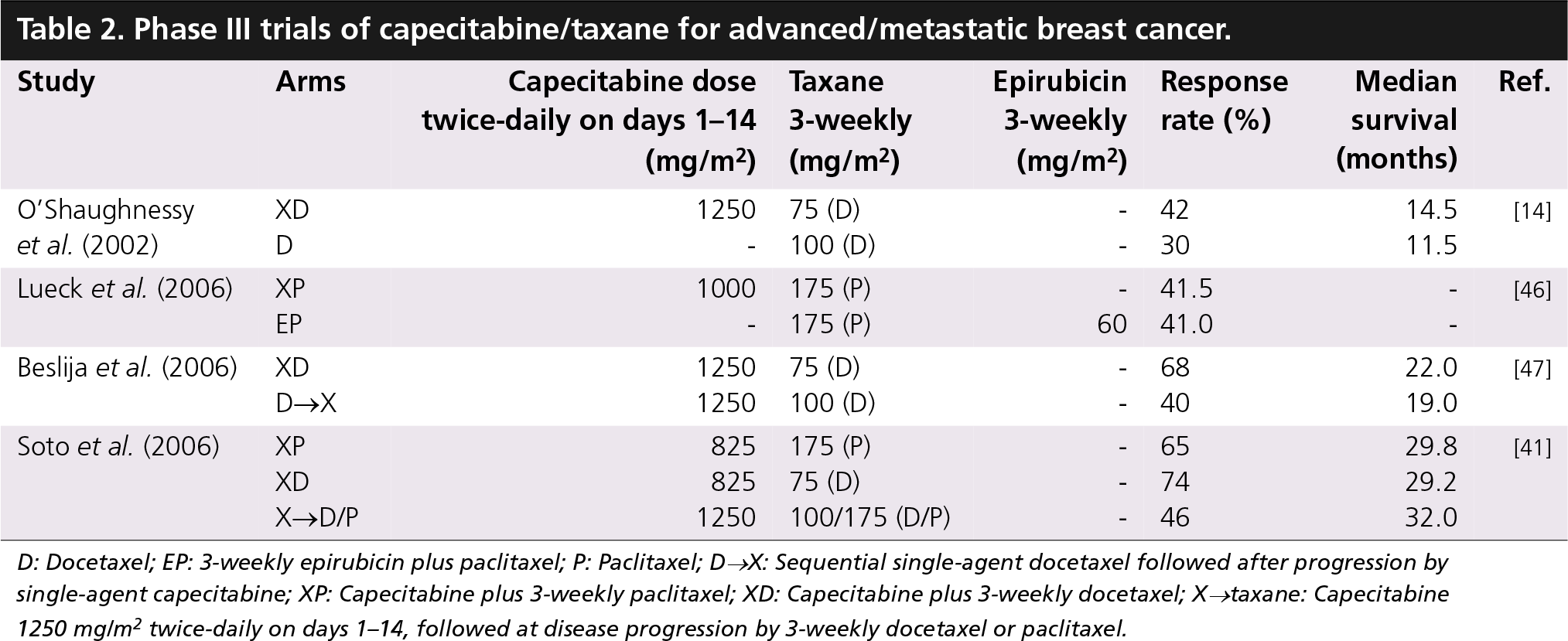
D: Docetaxel; EP: 3-weekly epirubicin plus paclitaxel; P: Paclitaxel; D→X: Sequential single-agent docetaxel followed after progression by single-agent capecitabine; XP: Capecitabine plus 3-weekly paclitaxel; XD: Capecitabine plus 3-weekly docetaxel; X→taxane: Capecitabine 1250 mg/m2 twice-daily on days 1–14, followed at disease progression by 3-weekly docetaxel or paclitaxel.
Docetaxel was the first cytotoxic agent to improve survival over standard salvage regimen (combination) in patients with anthracycline-pretreated MBC [32], and the multicenter, Phase III study, which evaluated docetaxel and capecitabine combination, was the first clinical trial in which a cytotoxic combination regimen provided a significant survival advantage over monotherapy in this patient population and led to the approval of XT for patients with MBC failing anthracycline therapy. Again, this trial persuaded NICE to approve this combination as worthy of recommendation for anthracycline-pretreated or anthracycline-failed MBC. Nevertheless, for clinical practice, this trial does not necessarily confirm that XT upfront is better than T followed by X.
