
Abstract
Denosumab (formerly AMG 162) is a fully human monoclonal antibody with a high affinity and specificity for receptor activator of nuclear factor-κB ligand, a cytokine member of the tumor necrosis factor family that is the primary mediator of osteoclastic bone resorption. Increased bone resorption is a prominent feature in the pathogenesis of postmenopausal osteoporosis and other skeletal disorders. Denosumab inhibits the action of receptor activator of nuclear factor-κB ligand, thereby reducing the differentiation, activation and survival of osteoclasts, and slowing the rate of bone resorption. Postmenopausal women with low bone mineral density treated with denosumab have an increase in bone mineral density and a reduction of bone turnover markers that is rapid, sustained and reversible. In patients with multiple myeloma and bone metastases from breast cancer, denosumab reduces bone turnover to a similar magnitude but in a more sustained manner than intravenous pamidronate. Denosumab is well tolerated with adverse events similar to placebo. Denosumab is a promising investigational agent for the management of osteoporosis and other diseases associated with bone loss.
Osteoporosis is a skeletal disease in which low bone strength predisposes affected individuals to an increased risk of low-trauma fractures. It is a common disease with serious consequences. Approximately 30% of postmenopausal Caucasian women have osteoporosis [1], with a lifetime fracture risk of approximately 40% [2]. In 1990, there were an estimated 1.31 million hip fractures worldwide, with 740,000 associated deaths and 1.75 million disability-adjusted life-years lost [3]. Despite widespread recognition of the high prevalence of osteoporosis, these patients are often not recognized and treated. Even patients with fractures, who have a very high risk of future fracture [4], are usually not evaluated or treated for osteoporosis [5]. Healthcare providers are poorly adherent to osteoporosis treatment guidelines [6] and patient adherence to treatment, when initiated, is poor [7]. Better adherence to therapy is associated with greater bone mineral density (BMD) response [8], greater reduction in fracture risk [9] and reduced healthcare costs [7]. While the causes of poor adherence are complex and the solutions difficult, potential pathways to improving adherence include less frequent dosing and simplified drug administration [10].
Denosumab (AMG 162) is an investigational drug that is being studied using 6-month intervals between doses given by subcutaneous injection. Denosumab suppresses bone turnover in healthy postmenopausal women [11] and in patients with multiple myeloma or bone metastases from breast cancer [12]. A Phase II clinical trial showed that it increases BMD in postmenopausal women with low BMD [13]. Clinical trials are ongoing to evaluate its safety and efficacy for the prevention and treatment of postmenopausal osteoporosis and the management of other skeletal diseases associated with bone loss. This article will focus on potential uses of denosumab in the prevention and treatment of postmenopausal osteoporosis.
Overview of osteoporosis treatments
Pharmacological agents for the prevention and treatment of osteoporosis may be categorized as anticatabolic (antiresorptive) or anabolic [14], with some drugs having features in both categories. Anticatabolic drugs (e.g., estrogens, bisphosphonates, selective estrogen receptor modulators [SERMs] and calcitonin) improve bone strength and reduce fracture risk largely by reducing bone turnover, which decreases the number of bone multicellular units (BMUs), thereby preserving bone microarchitecture, reducing trabecular perforation and decreasing cortical porosity [15]. The BMD increase associated with anticatabolic therapy is probably initially due to filling in of the remodeling space and subsequently due to prolonged secondary mineralization [16]. Anabolic agents (e.g., teriparatide and recombinant human parathyroid hormone [rhPTH 1–84]) increase bone strength and reduce fracture risk by increasing bone mass through an increase in the number and activity of BMUs, with some evidence for restoration of lost microarchitectural elements and increases in bone size [16]. Strontium ranelate (SR), which has also been shown to reduce fracture risk, increases BMD by virtue of incorporation into bone (SR has a higher atomic weight than calcium), as well as having effects on bone cell metabolism [17]. While the pharmacological properties and mechanisms of action of these drugs vary according to drug class and the individual agent, all have effects on bone turnover. Denosumab is an anticatabolic drug that acts directly on the receptor activator of nuclear factor-κB ligand (RANKL)/receptor activator of nuclear factor-κB (RANK)/osteoprotegerin (OPG) signaling pathway, which regulates bone resorption [11].
