
Abstract
Numerous studies have reported on cancers among Mayak Production Association (PA) nuclear workers. Other studies have reported on serious deterministic effects of large radiation doses for the same population. This study relates to deterministic effects (respiratory system dysfunction) in Mayak workers after relatively small chronic radiation doses (alpha plus gamma). Because cigarette smoke is a confounding factor, we also account for smoking effects. Here we present a new empirical mathematical model that was introduced for simultaneous assessment of radiation and cigarette-smoking-related damage to the respiratory system. The model incorporates absolute thresholds for smoking- and radiation-induced respiratory system dysfunction. As the alpha radiation dose to the lung increased from 0 to 4.36 Gy, respiratory function indices studied decreased, although remaining in the normal range. The data were consistent with the view that alpha radiation doses to the lung above a relatively small threshold (0.15 to 0.39 Gy) cause some respiratory system dysfunction. Respiratory function indices were not found to be influenced by total-body gamma radiation doses in the range 0–3.8 Gy when delivered at low rates over years. However, significant decreases in airway conductance were found to be associated with cigarette smoking. Whether the indicated cigarette smoking and alpha radiation associated dysfunction is debilitating is unclear.
INTRODUCTION
Workers at the Mayak Plutonium Production Facility (Mayak PA) were chronically exposed over years to alpha (from inhaled 239Pu) and gamma radiations as a result of their occupational setting (Khokhryakov et al. 2000a). Numerous studies have focused on dosimetry and cancer induction among the Mayak PA workers (Tokarskaya et al. 1995; Vasilenko et al. 2000; Khokhryakov et al. 2000a,b; Gilbert et al. 2001; Suslova et al. 2002; Hahn et al. 2003; Shilnikova et al. 2003; Tokarskaya et al. 2006). It is also important to study morbidity endpoints other than cancer. Since the lung is a primary deposition site for inhaled Pu aerosols, this study focuses on respiratory function abnormalities among the Mayak PA workers. The function of the respiratory system is influenced by different agents that include internal and external radiation, inhaled particles from forest and other fires, and airborne chemical toxicants (including cigarette smoke), and is influenced by age and body mass (Balmes et al. 2003; Anderson et al. 1997; Samet and Lange 1996; Higenbottam et al. 1980; Knudson et al. 1987; Lebowitz et al. 1987).
Radiation doses to pulmonary tissue in the range of 20–30 Gy induce fibrosis and radiation pneumonitis and cause respiratory system dysfunction in patients during fractionated radiotherapy treatment of lung cancer (Abratt and Morgan 2002), after total body irradiation before bone marrow transplantation (Thomas et al. 2001), and in experiments where dogs inhaled large amounts of insoluble 239PuO2 (Muggenburg et al. 1996).
High-level alpha radiation exposure of humans occurred as a result of lax radiation protection practices during the early years of operation of the Mayak PA (Koshurnikova et al. 1999; Khokhryakov et al. 2002). In some cases this led to plutonium pneumosclerosis, whose clinical characteristics and associated radiation doses are discussed in several publications (Ilyin 2005; Okladnikova et al. 2000a; Koshurnikova et al. 1973). According to published data (Okladnikova et al. 2000b), in order to induce plutonium pneumosclerosis among Mayak PA workers, the absorbed alpha radiation dose to the lung had to be about 1.4 Gy or higher. However, this low value may relate to the workers also having been exposed to gamma rays, which has not been accounted for in this threshold estimate.
Current radiation protection standards and protective equipment at nuclear industry facilities in Russia limit inhalation of significant amounts of radionuclides and external gamma-ray exposure. Persistent respiratory system dysfunction was not detected in preliminary studies of Mayak PA workers who were exposed to external gamma-rays and internal alpha radiation over years in amounts not exceeding the maximum permissible annual dose (15 cSv) (Okladnikova et al. 2000c). Preliminary finding suggests a large cumulative radiation dose threshold for inducing persistent respiratory system dysfunction in the case of chronic exposure of the adult lung at low rates over years to alpha plus gamma radiations; however, more research is needed on this topic.
