
Abstract
Prior to observing low-dose-induced cell signaling and adaptive protection, radiogenic stochastic effects were assumed to be linearly related to absorbed dose. Now, abundant data prove the occurrence of radiogenic adaptive protection specifically at doses below ∼ 200 mGy (with some data suggesting such protection at a dose even higher than 200 mGy). Moreover, cells do not thrive properly when deprived of radiation below background dose.
Two threshold doses need be considered in constructing a valid dose-response relationship. With doses beginning to rise from zero, cells increasingly escape radiation deprivation. The dose at which radiation-deprived cells begin to function homeostatically provides dose
Thresholds A and B should be terms in modeling dose-response functions. Regarding whole-body responses, current data suggest for low-LET acute, non-chronic, irradiation a
Introduction
There is much controversy regarding the relationship between dose and late radiation effects such as cancer. 1 A consensus approach accepts the linear-no-threshold (LNT) model to be applicable for any dose, however small, for the purpose of radioprotection –with linearity being assumed irrespective of radiation quality or type of biological target. The LNT function is schematically expressed in Figure 1 by the straight line. The unit of dose in the Figure is the Gray (Gy). The unit Sievert (Sv) complies with international recommendations for the purpose of quantitative comparison of health (cancer) risk. Zero dose in Figure 1 denotes the level of local background radiation in terms of cumulative dose (i.e. the dose conforms to absorbed dose exclusive of natural background radiation).
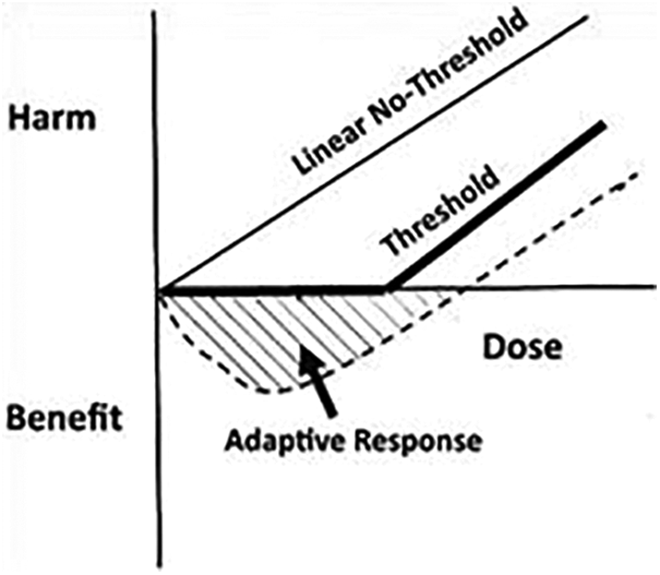
Traditional illustration of low dose radiation response.
Figure 1 shows 2 more debated curves: a) a threshold of dose below which radiogenic detrimental health effects are not seen experimentally or epidemiologically, and b) a J-shaped curve that express effects of adaptive protection against radiogenic and non-radiogenic spontaneous DNA damage in low-dose irradiated organisms.
At chronic exposures, doses may lead to some accumulated effects. However, the effects per Sv at low-dose-rates are considerably smaller or even absent compared with the effects per unit dose that are delivered acutely. The lower the dose-rate, the greater tends to be the efficacy of repair and protection against radiogenic damage. 2 In life-span studies in irradiated dogs, a threshold to life-shortening was observed after about 3 mGy per day in the case of chronic Co-60 gamma irradiation. 3 This dose amounts to about 1 Gy per year. The optimal dose-rate for extended life-span peaked at about 50 mGy/y or 0.14 mGy/d. 4
A tissue absorbed dose of 3 mGy per day from Co-60 gamma radiation causes stochastically distributed, on average, 10 radiogenic energy deposition events (hits) per nano-gram tissue, i.e. average cell, per day. Each of these hits, on average, is from about a 2 keV Compton electron track. 2 In other words, 3 mGy from Co-60 gamma radiation produces—on average—about 10 hits of about 0.3 mGy each per cell per day, or 1 hit per cell every 2.5 hours. The time between 2 consecutive hits affects the efficacy of repair and protection processes. 2
However, to more accurately depict the authentic relationship between dose and dose effects after low-dose and dose-rate irradiation, it is suggested that neglecting doses close to zero, i.e. below background radiation, may be misleading.
