
Abstract
Objective
The purpose of this study was to determine the effect of 12°C cold exposure for 180-minutes on the hormonal responses of sleep-deprived individuals.
Methods
Participants underwent 2 cold-air trials: 1 after a normal night of sleep (ie, 6–8 hours) and 1 after 33 hours of sleep deprivation (SDEP). A venous blood sample was taken at baseline and then at 90-and 180-minute cold-exposure time points. Repeated-measures analysis of variance was used to determine significance between a normal night of sleep and SDEP for norepinephrine, epinephrine, cortisol, insulin, thyroid hormones triiodothyronine and thyroxine, glucose, and non-esterified fatty acids.
Results
There was no significant main effect for time, trial, or interaction for insulin, thyroid hormones, epinephrine, cortisol, and glucose (P ≤ .05). A significant main effect for time for norepinephrine and non-esterified fatty acids was demonstrated (P < .001).
Discussion
The lack of significant differences in the hormonal and metabolic responses to cold exposure combined with SDEP may have been because of an ability of the individual to continue to respond despite the environmental stressor or the physiological effect elicited from cold exposure, thereby possibly masking physiological responses of SDEP.
Conclusions
On the basis of these data, SDEP combined with protracted cold exposure apparently was not a great enough stressor to cause a differential response in the hormonal and metabolic parameters.
Introduction
Sleep deprivation (SDEP) and cold exposure are 2 physiological stressors that may have an affect on the body's ability to thermoregulate. The popularity of sports such as mountain climbing and the rigors of military operations combine these physiological stressors. Pugh 1 examined 23 cases of hypothermia in winter recreation activities to discern similarities among them and determined that the majority of the victims were fatigued, of which many were sleep deprived. Hypothermia cases have occurred during military training operations that combined numerous physiological stressors (eg, SDEP, cold exposure, exercise, negative caloric balance). 2 To help reduce these hypothermic injuries, it is important to discern which stressors may have an impact on increasing the prevalence of hypothermia. Furthermore, the combination of SDEP and cold exposure may have a distinct influence on thermoregulation when compared with their individual responses. Therefore, it is important to investigate the physiological effects of these combined stressors.
Sleep deprivation is defined as fewer than 6 to 7 hours of sleep, which is the average amount an adult needs to maintain normal physiological functioning. 3 Sleep deprivation has been hypothesized to alter central nervous system activity, thereby down regulating a number of physiological processes (eg, reduced body temperature, muscle coordination, cognitive function). 4 It has also been shown to disrupt normal metabolism5,6 and alter endocrine function. 7 If SDEP alters resting core temperature and disrupts both hormonal and metabolic processes, thermoregulation may be altered.
Thermoregulation during cold exposure is regulated through both central and peripheral mechanisms. Body temperature is regulated through a complex nervous system feedback mechanism where the hypothalamus is the control center for temperature regulation. 1 Therefore, as the body tries to maintain core temperature during cold exposure, central thermoregulatory mechanisms are altered.
Both cold exposure and SDEP act as physiological stressors that alter the hypothalamic-pituitary-adrenal (HPA) axis, which is the site of central thermoregulation. 8 By altering the HPA axis, numerous hormonal pathways may be altered, thereby possibly shifting mechanisms that the body uses to respond to these stressors (ie, up- or down-regulating hormones that affect thermoregulation and fuel utilization). 9 Changes in hormonal status and thereby fuel utilization may alter the body's ability to thermoregulate; therefore, it is important to consider the effects of the combination of SDEP and cold exposure on hormones important to thermoregulation.
Alterations in endocrine and hormonal function have been shown to occur after SDEP, but findings have been equivocal. Plasma cortisol (CORT) concentrations as well as sympathetic nervous system activity are increased after SDEP. 7 Alternatively, Vogntzas et al 10 noted an increase in activity of the HPA axis with 24 hours of SDEP. Unlike Spiegel et al, 7 Vogntzas et al 10 noted reductions in CORT secretions after SDEP. Decreases in CORT concentrations reduce blood glucose (GLU) concentrations, which would ultimately affect GLU metabolism. Kuhn et al 11 noted increases in CORT and decreases in plasma GLU but also noted increases in free fatty acids. Because of previous inconsistent research findings, it is important to reevaluate the impact SDEP has on hormonal and endocrine function.