RANKL/RANK/OPG signaling pathway
The adult skeleton is continuously being broken down and reformed in a dynamic process known as bone remodeling. This occurs due to the coordinated or ‘coupled’ action of osteoclasts and osteoblasts in discrete packets (BMUs) located on the surface of trabecular bone and in Haversian systems of cortical bone. When bone resorption exceeds bone formation, as is commonly seen in early postmenopausal women, bone loss occurs and osteoporosis may eventually be the result [18]. While many systemic and local factors participate in the regulation of bone remodeling, the RANKL/RANK/OPG signaling pathway (Figure 1) is the principal final mediator of bone resorption [19]. RANKL, expressed on the surface of osteoblasts and in soluble form after cleavage from the cell surface or secretion from T cells [20], is a cytokine member of the tumor necrosis factor (TNF) superfamily. When RANKL binds to its membrane-bound receptor, RANK, found on osteoclasts and their precursors, it promotes osteoclast differentiation, activity and survival, which in turn stimulates bone resorption. OPG, another member of the TNF receptor superfamily, is a soluble nonsignaling ‘decoy receptor’ that binds to RANKL, inhibiting osteoclastogenesis and decreasing the survival of existing osteoclasts [21]. Although soluble RANKL and OPG levels can be measured in serum, correlation of serum levels with clinical disorders has been variable. An increase in the RANKL:OPG ratio has been implicated in the pathogenesis of postmenopausal osteoporosis, as well as bone disease associated with multiple myeloma, metastatic bone disease, treatment-related bone loss, rheumatoid arthritis, hyperparathyroidism, Paget's disease of bone and familial expansile osteolysis [22].

Denosumab action on the RANKL/RANK/OPG regulatory pathway.
The role of RANKL, RANK and OPG in nonskeletal organ systems, particularly the immune system, is an area of active investigation. In addition to its expression by osteoblasts and their precursors, RANKL is expressed by endothelial cells, stromal cells, primitive mesenchymal cells surrounding cartilage, chondrocytes, activated T lymphocytes and immature CD4/CD8 thymocytes. RANK is expressed on the surface of chondrocytes, mammary gland epithelial cells, trophoblast cells, dendritic cells and mature T cells, as well as on the surface of osteoclasts. OPG is produced and released by cells that include osteoblasts, dendritic cells and lymphocytes, and OPG is expressed in organs that include the heart, lung, spleen, thymus, kidney and intestine [23]. Many chronic inflammatory diseases are associated with systemic and focal bone loss that may be mediated through an imbalance in components of the immune system that participate in the regulation of the RANKL/RANK/OPG pathway [24]. The potential immunomodulatory effects of the RANKL/RANK/OPG pathway have raised concerns that perturbations of the pathway might have adverse effects on immune function [25]. Animal studies suggest that the pathway is critical for the development of an intact immune system. For example, RANK-knockout mice are deficient in splenic B cells and have impaired lymph-node organogenesis [26]. However, in adults with a fully developed immune system, there is evidence to suggest that the RANKL/RANK/OPG system has a nonessential role for immune function. Rats and mice overexpressing OPG had no impairment of immunological parameters or lymphocyte function [27]. Studies of RANKL inhibition in humans have also shown no evidence of impaired immunological function [11,13,28].
There is some evidence to suggest that RANKL/RANK/OPG may play a role in the pathogenesis of vascular calcification, a common comorbidity in osteoporosis patients, with RANKL accelerating and OPG inhibiting its development [20]. Preclinical studies have demonstrated that the administration of recombinant OPG reduces the growth of breast cancer cells, while OPG overexpression in breast cancer cells has been shown to enhance tumor growth [29]. In an animal model of prostate carcinoma, RANKL inhibition slowed the progression of skeletal metastases [30]. RANKL has been shown to trigger the migration of human epithelial cancer cells and melanoma cells, suggesting that inhibition of RANKL may offer protection against tumor metastasis and progression in bones [31].