Tolerability & dose evaluation of capecitabine/docetaxel combination therapy
The perceived tolerability of XT has hindered its uptake by some physicians and does limit its applicability for all patients [14]. However, with appropriate dose modification, XT demonstrated a manageable safety profile [14]. Gastrointestinal side effects and hand-foot syndrome were more common with XT combination therapy, whereas myalgia, arthralgia, alopecia and neutropenic fever/sepsis were more common with single-agent docetaxel. More grade 3 adverse events (AEs) occurred with XT therapy (71 vs 49%, respectively), due primarily to the higher incidence of grade 3 hand-foot syndrome, a cutaneous side effect commonly associated with continuous-administration fluoropyrimidines, but which is never life threatening and which can be managed effectively with dose modification. For the significant minority of patients who developed grade 3 or 4 hand-foot syndrome, this is a significant daily problem in the context of a treatment regimen that is palliative in intent. On the other hand, grade 4 events were slightly more common with docetaxel (31 vs 25% with combination), largely as a result of the higher incidence of neutropenic fever with docetaxel monotherapy [14].
The retrospective analysis of O'Shaughnessy's Phase III study, as well as multiple Phase II studies of taxanes with reduced-dose capecitabine, suggests that reducing the starting dose of capecitabine with docetaxel is a reasonable strategy for the treatment of patients with MBC [39]. By reducing capecitabine and docetaxel to 75% of the starting dose (from 1250 to 1000 mg/m2 and from 75 to 60 mg/m2, respectively), the proportion of treatment cycles with grade 3 or 4 treatment-related AEs was approximately halved [39,40]. The Kaplan-Meier curves for TTP and OS in patients with and without XT dose reductions (cycle 2 onwards) were similar, indicating that capecitabine and docetaxel dose reduction did not compromise efficacy in terms of these end points (Figure 1) [39]. Based on retrospective analysis of the Phase III trial reported by O'Shaughnessy et al., a lower capecitabine starting dose (1000 mg/m2 twice-daily) is recommended in patients aged 60 years and over receiving XT. In addition, in a randomized, Phase III trial by Soto et al., a lower capecitabine dose (825 mg/m2) in the XT combination demonstrated high activity but better tolerability than in the O'Shaughnessy trial [41].
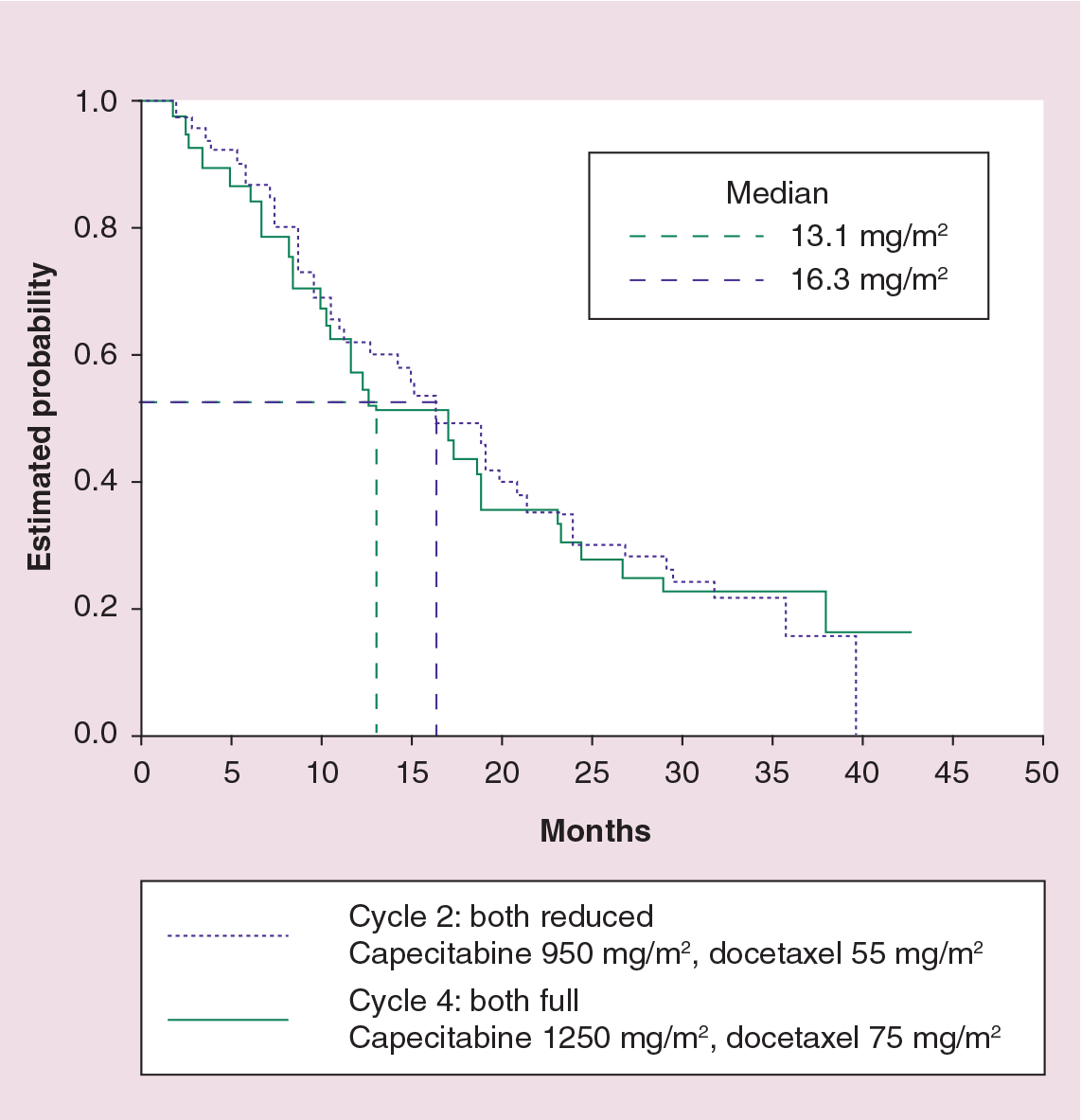
Survival curves comparing capecitabine/docetaxel versus docetaxel in different dose reduction.