Thyrotropic function and the activity of the HPA axis may also be reduced by SDEP. 11 This finding is especially important with respect to cold exposure because the hypothalamus is the center of thermoregulation. Palmblad et al 12 demonstrated an increase in thyroid hormone concentrations, which were believed to be due to an increase in thyroid stimulating hormone (TSH). After their study subjects experienced 24 hours of SDEP, Parekh et al 13 and Gary et al 14 demonstrated increases in TSH, which were believed to be related to changes in the HPA axis. Others demonstrated no changes in triiodothyronine (T3) and thyroxine (T4) and a decrease in TSH. 5 The variations in findings may be attributed to activity level or cognitive-performance activities that the participant underwent during SDEP. 14
Research has also shown that fuel utilization during SDEP may be altered because of changes in hormonal concentrations. Carbohydrate tolerance may be impaired. 7 A reduction in GLU tolerance in humans has been noted after 60 hours of SDEP. 15 A decrease in the acute insulin (INS) response to high plasma GLU concentrations has been noted during prolonged discontinuous SDEP. 7 In addition, researchers have shown decreases in INS sensitivity during acute cold exposure.5,15 Therefore, because components of carbohydrate metabolism are altered during both cold exposure and SDEP, there may be a reduction in carbohydrate metabolism when these stressors are combined. However, this is difficult to discern from current literature because of the various lengths and types of both SDEP and cold exposure used in previous research as well as the lack of research combining these 2 stressors.
Sleep deprivation alters both resting hormonal and metabolic responses; therefore, these changes during rest may be amplified or attenuated when SDEP is combined with cold exposure, but few studies have addressed this theory. The purpose of this study was to determine if 180 minutes of cold exposure at 12°C had an effect on the hormonal and metabolic concentrations of sleep-deprived individuals. Researchers have hypothesized that sympathetic nervous system activity is increased after SDEP and that the HPA axis may be altered. Changes in both pathways may directly affect the body's ability to thermoregulate.
Methods
Before data collection, the Kent State University Human Subjects Review Board approved all experimental protocols. Each participant provided written informed consent before participating. The study consisted of 6 women and 6 men who were all regularly active, apparently healthy, and nonsmokers between the ages of 18 and 40 years and who averaged 6 to 8 hours of sleep per night and were free of all supplements and medications. Also, women were not using oral contraceptives and were eumenorrheic, and they were tested only during the follicular phase of their menstrual cycle (days 1–7 of the menstrual cycle), whereby day 1 of the follicular phase was defined as the first day of menses. Experimental trials were completed during this phase of the menstrual cycle to control for possible changes in core temperature related to menstrual cycle phase, for previous studies have shown that core temperature during the luteal phase may be higher than in the follicular phase. 16
Preliminary measures of height (in centimeters) and weight (in kilograms) were measured with a stadiometer and balance beam scale. Body density was determined with skinfolds (chest, midaxillary, triceps, subscapular, abdomen, suprailliac, and thigh). 17 Percent body fat was calculated from body density by using the Siri equation. 18 Surface area (in square meters) was calculated from height and weight. 19 Anthropometric measures were measured for the purpose of determining participant characteristics.
A maximal exercise test was performed on a magnetically braked cycle ergometer (Lode Excalibur, Groningen, Netherlands) to determine oxygen uptake peak for participant characteristic purposes only. The protocol consisted of increasing the workload progressively until maximal voluntary exhaustion was achieved. Expired respiratory air samples were collected continuously via collection of expired gases throughout the exercise test and recorded at 30-second intervals (MAX-1 CART, Physio-Dyne Instrument Company, Quogue, NY).
Participants were exposed to 2 cold-air trials (CAT) at 12°C for 180 minutes. The temperature of the trials was chosen to mimic previous cold-exposure literature that demonstrated physiological changes.20,21,22 Ambient temperature of the environmental chamber was maintained at 12 ± 0.5°C in a climate-controlled environmental chamber (Neslab, Newington, NH). Relative humidity was passively controlled. The average humidity in the experimental lab was 48%.