Pharmacokinetic properties of denosumab
Denosumab is a fully human monoclonal antibody of the immunoglobulin (Ig)G2 isotype. It has a high affinity and specificity for human RANKL, thereby blocking the binding of RANKL to RANK in a manner similar to native OPG (Figure 1). It does not bind to TNF-α, TNF-β, TNF-related apoptosis-inducing ligand (TRAIL) or CD40 ligand. The pharmacokinetics of denosumab are nonlinear with dose and similar to other fully human IgG2 monoclonal antibodies. In a Phase I dose-escalation trial in healthy postmenopausal women given a single subcutaneous dose of densosumab (0.01–3.0 mg/kg) [11], three phases were observed:
A prolonged absorption phase with maximum serum concentration (Cmax) observed at 5–21 days post dose, increasing as dose increased
A prolonged β-phase, with a serum half-life as long as 32 days with the maximum dose
A rapid terminal phase during which the serum concentration dropped below 1000 ng/ml
In a study of patients with multiple myeloma or breast cancer metastatic to bone, a single subcutaneous injection of denosumab 1 or 3 mg/kg resulted in serum levels detectable as early as 1 h post dose and a mean serum half-life of 33.3 days, with suppression of bone resorption markers within 1 day that persisted to at least 84 days [12]. Postmenopausal women with low BMD given subcutaneous denosumab 60 mg (the dose being used in the Phase III osteoporosis clinical trials every 6 months) were found to have a median time to maximum concentration (Tmax) after the first dose of 26 days (range 3–32 days) [32]. In comparison with OPG–Fc studied in postmenopausal women [28] and patients with multiple myeloma or bone metastases due to breast carcinoma [33], denosumab is a more potent antiresorptive agent with a longer duration of antiresorptive effect using similar doses. The duration of denosumab's antiresorptive effect is a function of both its long half-life, which is typical for IgG2 antibodies [34], and its effects on osteoclast recruitment, function and survival.
Preclinical studies of RANKL inhibition
The rationale for the clinical use of denosumab is based on extensive preclinical data documenting the key role of the RANKL/RANK/OPG signaling pathway in the regulation of bone remodeling and, in particular, RANKL inhibition to reduce bone resorption. Since denosumab does not recognize or neutralize mouse or rat RANKL, studies of RANKL inhibition with these animals have utilized OPG–Fc or RANK–Fc, fusion molecules of recombinant OPG or RANK with the Fc fragment of IgG. In vitro, RANKL induces osteoclast-like cell formation in cell cultures [35], while recombinant OPG inhibits osteoclast differentiation in a dose-dependent manner [21]. Osteotropic hormones and cytokines are capable of regulating the expression of RANKL and OPG in human-derived osteoblast cell lines [36]. Recombinant OPG prevents bone loss associated with ovariectomy in rats [21]. Overexpression of OPG in transgenic mice and administration of recombinant OPG to normal mice decreases osteoclast differentiation and results in a nonlethal osteopetrosis (or osteopetrotic) phenotype [21]. OPG-knockout mice develop osteoporosis and fractures [37]. RANKL-knockout mice [38] and RANK-knockout mice [39] have a total absence of osteoclasts and develop osteopetrosis. In young male rats, RANKL inhibition has been shown to increase bone mineralization and improve mechanical strength in the femur [40]. A study of aged ovariectomized rats demonstrated that treatment with a combination of recombinant rat OPG and PTH increased BMD more than either agent alone [41], suggesting an additive effect that has not been observed with other combinations of antiresorptive and anabolic agents. These studies and others have suggested that RANKL inhibition may have a therapeutic role in the management of osteoporosis and other skeletal disorders.
Clinical efficacy & safety of RANKL inhibition with OPG
A Phase I randomized, double-blind, placebo-controlled, sequential dose-escalation study evaluated the safety, tolerability and antiresorptive effect of OPG–Fc in 52 healthy postmenopausal women [28]. The subjects received a single subcutaneous dose of OPG–Fc 0.1, 0.3, 1 or 3 mg/kg, or placebo, and were then followed for 84 days. All subjects were monitored by physical exams and laboratory studies that included hematology, blood chemistries, coagulation studies, Igs, T-cell enumeration (CD3, CD4 and CD8), neutralizing antibodies to OPG and bone-turnover markers. At the highest administered dose (3 mg/kg), urinary N-tel-opeptide, a marker of bone resorption, decreased within 12 h of dosing, with maximum suppression of approximately 80% below baseline after 3 days. N-telopeptide then began to rise, so that a mean decrease of 14% below baseline was observed at 6 weeks. Serum bone-specific alkaline phosphatase (BSAP), a marker of bone formation, did not change until approximately 3 weeks after dosing, reaching a nadir of 30% below baseline at approximately 6 weeks with the 3 mg/kg dose. The pattern of change in the resorption and formation markers was consistent with findings in preclinical studies. This suggests that OPG–Fc acts primarily by decreasing the activation frequency of BMUs and does not have a direct effect on bone formation. This study demonstrated for the first time that a single dose of OPG–Fc could cause a rapid, reversible and dose-dependent suppression of bone resorption. OPG–Fc was not associated with serious adverse events, dropouts due to adverse events, or identification of neutralizing antibodies to OPG. The most common adverse event was a mild injection-site reaction. The findings of this study initiated further clinical investigation of RANKL inhibition as a potential therapeutic agent for disorders of skeletal health. Denosumab, a fully human monoclonal antibody to RANKL that acts in a similar way to OPG, was selected for further development due to its greater antiresorptive potency and longer duration of action compared with OPG–Fc.