Lower initial doses of capecitabine and docetaxel are being prospectively evaluated in the neo-/adjuvant setting. Preliminary reports indicate that the frequency and severity of side effects is reduced with the lower doses, but efficacy of XT is not compromised [42,43]. However, it should be emphasized, that in the pivotal trial in MBC, all patients were allocated full-dose capecitabine for their first course [39].
Cost- & performance-effectiveness of capecitabine/docetaxel combination therapy
Home-based therapy with oral capecitabine has a number of advantages over intravenous hospital-based chemotherapy regimens, including improvement in patients' QoL, and medical resource/cost savings compared with intravenous regimens. In addition, the ability of capecitabine and docetaxel to extend survival beyond docetaxel in patients with previously treated MBC means that XT is a cost-effective combination. For the optimal use of oral capecitabine, effective patient education is crucial. Numerous methods have shown good results, including the use of treatment diaries, regular telephone calls, specialist oral chemotherapy clinics, and information booklets [44,45].
Verma et al. evaluated the cost-effectiveness of the XT combination versus docetaxel monotherapy, comparing the gain in quality-adjusted survival with associated healthcare costs [16]. The survival benefit with the XT regimen is achieved at a small incremental cost. The total medical-resource utilization cost per patient was 8.9% higher with the combination. Patients receiving the XT combination therapy consulted healthcare professionals more frequently regarding AEs than patients receiving docetaxel alone. Clinical toxicity can be a significant problem with this regimen and improving patient education may play an important role in helping patients to recognize side effects and their severity, enabling them to take action to avoid development of more severe toxicity [16]. Another French multicenter, randomized study estimated the cost-effectiveness ratio of adopting XT combination therapy in place of docetaxel alone [17]. In addition to efficacy data, medical-resource consumption related to AEs was also collected in this trial. The addition of capecitabine to docetaxel resulted in an increase in median survival of 90 days (p = 0.0126) and increase in the duration of progression-free survival (PFS) of 58 days (p = 0.0001) compared with docetaxel alone. The total medical cost per patient was evaluated at €11,786 on average IC95% = (€10,982-€12,591) in XT arm versus €11,570 IC95% = (€10,719-€12,421) in monotherapy (p = 0.642). Moreover, the additional cost per year of life saved was estimated at €952 and the cost per year without progression of the disease was established at €1198 [17].