The present study was conducted with the following two goals: (1) to assess the functional state of the respiratory system (bronchopulmonary components) of a group of male Mayak PA workers who were chronically exposed at low rates over years to external gamma rays and internal alpha radiation (due to inhalation of plutonium aerosols), and (2) to develop an empirical threshold-type model for quantitatively characterizing respiratory system dysfunction (based on specific respiratory system variables) as a function of radiation doses (alpha and gamma) and smoking history. The model will facilitate estimation of thresholds for inducing the deterministic effect of interest (i.e., respiratory system dysfunction).
METHODS
Only previously documented dosimetry and clinical information were used in this study. Pulmonary function measurement protocols discussed here refer to work previously carried out by Russian physicians and scientists prior to initiating the clinical study during periodical prophylactic medical examinations of Mayak PA workers. The present study was approved by the Southern Ural Institutional Review Board. The SUBI assures that it complied with U.S. Department of Energy regulations for protection of human research subjects (10 CFR 745) and the Russian Federation Law of Public Health Protection (1993). In addition, the Western Institutional Review Board, Western International Review Board granted the project in which this study was undertaken an exempt status.
Specific respiratory system function measurements were used to assess the status of the bronchopulmonary system. The respiratory system function measurements were carried out during medical examinations of 386 male Mayak PA workers over a prolonged follow-up period (from 7 to 50 y for some subjects). The workers were exposed via inhalation to 239Pu aerosols and were also exposed to sources of external gamma radiation from neutron-activation and fission-product sources in the workplace. The indicated exposures occurred over several decades and the length of exposure varied for different individuals.
Individuals with bronchopulmonary diseases, plutonium pneumosclerosis, and other diseases which could influence respiratory function indices were not included in the present study. The respiratory function measurements were carried out 2–3 times with several year intervals for a majority of the individuals (65.7 %). In individual with a long-term follow-up period the number of respiratory function measurement was 10–12 times. The intervals between measurements were 5–10 years. Age at the time of respiratory function evaluation ranged from 19 to 81 years (average 44.2 ± 0.32 y). The time from starting work with sources of ionizing radiation until respiratory function evaluation ranged from 1 to 50 years (average 20.9 ± 0.31 y).
The following variables of the respiratory system function were analyzed: vital capacity (VC), carbon monoxide diffusing capacity (DCO), airway conductance including forced expiratory flow in one second (FEV1), and forced expiratory flow for 25%, 50%, or 75% of forced vital capacity (FEF25, FEF50, FEF75). Relative values were calculated as a ratio of the measured value and the predicted value, and were expressed as a percent (%) of the predicted value (Koo et al. 2000; Mustajbegovic et al. 2003). The predicted value was calculated as a function of age, height and body mass index (Knudson et al. 1987). We recognize that this may have introduce systematic error. This error is assumed to be small in comparison to the large variation in measured responses. Respiratory system function measurements were obtained using a compliance testing instrument (Godart, Holland) and a pneumatoscope II (Jaeger, Germany).
The main factors of occupational exposure were internal alpha radiation due to inhalation of airborne 239Pu compounds and chronic total-body exposure to external gamma rays; 46.2% of examined workers started working at the Mayak PA before 1958 when annual gamma-ray doses were the highest due to imperfection of technological processes. Later, the improvements in the radiation environment led to a reduction in the annual gamma-ray exposures of workers (Koshurnikova et al. 1999; Vasilenko et al. 2000).
External gamma radiation doses (D γ) to the total body were recorded by the dosimeter-control service of the Mayak PA, based on individual film badges. Dosimeter replacements and dose registrations were carried out once every month. After repair-maintenance work when the exposure risk was increased, dosimeter replacement and dose registration were carried out immediately. Before and during 1985, the dosimeter error was estimated to be about 60%. However, after 1985 this error was reduced to about 30%. The thermoluminescence method has been used since 1988 (Vasilenko et al. 2000).