Clinical efficacy of denosumab for prevention & treatment of postmenopausal osteoporosis
A single-dose, randomized, double-blind, placebo-controlled, dose-escalation study of denosumab was conducted in 49 healthy postmenopausal women who were given a single subcutaneous dose of denosumab 0.01, 0.03, 0.1, 0.3, 1 or 3 mg/kg, or placebo [11]. They were followed for up to 6 months in all cohorts and up to 9 months in the three highest dose cohorts. The primary objectives were to assess drug safety and tolerability, the effect on bone-turnover markers, and pharmacokinetics. The effect on suppression of bone resorption, as measured by urinary N-telopeptide, was dose-dependent, rapid (within 12 h, the earliest time point measured), profound (up to 84% decrease from baseline), sustained (up to 6 months) and reversible (rise in N-telopeptide at the end of the monitoring period). Suppression of serum BSAP occurred later and was less pronounced than was observed for N-telopeptide. Further study was undertaken to determine the effects of denosumab on BMD.
The efficacy and safety of denosumab were evaluated in a Phase II randomized, placebo-controlled, dose-ranging study of 412 postmenopausal women with a low BMD T-score of −1.8 to −4.0 at the lumbar spine or −1.8 to −3.5 at the total hip or femoral neck. The subjects were randomized to nine groups (41–54 subjects/group) receiving subcutaneous denosumab 6, 14 or 30 mg every 3 months; subcutaneous denosumab 14, 60, 100 or 210 mg every 6 months; open-label alendronate 70 mg weekly; or placebo. The primary end point was percentage change in lumbar spine BMD at 12 months compared with baseline. Bone turnover was assessed by measurement of serum and urine telopeptides, and BSAP. Denosumab treatment for 12 months resulted in a BMD increase of 3–6.7% at the lumbar spine compared with baseline, while there was a 0.8% loss with placebo (p < 0.001) (Figure 2A). At the total hip there was a BMD increase of 1.9–3.6% compared with baseline, with a 0.6% loss in the placebo group (p < 0.001) (Figure 2B). At the distal one-third radius, there was a BMD increase of 0.4–1.3% with denosumab, compared with a 2% loss with placebo (p < 0.001). In exploratory comparisons with alendronate, the BMD changes were at least as great with denosumab, with an apparently greater BMD increase at the total hip and distal one-third radius with denosumab 30 mg every 3 months and 60 mg every 6 months. Denosumab groups showed a decrease in serum C-telopeptide compared with placebo (p < 0.001) as early as 3 days, the first scheduled time of C-telopeptide measurement. Serum C-telopeptide suppression reached a maximum mean decrease of 88% compared with 5% with placebo (Figure 2C). The effects on urinary N-telopeptide were similar to those on serum C-telopeptide. The suppression of BSAP with denosumab was significant compared with placebo (p < 0.001) (Figure 2D), but was delayed by approximately 1 month compared with C-telopeptide. The suppression of bone turnover was dose-dependent, rapid, sustained and reversible. These data suggest that denosumab 60 mg every 3 months and 30 mg every 3 months are associated with maximum therapeutic benefit and minimal exposure dose. The dose of 60 mg every 6 months, having the longer dosing interval, was selected for further investigation in the management of postmenopausal osteoporosis.