Further capecitabine/taxane combinations & sequenced therapy
In a recent Phase III study, capecitabine plus 3-weekly paclitaxel (XP) (capecitabine 1000 mg/m2 twice-daily on days 1–14 plus paclitaxel 175 mg/m2 on day 1 of a 21-day cycle) showed non-inferiority with epirubicin plus paclitaxel (EP) regimen (epirubicin 60 mg/m2 plus paclitaxel 175 mg/m2, both on day 1 of a 21-day cycle) in first-line MBC in PFS (12.3 vs 11.8 months, respectively) and responce rate (RR) (41.5 vs 41.0%, respectively) (Table 2) [46]. Febrile neutropenia and cardiac toxicity were higher in the EP arm, while grade 3 skin toxicity was seen in 3% of the XP arm [46].
An open-label, single-center, randomized trial of XT (capecitabine 1250 mg/m2 twice-daily on days 1–14 plus docetaxel 75 mg/m2 on day 1) versus sequential T→X, sequential single-agent docetaxel (docetaxel 100 mg/m2 on day 1 of a 21-day cycle) followed after progression by single-agent capecitabine (capecitabine 1250 mg/m2 twice-daily on days 1–14), as first-line therapy for MBC was recently presented [47]. XT demonstrated statistically superior efficacy versus sequential T→X in RR (68 vs 40%; p = 0.004), TTP (9.3 vs 7.7 months; p = 0.001) and OS (22.0 vs 19.0 months; p = 0.006) (Table 2) [47].
A Mexican Oncology Study Group (MOSG) randomized Phase III trial, in which 368 patients with anthracycline-pretreated MBC were randomized to receive one of the following 3-weekly regimens: capecitabine 825 mg/m2 twice-daily on days 1–14, plus paclitaxel 175 mg/m2 on day 1 (XP); or capecitabine 825 mg/m2 twice-daily on days 1–14, plus docetaxel 75 mg/m2 on day 1 (XT); capecitabine 1250 mg/m2 twice-daily on days 1–14, followed at disease progression by docetaxel 100 mg/m2 or paclitaxel 175 mg/m2 on day 1 (X→taxane), demonstrated that XP was as effective as XT: RR: 65 versus 74%; median PFS: 6.7 versus 8.1 months; median OS: 29.8 versus 29.2 months in the XP and XT groups, respectively [41]. Both of the combined therapies were generally well tolerated, with a predictable safety profile such as hand-foot syndrome and diarrhea [41]. The third arm, sequential X→taxane, single-agent capecitabine achieved less RR (46%) compared with XP and XT, and 59 (65%) patients received a sequential taxane at progression. In final analyses, the X→taxane arm resulted in similar median PFS (8.4 months) and median OS (32.0 months) (Table 2) [41].
As first-line treatment for MBC, weekly paclitaxel plus capecitabine was evaluated [48]. Participants (n = 55) received capecitabine 825 mg/m2/dose orally twice-daily (1650 mg/m2/day) for days 1–14 and paclitaxel 80 mg/m2 was administered intravenously weekly on days 1 and 8. Cycles were repeated every 3 weeks. In the intent-to-treat population, objective responses were achieved in 30 patients (55%; 95% CI: 40–69%), and six additional patients had stable disease for 6 months or longer (clinical benefit rate of 65%). The median duration of response was 10 months (range: 2.5–18.7 months). Dose modifications and reductions were common, particularly for capecitabine, leading to a delivered dose intensity of 75% for capecitabine and 91% for paclitaxel. The most frequent grade 3 to 4 treatment-related AEs were hand-foot skin reaction (n = 10), neutropenia (n = 7), fatigue (n = 4), and leukopenia, diarrhea and pain (n = 3 for each).