The Double Threshold
For reasons that have yet to be fully explained, living organisms do not thrive when deprived of absorbed doses well below normal background radiation, down toward zero dose. 5 For instance, subjecting living cells to ultra-low-dose radiation by encasing the species in heavily leaded shielding, or by placing them into deep caves, led to protecting them against a large fraction of the natural background radiation, i.e. to below a dose of 1 mGy per year. The ensuing biologic responses provided convincing data demonstrating that life in such a “radiation-protected” biosphere cannot physiologically thrive without at least some radiation. A minimum amount of radiation exposure appears to be essential for living organisms to develop and function. 6 -10
Hence, if one were to plot radiation dose from acute and protracted exposure vs dose response, where we reduce the radiation dose to begin at absolute zero, i.e. with no dose from ambient natural background radiation, one then arrives at a curve like the one in Figure 2, where there are 2 thresholds. Here the dose conforms to total absorbed dose including that from ambient natural background radiation. Moving from the harmful effect of zero radiation dose to a higher dose, we note that beyond Point A (the “Beneficial Threshold”), life functions at homeostasis properly. 2 With increasing doses, cells and tissues show changes in biologic signaling that culminate in adaptive protections in the exposed body. 2 These generally are referred to as “Protective Responses,” an expression of system of adaptation. 11 They tend to result in bodily benefit of various types—under genetic control, which also reflect individual differences to radiation sensitivity. Adaptive protection appears measurable down to about 10 mGy above background radiation doses. 11 Radiogenic protection also operates against non-radiogenic damage that quantitatively far outweighs radiogenic damage. Substantial research (e.g. reference 11) indicates that at higher radiation doses beyond the value indicated by point B in Figure 2, here called “Threshold for Harm,” harm prevails.

The double threshold.
With further increasing dose or dose-rate, damage eventually overwhelms the system. The junction between protecting and damaging responses to acute exposures peaks at about 100 to 200 mGy. 11 With protracted chronic exposures, the transition to harm occurs at a much higher dose, i.e. at about 1000 mGy or more.
In the dose region between A and B, prevention of damage (mainly of spontaneous origin) outbalances the degree of damage that might result from irradiation. If both damage causation and damage prevention are about of the same quantity, a threshold dose to harm would be the measurable system response. If damage causation by irradiation would be surpassed by prevention of damage, the result would be a measured benefit to the system, i.e. a hormetic response. 1,2
Zero Dose and Background Radiation
The question arises, how do the traditional curves relate to each other if the zero dose in Figure 1 expresses the dose without background radiation. In other words, do the curves in Figure 1 superimpose to those in Figure 2? The answer, obviously, is no.
Here it is suggested to insert a vertical line (called Z in Figure 3) to define the value of ambient background dose or dose rate level at which the exposed system operates homeostatically in the locale of interest. The regional background doses vary locally and add to the doses from other exposure modes. Even in the face of many uncertainties regarding the proper background radiation dosimetry, the annual background radiation exposure approximates 6 mSv/y for the United States (∼3 mSv/y for natural background plus an additional 3 mSv/y from medical and other radiation sources). If we are interested in Finland, we might start at ∼8 mSv/y associated with the prevailing background in that country. We might be tempted to put the vertical line Z at 120 mSv/y if we start evaluations in the Ramsar region of Iran, where the background is as high as 240 mSv / year. 12 At regions with higher background radiation levels, clinical studies show evidence of adaptive protection in people living in such regions. 2,11 This scenario would not be revealed by beginning observations of effects at the dose level of natural background radiation. Please note that this approach of summing up doses is not to sum up effects from these doses, but rather to generate evidence to what degree various background exposures modify the effects measured without relation to background doses, for instance, with respect of generating adaptive protection.

Where do we start.