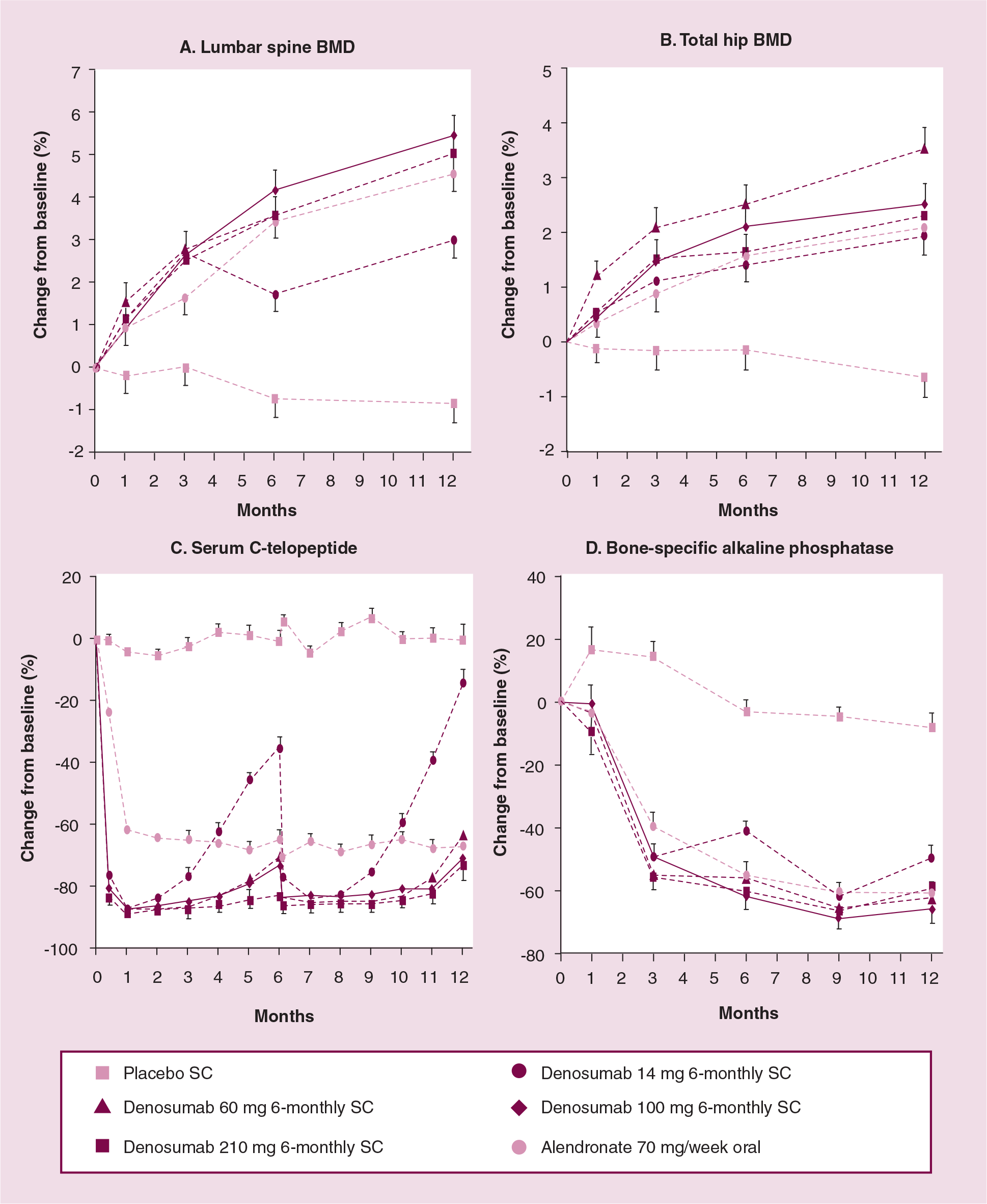
Changes in BMD and bone turnover markers over 12 months with 6-monthly denosumab.
Phase III trials are now in progress to evaluate the safety and efficacy of denosumab for:
Reducing vertebral fracture risk in women with postmenopausal osteoporosis
Preventing bone loss in postmenopausal women with low BMD (osteopenia)
Preventing bone loss in women with nonmetastatic breast cancer who are receiving aromatase-inhibitor therapy
Preventing bone loss in men with nonmetastatic prostate cancer who are receiving androgen-deprivation therapy
In addition, Phase II clinical trials are ongoing to evaluate the use of denosumab in patients with rheumatoid arthritis, bisphosphonate-naive breast cancer and advanced cancer metastatic to bone who are receiving intravenous bisphosphonates.