Somer et al. designed a Phase II study to test the safety and efficacy of nabpaclitaxel (nanoparticle albumin-bound paclitaxel [ABX]) (125 mg/m2 intravenously on days 1 and 8) plus capecitabine (825 mg/m2 orally twice-daily on days 1–14 on an every-3-week cycle) given in a novel combination schedule as first-line treatment for MBC (n = 43) [49]. In total, 37% received prior adjuvant anthracycline and 33% recieved prior adjuvant taxane. The incidence of grade 1–2 neuropathy was 25% (no grade 3–4). Ten patients had grade 3–4 nonhematologic AEs: three hand-foot syndrome, four fatigue and three gastrointestinal. Hematologic AEs included four with grade 3 and one with grade 4 neutropenia, and two with grade 4 febrile neutropenia. Of 38 patients available for analysis of response, the overall response rate was 47.5%: partial response (PR) 39.5%, complete response (CR) 8%. In total, 12 patients had stable disease and 20 patients had completed six or more cycles.
Potential role of the capecitabine/docetaxel regimen for HER2-positive breast cancer
Adding trastuzumab to a chemotherapy agent in HER2-positive MBC provides significant clinical benefit, including prolonged survival. Taxanes or vinorelbine plus trastuzumab are among the most widely applied options in the first-line setting in HER2-positive advanced breast cancer. Recent studies have evaluated the efficacy and tolerability of capecitabine plus trastuzumab after anthracycline and docetaxel or vinorelbine failure and prior trastuzumab exposure [50–53]. Bartsch et al. examined 40 patients with capecitabine (1250 mg/m2 twice-daily for 14 consecutive days in 3-week cycles, with dose modifications if necessary) plus trastuzumab, administered every 3 weeks [50]. TTP was a median of 8 months and overall survival was 24 months. No significant difference was found for second-line and beyond second-line treatment. A CR was observed in 2.5%, PR in 17.5%, stable disease (SD) lasting for at least 6 months in 50%, resulting in a clinical benefit rate (CR + PR + SD > or = 6 months) of 70%. Diarrhea (5%) and hand-foot syndrome (15%) were the only treatment-related AEs that occurred with grade 3 or 4 intensity [50].
In a Japanese trial, 59 patients were enrolled to determine the response rate and toxicity profile of trastuzumab and capecitabine in women with HER2-overexpressing advanced breast cancer [51]. The response rate was 65.0% in patients treated as first-line therapy for metastatic disease and 62.5% among HER2-positive patients, while high response rates were also seen in women treated with second- or third-line therapy. Patients receiving trastuzumab and capecitabine as first-line therapy had a longer TTP than patients receiving this treatment as second- or third-line therapy (median TTP: 280 vs 130 days; p < 0.05). Furthermore, patients receiving trastuzumab and capecitabine as first-line therapy had longer OS than patients receiving this treatment as second- or third-line therapy (median OS: 780 days vs 480 weeks; p < 0.05) [51].
A German, Phase II study has also confirmed activity and feasibility of capecitabine and trastuzumab in combination in HER2-overexpressing advanced/MBC [52]. In total, 27 patients with HER2-overexpressing MBC previously treated with anthracyclines and/or taxanes received oral capecitabine 1250 mg/m2 twice-daily for 14 days followed by a 7-day rest period combined with intravenous trastuzumab 4 mg/kg body weight on day 1 (loading dose) followed by 2 mg/kg weekly. Capecitabine/trastuzumab treatment achieved objective responses in 12 patients (45%), including CR in four patients (15%) and PR in eight patients (30%). Disease was stabilized in an additional nine patients (33%). The median OS time was 28 months and the median PFS time was 6.7 months. The safety profile of the combination was favorable and predictable, with a low incidence of grade 3/4 AEs. The most common AEs were pain, hand-foot syndrome and gastrointestinal toxicities. Severe myelosuppression was rare and severe alopecia did not occur.
Xu et al. evaluated the efficacy and safety of capecitabine plus trastuzumab in first-line MBC [53]. Patients (n = 90) received capecitabine 1250 mg/m2 twice-daily on days 1–14 every 3 weeks and trastuzumab, which was administered as a 4-mg/kg loading dose followed by 2 mg/kg intravenously weekly. In total, 43 patients are evaluable and 47 are still being analyzed. Prior treatment included surgery 77%, radiotherapy 21% and adjuvant chemotherapy 58% (including anthracyclines 35%, paclitaxel 7%, docetaxel 7% and other 21%). ORR was 63%, including five CRs and 22 PRs. At a median follow-up of 6 months, median PFS has not been reached. Most common grade ½ AEs were hand-foot syndrome 14%, neutropenia 14%, serum glutamic-oxaloacetic transaminase abnormality 16% and serum glutamate pyruvate transaminase abnormality 14%. Grade 3 hand-foot syndrome occurred in four patients (9%) and grade 3 myelosuppression affected one patient (2%) [53].