The amount of incorporated 239Pu was estimated based on a urine bioassay carried out at the Biophysical Laboratory of the SUBI. The urine bioassay was based on the radiochemical method of double phosphate precipitation of 239Pu. The error in the estimated body burden of 239Pu was less than or equal to 30%. The detection limit for the 239Pu body burden was estimated to be 0.26 kBq (Russian Federal State Standard No. 37–2/93; Khokhryakov et al. 2000a, b). Absorbed alpha radiation doses (D α) to the lung were estimated based on the biokinetic model described by Khokhryakov et al. (2005). The model is a modification of the Human Respiratory Tract model (ICRP 1999). Total-body external gamma-ray doses and internal alpha radiation doses to the lung were calculated specifically for this respiratory function study.
Estimates of D γ ranged from 0 to 3.82 Gy (average 0.44 ±0.02 Gy). 239Pu body-burden estimates ranged from 0 to 91 kBq (average 2.65 ± 0.29 kBq), and D α estimates ranged from 0 to 4.35 Gy (average 0.16 ± 0.1 Gy). The reported standard deviations relate to variability in dose estimates for different workers and does not include dose uncertainty. Addressing dose uncertainty was beyond the scope of our research project. Thus, dose estimates provided should be considered preliminary. The average age at the start of work at the Mayak PA was 23.7 ± 0.3 years for these workers.
Smoking information was obtained with the help of individual interviews which were held by medical staff during obligatory medical preventive examinations. Smoking intensity was characterized using the smoking index (SI), which was calculated as the product of the number of packs of cigarettes smoked per day (d) and number of years (y) of smoking, and it was evaluated up to the time of respiratory function measurement. Units for the SI are therefore packs∗y/d. 82% of the examined Mayak workers were smokers, but 30% of these workers stopped smoking over the period that this study covers. Age at the start of smoking varied from 7 to 40 years (average 18.1 ± 0.3 y). On average, the duration of smoking was 26.5 ± 0.4 years at the time of follow-up. Some individuals smoked for more than 60 years. The average SI was 16.8 ± 0.4 packs∗y/d and the maximum value of this index reached 61.3 packs∗y/d. Morbidity information was based on medical documentation (case histories and medical cards).
Comparison of averages of study variables between smokers and non-smokers was based on Student's t test and Kolmogorov-Smirnov test (Zar 1999). Multiple regression analysis was used (Draper and Smith 1981; Korn and Korn 1968) for estimation of covariate dependences on the basis of our empirical non-linear model. Statistical significance was based on p <0.05.
RESULTS AND DISCUSSION
Based on the well-known fact that smoking has a negative effect on respiratory function, results are shown separately for smokers and non-smokers (Table 1). Workers with smoking durations of greater than 1 year were classified as smokers. The remaining workers were classified as non-smokers. These groups did not differ significantly in the average age at the time of respiratory function measurement, average time from the start of work in radiation exposure conditions until the time of follow-up, or in average total-body external gamma-ray dose. Indices of respiratory function both for smokers and non-smokers were within the physiological normal range as described by the American Thoracic Society (1991). However, a consistent decrease of not only airway conductance (FEF1, FEF25, FEF50, FEF75) but also VC and DCO were observed as the SI increased (Table 1). Table 1 provides comparisons between smokers and nonsmokers based on group-specific averages of respiratory function measurements as well the percentage of predicted values. The largest difference between groups (15–17.6 %) was seen for FEF50 and FEF25 which characterize the functional states of middle and small bronchi. Differences in VC and DCO values between smokers and non-smokers didn't exceed 3–4%. It was impossible to attribute unambiguously the decrease in indices of respiratory function to the effects of smoking because 239Pu body burdens and consequently D α values were significantly higher for smokers than for non-smokers (Table 1).