Each participant completed a control (CON) and an SDEP experimental trial of same temperature and duration. The SDEP trial began after the participant had been awake continuously for 33 hours after a night of at least 6 to 8 hours of continuous sleep. Thirty-three hours of SDEP was selected to replicate the average of SDEP ranges used in previous studies6,15,23 and to control for circadian rhythms. One of the researchers in the laboratory continuously monitored SDEP. The order of the trials was counterbalanced. In a meeting with participants before the experimental trials, each participant was asked his or her normal morning time to wake up and normal length of sleep during the night. Both experimental trials were then scheduled at the same time of day (ie, between 3:00
Participants refrained from consuming alcohol or caffeine and abstained from exercise for 24 hours before the CAT. Participants were also 12 hours postprandial. Trials were separated by at least 48 hours, for this period of time has been shown to be a sufficient recovery interval between SDEP trials. 8 Thermoregulatory and metabolic (oxygen uptake) variables were collected continuously throughout the trials, and findings have been previously published. 24
After the 33 hours of SDEP, the participants underwent a CAT whereby each one rested for a 30-minute baseline (BASE) period in a thermoneutral air environment outside the environmental chamber, during which time BASE blood measures were collected. The following blood parameters were measured at each blood-collection time point: catecholamine norepinephrine (NE), epinephrine (EPI), CORT, INS, thyroid hormones T3 and T4, GLU, and non-esterified fatty acids (NEFA). During the 30-minute BASE, participants sat quietly in a semirecumbent position on a lounge chair in 26 to 28°C air. They were then wheeled on lawn chairs into the environmental chamber to commence the experimental trial. The participants wore shorts (men) or shorts and a jogging bra (women) and remained seated and still on plastic lawn chairs with their arms and legs separated and extended. The participants were also permitted to wear socks during the CAT. Venous blood was drawn from the antecubital space with a vacutainer at the 90- and 180-minute time points of the CAT.
Standard laboratory procedures in accordance with the Kent State University Review Board were followed regarding the venipuncture protocol. Fourteen milliliters of blood was taken at each time point. Before blood was centrifuged, 0.5 mL was extracted from the whole blood for catecholamine stabilization. Blood was centrifuged for 10 minutes at 300g at 12°C (IEC Centra-7R, International Equipment Company, Needham Heights, MA). Serum and plasma was then removed from the tubes and frozen at −70°C for later analyses.
Catecholamine concentration was determined at Walter Reed Army Institute, Washington, DC, by alumina extraction with a chromsystems reagent kit for high-pressure liquid chromatography analysis of catecholamines in plasma. The between-days coefficient of variation is less than 3% and the within-days variation is less than 1%. The coefficient of correlation from 9 to 1000 pg is 0.9989 and sensitivity is 5 pg with a signal-to-noise ratio of 5:1.
For the determination of GLU concentration in duplicate, the glucose trinder enzymatic method was used (Kit no. 315–100, Sigma Diagnostics Inc, St Louis, MO). Glucose concentration was calculated based on the absorbance of the standard (300 mg·dL−1), the sample, and a blank (deionized water). Plasma NEFA concentration in duplicate was determined by an in vitro enzymatic colorimetric method (Kit no. 994–75409, Wako Chemicals USA Inc, Richmond, VA). Insulin was determined in duplicate by enzyme-linked immunosorbant assay (Kit no. 008-10-1113-01, Alpco diagnostics, Windham, NH). Cortisol concentration was determined in duplicate by radioimmunoassay technique (Kit no. 06B256635, Corti-Cote, ICN Pharmaceurticals, Diagnostics Division, Orangeburg, NY). Total T4 and T3 concentrations were determined in duplicate by using 125I radioimmunoassay in plasma (Kit no. TKT41, DPC Coat-A-Count, Los Angeles, CA). Total T4 and T3 concentrations were then determined by a standard curve, as were concentrations of all assays.
Statistical Analysis
A 2 × 3 repeated-measures analysis of variance was used to determine differences between the SDEP and CON trials by using SPSS software (SPSS 11.5.0, SPSS Inc, Chicago, IL). Because of the small number of participants and the previous analysis of data, the male and female data were pooled (n = 12). From the previous analysis, no significant differences related to SDEP with respect to gender were found. Significance was set a priori at P ≤ .05. When significant differences were found, post hoc simple effects analysis was used to determine significant contrasts with Bonferroni adjustments. All values were expressed as mean ± SD.