Capecitabine plus trastuzumab appears to be active and well tolerated in heavily treated, and as first-line treatment, for HER2-positive MBC.
Role of the capecitabine/docetaxel regimen for neoadjuvant/adjuvant therapy
In the neoadjuvant setting, several Phase II and III studies of different capecitabine/taxane regimens have confirmed the high activity and acceptable safety of the combination. Capecitabine- and taxane-containing combinations have shown high clinical response rates (78–100%) and pathological (p)CR rates (9–21%) in the neoadjuvant setting [42,54–59]. Furthermore, Lybaert et al. performed a Phase II study comparing XT with or without trastuzumab for HER2-positive locally advanced breast cancer. The rate of pCR was 9% in the XT arm and 45% in the XT+trastuzumab arm, respectively, with manageable toxicity by dose reduction [60].
Recently, a randomized Phase III study evaluating XT (capecitabine 1000 mg/m2 twice-daily on days 1–14 plus docetaxel 75 mg/m2 on day 1 of a 21-day cycle) versus AC (doxorubicin 60 mg/m2 and cyclophosphamide 600 mg/m2, both on day 1 of a 21-day cycle) as neoadjuvant treatment demonstrated that XT resulted in significantly superior efficacy compared with AC in clinical response rate (84 vs 65%, respectively; p = 0.003) and pCR rate (21 vs 10%, respectively; p = 0.024) with a manageable safety profile in early breast cancer [61]. Another randomized Phase III trial, ABCSG-24, by Steger et al., comparing TEX versus ET in neoadjuvant treatment of operable breast cancer, is underway, aiming at achieving high rates of pCR [62]. Von Minckwitz et al. also reported safety results from GeparQuattro, a neoadjuvant trial exploring the effect of simultaneous or sequential use of capecitabine with docetaxel after four cycles of epirubicin/cyclophosphamide (EC) as well as simultaneous trastuzumab on pCR of previously untreated stage I-III breast cancers, at the ASCO Breast Cancer Symposium in 2007 [64]. Hematological toxicities were more frequent with docetaxel (100 mg/m2) alone whereas nonhematological toxicity increased step by step with the sequential and simultaneous addition of capecitabine. Simultaneous addition of trastuzumab to EC/docetaxe/capecitabine was feasible without additional cardiotoxicity. No safety concerns were raised and the trial proceeded as planned [63].
As in the metastatic setting, a large, ongoing clinical-trial program is continuing to explore the potential for capecitabine in the treatment of early breast cancer, looking at capecitabine-taxane combinations (US Oncology Trial, German Adjuvant Intergroup Node-Positive study trial, MD Anderson Cancer Center trial), capecitabine maintenance therapy (Coalicion Iberoamericana de Investigacion en Oncologia Mamaria trial), capecitabine for elderly patients (the Cancer and Leukemia Group B 49907 trial, Ibandronate With or Without Capecitabine in Elderly Patients), sequential therapy (Trial of Accelerated Adjuvant Chemo Therapy with capecitabine 2, Grupo Espanol de Investigacion de Cancer de Mama trial), and sequential capecitabine-based combinations (Finnish Phase III Adjuvant Study trial).