Respiratory function data for male Mayak PA workers
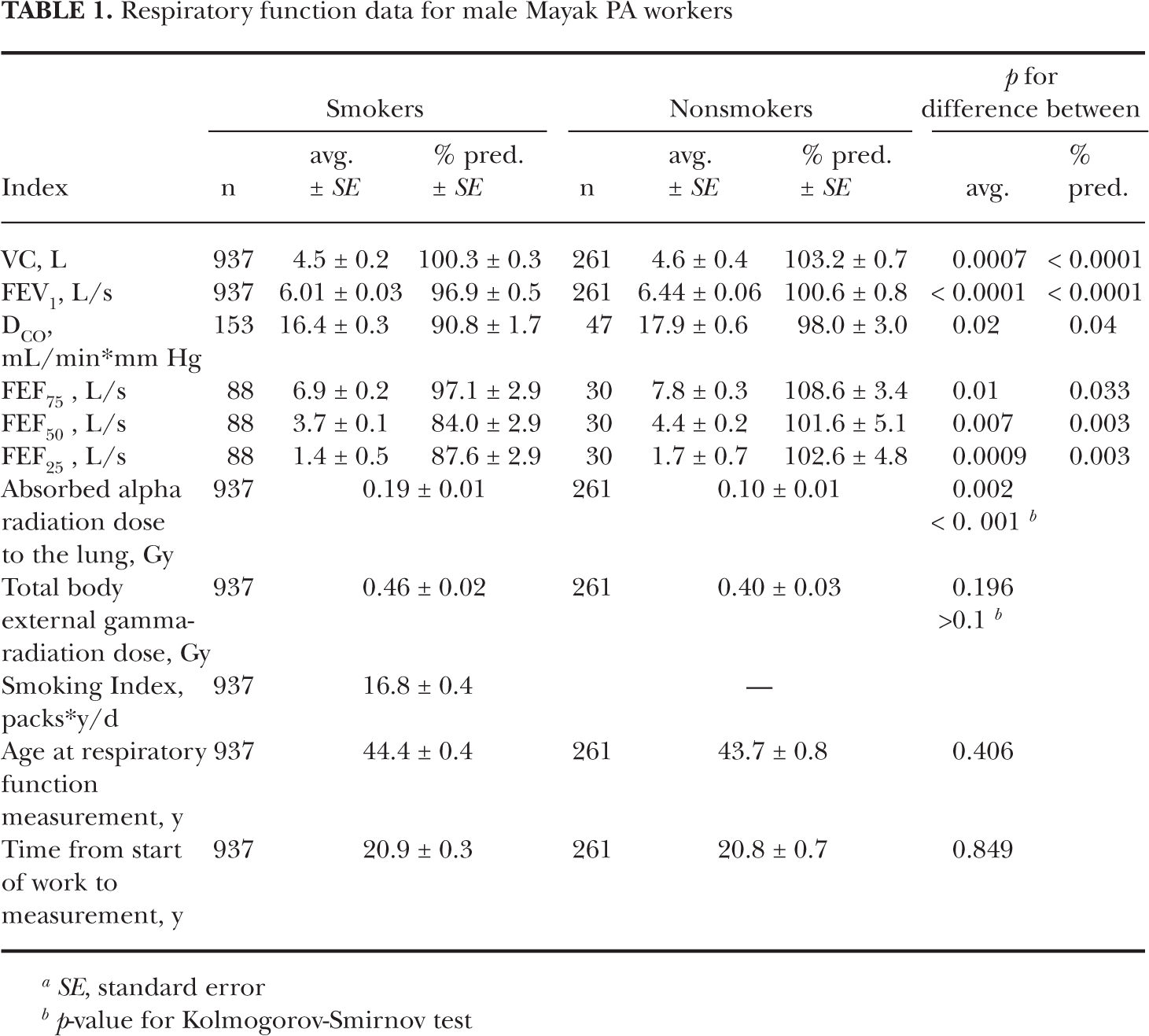
SE, standard error
p-value for Kolmogorov-Smirnov test
The following empirical threshold multifactor model was developed for the quantitative characterization of indices of respiratory functions under long-term exposure to alpha radiation from inhaled 239Pu aerosols and external gamma rays, taking into account the smoking history of nuclear workers at the Mayak PA:

Z represents the specific index of respiratory function (expressed in %). Z0 is the mean value of indices of respiratory function in the reference group (controls), which was formed out of unirradiated non-smokers. Only one control group was used. It was comprised of non-smoking, non-irradiated individuals. Unfortunately, this group was very small (Table 2), but their average age at the time of respiratory function measurement (41.9 ± 1.8 y) and the average time from start of work to measurement (19.2 ± 1.7 y) were not significantly different (p > 0.1) from corresponding averages for the irradiated nonsmoker group in Table 1. The value for Z0 was fixed prior to our regression analysis. Thus, results were conditional on Z0 . I and I0 are the smoking index and its threshold value (packs∗y/d). D 0,α is the threshold absorbed alpha radiation dose to the lung (Gy); D 0,γ is the threshold external gamma-ray absorbed dose to the total body (Gy); ψ is the slope parameter. ∊ is the error term and has a mean of zero and variance of σ2 (presumed independent of SI and radiation doses D α and D γ). The error term is needed to account for scatter in the real data. Based on our exploratory analysis of the data, D γ was found to be negligible for the range of doses considered here and therefore has been excluded from subsequent equations.