Dose Levels of Adaptive Responses/Protections
Whereas the implications from the results of references
6
through
10
will surely lead to additional research to establish the “
There is, to state again, still both scientific and politically based controversy regarding the types and ranges of adaptive response/protection, despite evidence from experimental work and epidemiological observations. The cell responses operate under genetic control and, thus, vary individually. The
Radiation at higher acute exposure levels is clearly harmful, and current international standards are widely accepted as being appropriate for modeling acute radiation dose vs harm in the high dose range. It is in the low dose range in which humans generally reside under normal conditions where the controversy exists.
Threshold B and the LNT Dilemma
The most essential threshold to establish appears to be the one that describes the entire biological system, i.e. whole-body. Indeed, cell biology as well as epidemiology data conform to the existence of
One could argue that once the background radiation dose level is made to move from zero to a level where life begins to thrive (that is, point A) the threshold curves from Figure 1 and 2 could be superimposed. Whereas the Adaptive Curve of Figure 1 would nicely fit, this is not so for the straight line representing the LNT function. In other words, the curves confirm the lack of compatibility of the adaptive curve and the linear function. Indeed, the LNT model principally disagrees with the experimental evidence of both
Threshold B Doses for Defined Damages
Regarding
Because of the enormous harm being caused by unjustified public fear of radiation at any level, 14,15 it is suggested that the initial focus be directed to establishing a threshold dose for evacuation in the event of a nuclear accident or a dirty bomb. The dose-rate threshold for evacuation could be ∼300 mGy/year. If an accepted threshold dose had been established and applied for evacuations prior to the Chernobyl or Fukushima accidents, a great many lives would have been saved—to say nothing of the extreme discomfort suffered by those subjected to prolonged evacuations. 16
The next R&D target might be to establish a damage threshold dose for siting a high-level nuclear repository waste site. That limit could be 100 mGy/year, which is less than half the upper level of threshold of reduced life span in experimental settings with chronically exposed dogs. 17 The current regulations are so restrictive (requiring postulated accidental radioactive release to be many levels below natural radiation) 15 that it has added hundreds of millions of dollars to the repository designs—making any of them essentially impossible to license. This is a political problem, not one of science, and should be understood in public.
Practicality of a Threshold Model for Regulation
But even if appropriate thresholds could be established and accepted by the national and international radiation protection institutions and by the scientific community, there remains a question on how such threshold models could be used for regulatory purposes. Based on the discourse above, the key question in this context is to what degree a radiation dose, administered at a low rate (the kind of radiation atmosphere in which people live in every day), causes damage that accumulates in the body system. A considerable amount of research has demonstrated that cellular protection and repair systems are physiologically most efficient leaving, if at all, a very small fraction of radiogenic damage becoming available for accumulation. This fraction, indeed if it occurs, is so small that one cannot observe it separately from the rather abundant damage, such as of DNA, from non-radiogenic sources– and biomarkers for these damages are not available. In other words, radiogenic damage accumulation is buried to total invisibility in the bulk of non-radiogenic damage. Thus, a threshold model should be very easy to administer. There would be no need to record radiation dose from normal background exposure—or industrial radiation exposure where the dose was received at low dose rates. The lowest threshold level observed with statistical significance in a system could serve as cut-off value for protection purposes. This issue is controversially entangled in the midst of political goals.
Next Steps
Considering what we know already and assuming the legitimacy of the above generic arguments, we suggest initiating a long-term, well-funded low dose program and coordinated at a global level. But rather than just turning researches on to an infinite list of “interesting” trails, we urge a key goal of the program to be that of evolving a new radiation standard based on a threshold model that regulators can use. Moreover, this research is expected to amplify and corroborate the potential for low-dose radiation in clinical trials on low-dose radiation therapy, for instance, for pneumonia, neurodegenerative diseases, auto-immune diseases, metastatic cancer, and infections.
To simply continue focusing on the limits of LNT model will not solve our problem. Regulators should aim at a sensible threshold model
18
that can be easily administered. It would appear most prudent to recognize this as both a necessary and achievable goal. For the time being, the current state of knowledge suggests a
Footnotes
Authors’ Note
The views and opinions expressed here are those of the authors and do not necessarily reflect the official policies or position of any affiliations that the author may have. Alan Waltar is now a Retired Professor and Head, Department of Nuclear Engineering, Texas A&M University, College Station, TX.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.