Safety & tolerability of denosumab
In the Phase I study of denosumab in healthy postmenopausal women (n = 49), no related serious adverse events were reported, and no subjects were discontinued from the study due to adverse events [11]. Mild, transient, dose-dependent decreases in albumin-adjusted serum calcium and corresponding increases in serum intact PTH levels were measured. Reported infectious events were similar with denosumab (38% for all treatment groups) and placebo (33%). Two subjects, receiving denosumab 1 and 3 mg/kg, had mild injection-site reactions. There were no denosumab-associated changes in white blood cell (WBC) counts, T-, B- or natural killer (NK)-cell counts (CD3, CD4, CD8, CD20 or CD56), Igs or coagulation parameters.
In the denosumab Phase II study, there was a small, transient, asymptomatic, nondose-dependent decrease in the mean albumin-adjusted serum calcium levels in patients treated with denosumab (n = 314 for all groups) compared with placebo (n = 46) and alendronate (n = 46) [13]. There was an increase in mean serum intact PTH with denosumab and alendronate compared with placebo, returning toward baseline over time. No significant differences were observed in the percentage of subjects having adverse events with denosumab, placebo or alendronate, with the exception of dyspepsia, which was most common with open-label alendronate. Two subjects receiving denosumab 100 mg every 6 months developed transient, non-neutralizing, denosumab-binding antibodies. In a subset of denosumab-treated subjects assessed for immune function, there were no clinically meaningful changes in WBC counts, T-, B- or NK-cell (CD3, CD4, CD8, CD19 and CD16/56) numbers at 1 year [42]. There is no evidence in the Phase II study data that denosumab is associated with an increased risk of infection, malignancy, oversuppression of bone turnover or impaired fracture healing. There have been no reported cases of osteonecrosis of the jaw with denosumab. The ongoing Phase III clinical trials will evaluate safety parameters in larger numbers of patients.
Regulatory issues
Denosumab is an investigational drug that is not currently approved for clinical use.
Conclusion
Denosumab is a fully human monoclonal antibody to RANKL that reduces bone turnover and increases BMD in postmenopausal women with low BMD. Its effects on suppression of bone resorption are rapid, sustained and reversible. Adverse events in Phase II clinical trials are similar to placebo. It is currently under investigation as an agent for the prevention and treatment of osteoporosis, and for the treatment of other skeletal diseases associated with bone loss.
Future perspective
Preliminary data suggest that denosumab is a potentially effective and safe agent for the management of osteoporosis and other skeletal disorders associated with bone loss. Dosing at 6-month intervals may be more convenient and improve adherence to therapy compared with less frequent dosing. Subcutaneous dosing may be more attractive for clinicians than intravenous dosing, since the time and office resources for administration are less. More data are needed to confirm the efficacy, safety, adherence and clinical utility of denosumab.
Executive summary

Denosumab is a fully human monoclonal antibody to receptor activator of nuclear factor-κB ligand (RANKL), the principal mediator of osteoclastic bone resorption.
Denosumab blocks the binding of RANKL to its receptor activator of nuclear factor-κB (RANK), thereby inhibiting osteoclast differentiation, activity and survival.
The pharmacokinetics of denosumab are nonlinear with dose and similar to other fully human monoclonal antibodies of the immunoglobulin G2 class.
Serum levels in healthy postmenopausal women after single subcutaneous doses ranging from 0.01–3 mg/kg showed three phases: a prolonged absorption phase with maximal serum concentrations observed at 5–21 days postdose, increasing as dose increased; a prolonged β-phase, with serum half-life as long as 32 days with the maximum dose; and a rapid terminal phase during which serum concentration dropped below 1000 ng/ml.
Denosumab does not bind to tumor necrosis factor (TNF)-α, TNF-β, TNF-related apoptosis-inducing ligand or CD40 ligand.
Denosumab results in a dose-dependent increase in bone mineral density (BMD) in postmenopausal women with low BMD.
Suppression of bone resorption is rapid, sustained and reversible.
Efficacy for the prevention of postmenopausal osteoporosis and reduction of fracture risk in women with this condition is under investigation.
Efficacy in the treatment of other skeletal disorders associated with bone loss is under investigation.
No significant differences in safety and tolerability end points have been observed in a Phase II clinical trial with denosumab compared with placebo.
Phase III clinical trials will evaluate safety and tolerability end points in a larger number of subjects.
There are no known drug interactions with denosumab.
Denosumab at a subcutaneous dose of 60 mg every 6 months is under investigation for the prevention and treatment of postmenopausal osteoporosis and the treatment of other skeletal disorders associated with bone loss.