Results of model parameters calculation of respiratory function

SE, Standard error
Age has not been explicitly included as a covariate in our present model. Age-relate changes would be expected to have a similar influence on the numerator and denominator involved in assigning values to Z0 and Z so that the age influence would be expected to cancel. The duration of smoking and radiation exposure are accounted for via the exposure-time-dependent variables I, D α, and D γ. Systematic error in radiation doses (e.g., associated with dosimeter performance for gamma rays and bioassay for Pu incorporation) would be expected to cancel in application of Equation 1 since doses appear as ratios.
The following equation defines sub-threshold values when D γ is negligible:

Note that Equation 2 implicates an equivalence between smoking (I/I0 ) and alpha radiation (D α D 0,α) induced damage to the respiratory system so far as the occurrence of respiratory dysfunction and the normalized functions I/I0 and D/D0 . However, I0 and D 0,α should not be considered to cause the same level and type of damage to the lung. The overall empirical threshold model is represented by the following equation:

Geometric characteristics of the model (Equation 3) are shown in Figure 1. The following relationship was plotted (dashed contour line) to explain the meaning of ψ:
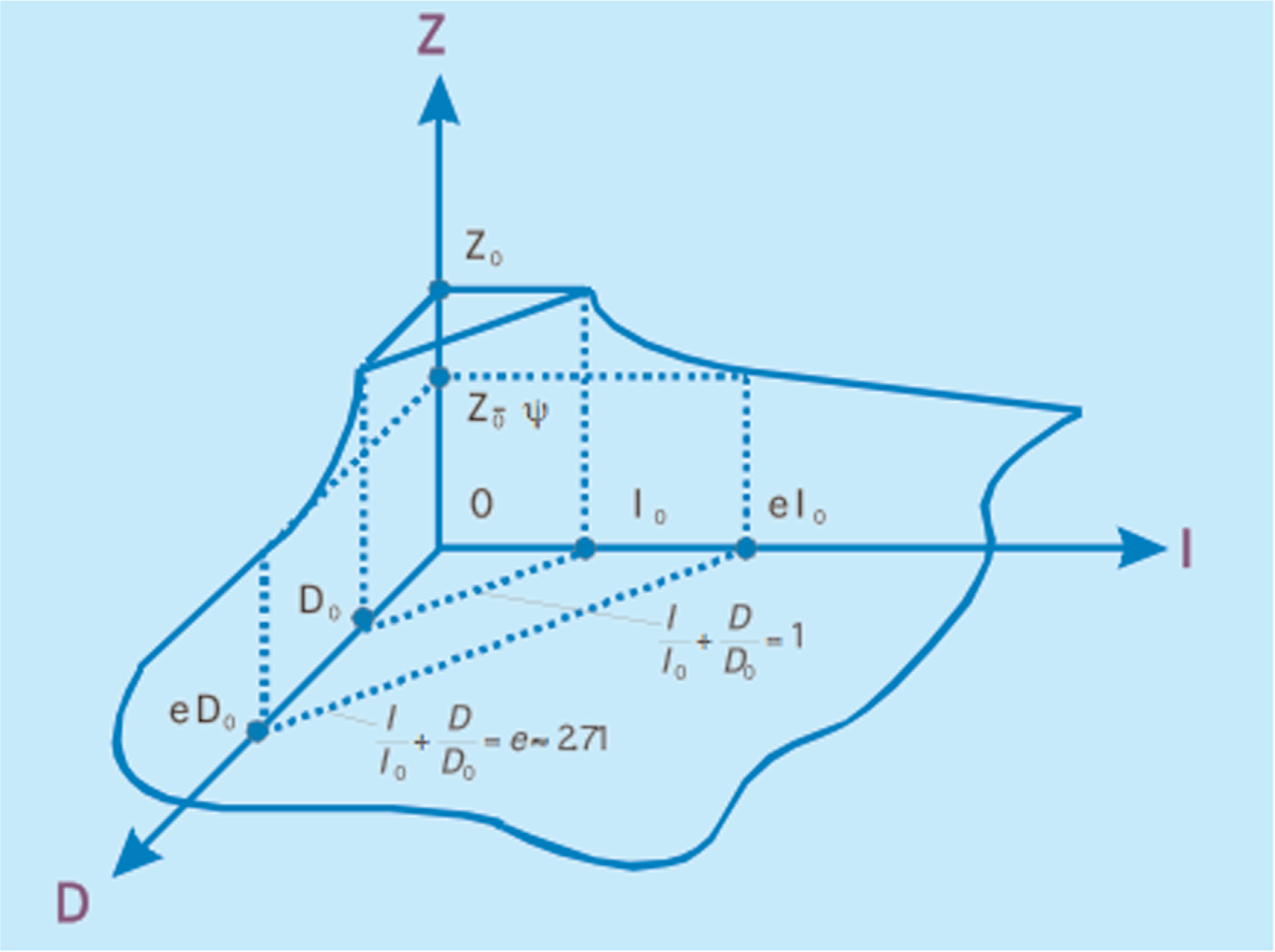
Geometric interpretation of the mathematical model represented by Equation 3. The response variable Z is presented schematically as a function of covariates D (radiation absorbed dose) and I (smoking index). Corresponding radiation- and smoking-associated thresholds are given by D0 and I0 , respectively. Z takes on the value Z0 – ψ, when (I/I0 ) + (D/D0 ) = e (i.e., the base for natural logarithms).
Results of model applications to respiratory function measurements for chronically irradiated Mayak workers are shown in Table 2. The Parameter ψ was subjectively changed while estimating I0 and D0 and therefore does not have an assigned standard error. The estimated thresholds I0 and D0 were statistically significant (p < 0.05). With our previous exploratory analysis with D γ included, we were not able to detect a dependency of the respiratory function indices studied on D γ. Also, no dependence of FEV1 on SI or D α was found.
Figure 2 presents the dependence of FEF50 on D α and SI. The indicated smooth response surface (sheet) is based on our model. Points falling above and below the model simulated surface are accounted for by the parameter ∊ when fitting the model to the data. Similar results were obtained for FEF25 and FEF75 surfaces.

Response-surface characterization of the forced expiratory flow for 50% of forced vital capacity (FEF50%) as a function of the smoking index and absorbed alpha-radiation dose to the lung for chronically irradiated Mayak PA workers. The smooth surface is based on Equation 3. The data are ratios of observed to the predicted values. The evaluation of predicted values is explained in the text.
Figure 3 presents the dependence of VC on D α and SI. The smooth response surface is based on our model. Points falling above and below the model simulated surface are accounted for by the parameter e. Similar results were obtained for the FVC surface.