Newer combinations Capecitabine or gemcitabine plus docetaxel combination therapy
A recent Phase III trial comparing gemcitabine/docetaxel (GT) with XT for MBC found that GT was not superior to XT in terms of PFS but patients on GT had less toxicity [64]. This study compared GT with XT as first- or second-line treatment in MBC pretreated with an anthracycline. Patients with histologically confirmed MBC who relapsed after an anthracycline-based regimen either in neoadjuvant or first-line metastatic disease were randomized to GD (gemcitabine 1000 mg/m2 on days 1–8; docetaxel 75 mg/m2 on day 1) or XT (capecitabine 1250 mg/m2 twice-daily on days 1–14; docetaxel 75 mg/m2 on day 1) every 21 days. At the interim analysis, 302 patients were evaluable for safety and 305 for response. ORR was 27% for GT and 31% for XT (p = 0.4537). The frequency of CTC grade 3/4 hematologic toxicity was similar in the two arms, but febrile neutropenia was more common in the XT arm (12 vs 7%). Nonhematologic toxicity was low in both arms, but diarrhoea (17 vs 7%), mucositis (16 vs 4%) and hand-foot syndrome (24 vs 0%) were more pronounced in the XT arm. More serious AEs occurred in the XT arm (36 vs 28%), causing discontinuation in 27 (XT) and 14% (GT) of patients. There were two toxic deaths, both in the XT arm.
To better understand how QoL is affected by toxicity and symptoms, Fumoleau et al. conducted an exploratory analysis of patients treated in the trial described above. QoL was assessed every cycle with Rotterdam Symptom Checklist (RSCL). As the physical symptom distress scale (PSDS) includes symptom- and toxicity-related items, distributions of responses to each item were explored. Among the 302 patients who received treatment (GT: n = 152; XT: n = 150), median number of cycles was six for both arms. In total, 267 patients had baseline RSCL data; compliance ranged from 79 to 88% for the first six cycles. Baseline RSCL scores were comparable between arms. No statistical differences between arms were seen for any of the RSCL dimensions (p > 0.05 at all cycles). Both arms had worsening in the PSDS (median increases of 3–6.8 on 69-point scale). By cycle 3, more GT patients reported tiredness (58 vs 47%), lack of energy (45 vs 38%) and back pain (19 vs 9%) and, by cycle 2, alopecia (76 vs 66%). By cycle 1, more XT patients reported tingling hands/feet (15 vs 7%) and burning/sore eyes (14 vs 3%). The authors concluded that this preliminary analysis indicated no QoL differences between GT and XT. However, further exploration shows that physical distress is explained by different symptoms and toxicities in each arm. Further analysis incorporating clinical outcomes may better explain QoL outcomes [65].
Executive summary
Capecitabine/docetaxel combination therapy
A randomized Phase III study demonstrated that the addition of capecitabine to docetaxel (XT) compared with single-agent docetaxel in patients with anthracycline-pretreated MBC resulted in significantly superior OS, with a 3-month improvement in median survival, significantly superior time to disease progression (TTP) and a significantly superior overall response rate, with a manageable safety profile.
To date, the XT combination therapy is indicated in the USA and Europe for the treatment of metastatic breast cancer failing anthracycline therapy, and as monotherapy for metastatic breast cancer resistant to paclitaxel and anthracycline therapy (USA) or after failure of taxanes and an anthracycline-containing regimen, or in patients for whom further anthracycline therapy is not indicated (Europe).
Tolerability & dose evaluation of capecitabine/docetaxel combination therapy
Quality-of-life (QoL) analysis of XT combination therapy was favorable.
Gastrointestinal side effects and hand-foot syndrome were more common with XT combination therapy, whereas myalgia, arthralgia, alopecia and neutropenic fever/sepsis were more common with single-agent docetaxel. This clinical toxicity can be difficult to manage. Consequently, some clinicians favor sequential single-agent therapy for palliation despite the positive QoL and survival results of the pivotal trial.
The retrospective analysis of O'Shaughnessy's Phase III study, as well as studies of taxanes with reduced-dose capecitabine, shows that after the first cycle, reducing the dose of capecitabine to 75% is an appropriate strategy for the treatment of some patients not tolerating the planned starting dose with MBC. In the O'Shaughessy trial, dose modification halved the frequency of grade 3 or 4 treatment-related adverse events, without reducing efficacy.
Cost & performance-effectiveness of capecitabine/docetaxel combination therapy
Pharmacoeconomic modeling using data from the Phase III trial has shown that the XT combination therapy is highly cost effective when compared with other cancer treatments that improve survival.
Capecitabine/paclitaxel combination in the first-line treatment of MBC
Phase III studies examining efficacy of capecitabine plus 3-weekly paclitaxel (XP) has also demonstrated high activity in MBC, with similar efficacy to epirubicin/paclitaxel (EP) and capecitabine/docetaxel (XT) regimens.