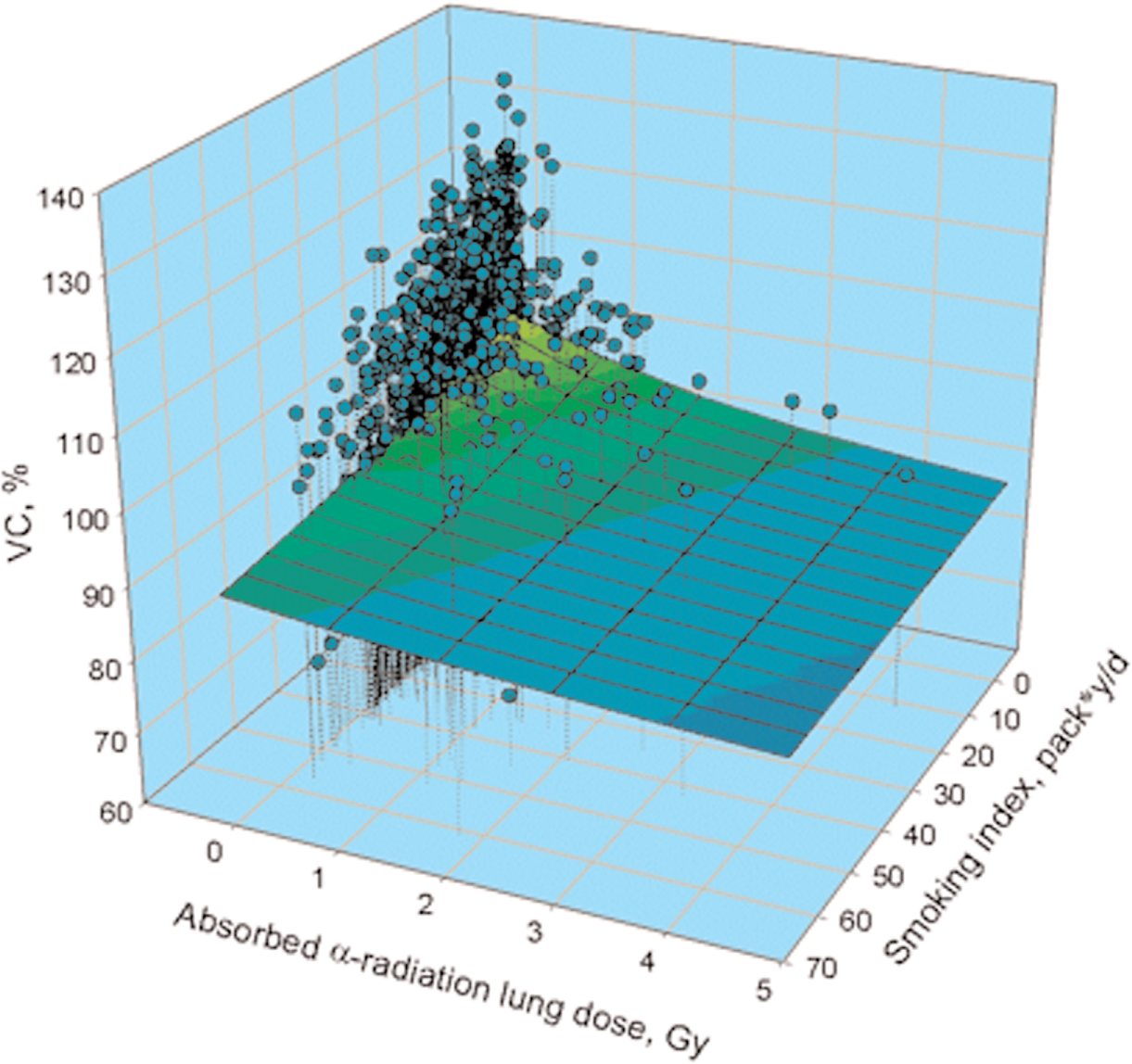
Response-surface characterization of the vital capacity (VC%) versus the smoking index and absorbed alpha-radiation dose to the lung for chronically irradiated Mayak workers. The smooth surface is based on Equation 3. The data are ratios of observed to the predicted values. The evaluation of predicted values is explained in the text.