Capecitabine & taxanes as sequential single agents in the first-line treatment of MBC
A randomized trial of XT versus sequential T→X (sequential single-agent docetaxel followed after progression by single-agent capecitabine) showed that XT achieved statistically superior efficacy versus sequential T→X in RR (68 vs 40%; p = 0.004), TTP (9.3 vs 7.7 months; p = 0.001) and OS (22.0 vs 19.0 months; p = 0.006).
In the Mexican Oncology Study Group randomized Phase III trial, sequential X→taxane demonstrated similar efficacy to XP and XT combinations in terms of PFS (8.4, 6.7 and 8.1 months, respectively) and OS (32.0, 29.8 and 29.2 months, respectively), although response rate was significantly higher with the combination regimens than the single-agent sequential approach.
Role of the capecitabine/docetaxel regimen for neoadjuvant/adjuvant therapy
In the neoadjuvant setting, several Phase II studies of capecitabine/taxane regimens have demonstrated high clinical response rates (78–100%) and pathological complete response (pCR) rates (9–21 %) in the neoadjuvant setting.
A randomized, Phase III study evaluating XT versus AC as neoadjuvant treatment showed that XT resulted in significantly superior efficacy in terms of clinical response rate (84 vs 65%; p = 0.003) and pCR rate (21 vs 10%; p = 0.024) compared with AC, with a manageable safety profile in early breast cancer.
In the adjuvant setting, a large, ongoing trial program is continuing to explore the potential of capecitabine in the treatment of early breast cancer, looking at capecitabine-taxane combinations, capecitabine maintenance therapy, capecitabine for elderly patients, capecitabine in combination with biologic agents, and sequential versus combination therapy.
Future perspective
Challenges for seeking more efficient and manageable regimens to treat breast cancer will continue. New drugs, including antihormonal, cytotoxic and molecular-targeted agents, and their new combinations will be tested.
The search is continuing, with the increasing use of expression arrays and tissue microarrays to predict who will benefit from a particular regimen.
This is even more important if we consider that the increasing number of patients will survive longer to seek the best treatment while maintaining their QoL.
Conclusion
The XT regimen for MBC has shown its usefulness in terms of the efficacy, flexibility and cost-effectiveness. A randomized Phase III study demonstrated that the addition of capecitabine to docetaxel compared with single-agent docetaxel in patients with anthracycline-pretreated MBC resulted in superior OS, including a 3-month median survival benefit, superior TTP and a superior response rate, with a manageable safety profile. To date, XT combination therapy is indicated in the US and Europe for the treatment of MBC failing anthracycline therapy, and as monotherapy for patients with MBC resistant to paclitaxel and anthracycline therapy (USA) after failure of taxanes and an anthracycline-containing regimen, or in patients for whom further anthracycline therapy is not indicated (Europe). Randomized trials have also compared the efficacy of docetaxel and paclitaxel as a partner for capecitabine, and the manner of administration (sequential or combination). Lower initial doses of capecitabine and docetaxel, being retrospectively and prospectively evaluated, demonstrated high activity but better tolerability. Furthermore, clinical trials examining capecitabine and taxane combinations have been conducted in the neoadjuvant and adjuvant settings for breast cancer. Recent results examining the efficacy of addition of trastuzumab to XT in HER2-positive patients were also encouraging.
Many physicians who are concerned regarding the toxicity of treatment in the palliative setting will often avoid the XT combination in favor of the less efficacious but more tolerable sequential single-agents philosophy.
However, there is certainly an argument to explore, in metastatic disease, lower initial dose capecitabine in combination with taxane, and with encouraging data from neoadjuvant study, their combination with trastuzumab for HER2-positive cancers.
Future perspective
Challenges for seeking more efficient and manageable regimens to treat breast cancer will continue. New drugs, including antihormonal, cytotoxic and, especially, molecular-targeted agents, and their new combinations will be tested. At the same time, with the increasing use of expression arrays and tissue microarrays, the search is on to better select patients for particular drug treatments. This is even more important if we consider the increasing number of patients who will survive longer to seek the best treatment while maintaining their QoL.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.