The obtained data indicate significant decreases of airway conductance in smokers (based on FEV1, FEF25, FEF50, FEF75) and coincides with results of numerous studies which show a decrease in FEV1 under the influence of smoking (Sorlie et al. 1987; Xu et al. 1992; Sherrill et al. 1996). In our study we detected a decrease of FEF25 and FEF50, characteristic of reduced conductance of small and middle bronchi, which was more marked in comparison with other respiratory function indices. Similar results were obtained in a tobacco worker study (Mustajbegovic et al. 2003; Mukhtar et al. 1991). Tobacco smoke components have a direct damaging influence on bronchopulmonary tissue, initiate inflammatory processes accompanied with neutrophil and macrophage activation, affect the balance of proteolytic enzymes and antiprotease, and cause bronchial obstruction and oxidative stress leading to bronchi hypersensi-tivity (Willemse et al. 2004; Hunninghake and Crystal 1983; Pryor and Stone 1993; Zang et al. 1995; Wright et al. 1983). There are data showing development of diffuse interstitial pulmonary fibrosis in tobacco workers (Lorenzo 1988). Even short-term tobacco smoking causes an inflammatory response in bronchi mucous membranes (van der Vaart et al. 2005).
Application of the threshold multifactor regression model demonstrated a significant dependency between the respiratory function indices, SI and D α, in Mayak nuclear workers. The study did not reveal a correlation between chronic exposure at low rates to gamma rays and the state of respiratory function. This is in agreement with previous studies (Belyaeva and Okladnikova 2003). It is worth mentioning that the average radiation doses for the workers studied were relatively small (average D γ = 0.44 Gy, average D α = 0.16 Gy). The indicated average doses were much lower than radiation doses reported to cause serious deterministic effects in the lung (Ilyin IA 2005; Okladnikova et al. 2000a,b; Muggenburg et al. 1988; Miller et al. 2003).
Alpha radiation threshold estimates for inducing respiratory system dysfunction ranged from 0.15 to 0.39 Gy depending on the respiratory function indices used. For deterministic effects in the lung an alpha radiation RBE of 12 has been recommended relative to gamma-ray exposure (Scott and Peterson 2003). This would indicate corresponding gamma-ray thresholds in the range 12∗0.15 Gy-Equivalent (Eq) to 12∗0.39 Gy-Eq or 1.8 to 4.7 Gy-Eq. The unit Gy-Eq applies to threshold-type deterministic effects rather than Sv (which apply to linear-no-threshold type responses) (IAEA 2005). In our exploratory analyses, we found no influence of gamma-ray doses up to 3.8 Gy (average dose of 0.44 Gy) on the respiratory system indices studied. This suggests that a higher RBE than 12 may apply for alpha radiation induced respiratory system dysfunction. More research is needed on this subject.
Threshold estimates provided should be considered preliminary as they were obtained on the basis of analyzing a relatively small number of respiratory function measurements for the examined Mayak workers. Future studies are required for improvements and would require new research support.
The multifactor model was used to address the combined effects of smoking and radiation on respiratory system functioning. The same approach might apply for evaluating respiratory system functioning after exposure to other airborne toxicants including complex mixtures.
CONCLUSIONS
A new empirical mathematical model was introduced which allows quantitative characterizations of thresholds for smoking- and radiation-induced respiratory system dysfunction under circumstances of combined exposure. The model incorporates absolute thresholds for smoking- and radiation-induced dysfunction.
The new model allows equating cigarette induced impairment with radiation induced impairment. Equal ratios I/I0 and D α/D 0,α reflect expected equal levels of respiratory system impairment for smoking and radiation. Similar relations could possibly be established for other pairs of respiratory system irritants using the same modeling approach.
Respiratory function indices studied decreased as the alpha radiation dose to the lung increased from 0 to 4.36 Gy, while remaining in the normal range. The data were consistent with the view that alpha radiation doses to the lung above a relatively small threshold (0.15 to 0.39 Gy) cause respiratory system dysfunction.
Respiratory function indices were not found to be influenced by total-body gamma radiation doses in the range 0–3.8 Gy when delivered at low rates over years.
Significant decreases in airway conductance were shown in smokers when compared to non-smokers.
Footnotes
ACKNOWLEDGMENTS
The authors would like to express their gratitude to O. Lifanova for translations and J. Di Palma for editorial assistance. This work was supported by the Office of Science (BER), U.S. Department of Energy, Grant Numbers DE-FG02-03ER63657 and DE-FGF02-03ER63671. Additional support for B. R. Scott was also provided by Lovelace Respiratory Research Institute.