Results
Participants
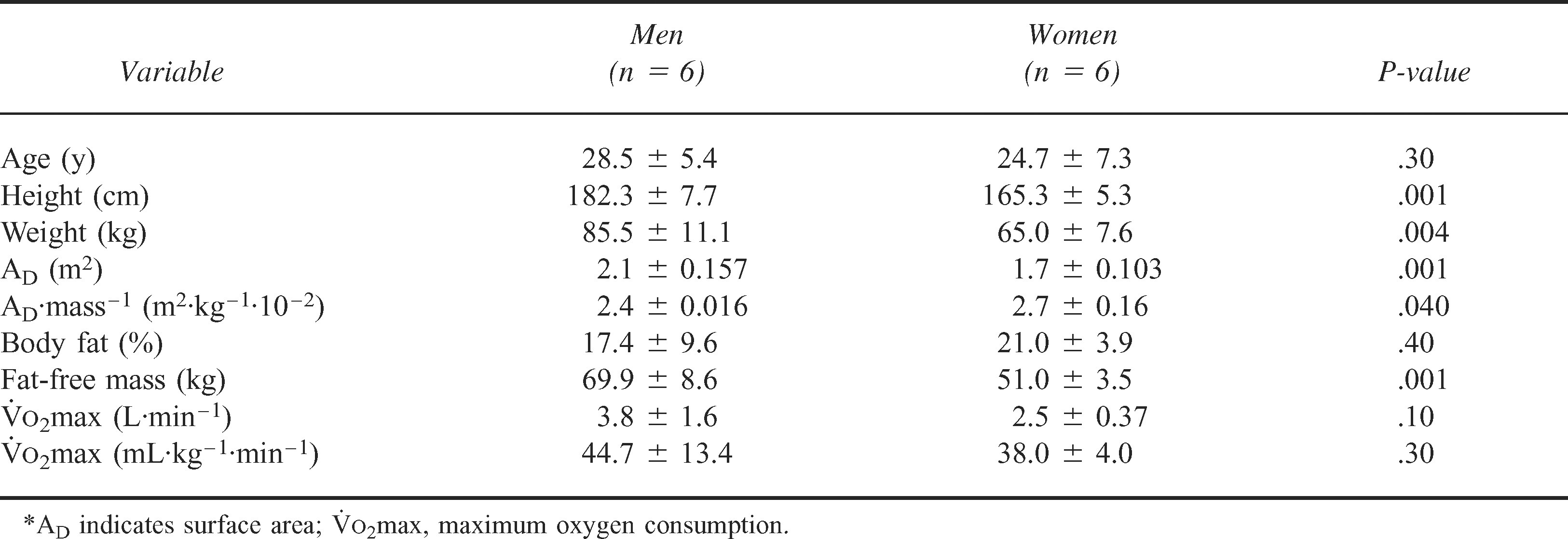
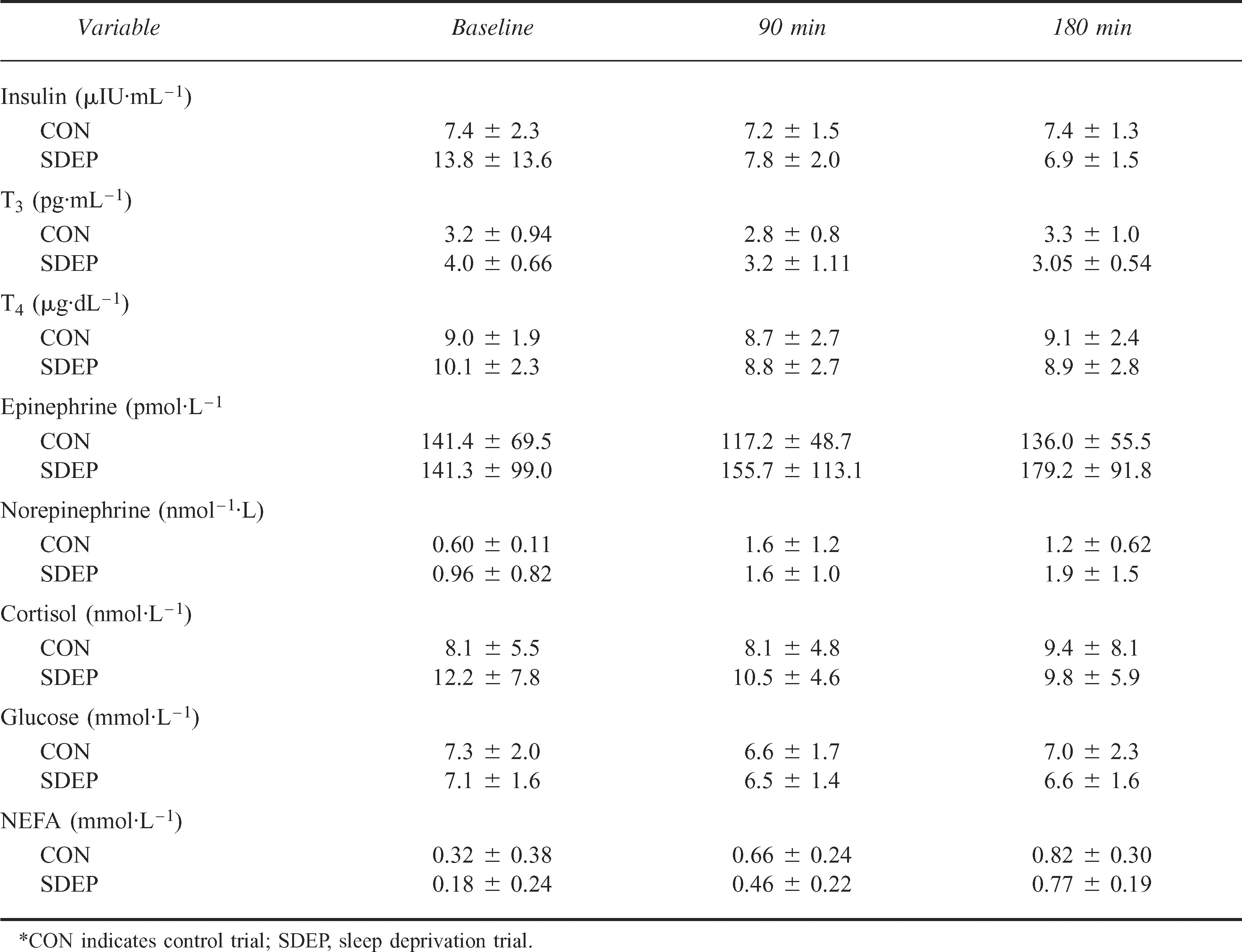
The current investigation measured apparently healthy male and female participants (n = 12) (Table 1). Group means for individual time points and treatments for each variable are provided in Table 2. Effect size (ES) (ie, eta squared) for main effects is reported for each variable.
Participant characteristics (mean ± SD)*
Group means for experimental variables (mean ± SD)*
Insulin
There was no difference in INS concentrations between SDEP and CON trials (9.5 ± 8.5 μIU·mL−1 and 8.3 ± μIU·mL−1 5.1; P = .24, ES = 0.15) or between time points (P = .12, ES = 0.21). No significant interaction was determined (P = .17).
Triiodothyonine
There was no difference in T3 concentrations between SDEP and CON trials (3.10 ± 0.91 pg·mL−1 and 3.41 ± 0.87 pg·mL−1; P = .17, ES = 0.28) or between time points during the CATs (P = .12, ES = 0.12). No significant interaction was determined (P = .13).
Thyroxine
There was no difference in T4 concentrations between SDEP and CON trials (9.28 ± 2.97 μg·dL−1 and 8.92 ± 2.23 μg·dL−1; P = .55, ES = 0.06) or between SDEP and CON over time during the CATs (P = .55, ES = 0.19). No significant interaction was determined (P = .20).
Epinephrine
There was no difference in EPI concentrations between SDEP and CON trials (158.75 ± 99.72 pmol·L−1 and 131.56 ± 57.65 pmol·L−1; P = .42, ES = 0.07) and no significant main effect for time (P = .45, ES = 0.09). No significant interaction was determined (P = .48).
Norepinephrine
There was no difference in NE concentrations between SDEP and CON trials (1.51 ± 1.20 nmol·L−1 and 1.13 ± 0.88 nmol·L−1; P = .27, ES = 0.12). On the other hand, there was a significant main effect for time (P = .002, ES = 0.75) (Figure 1). The 90- and 180-minute time points were different from BASE. No significant interaction was determined (P = .40).
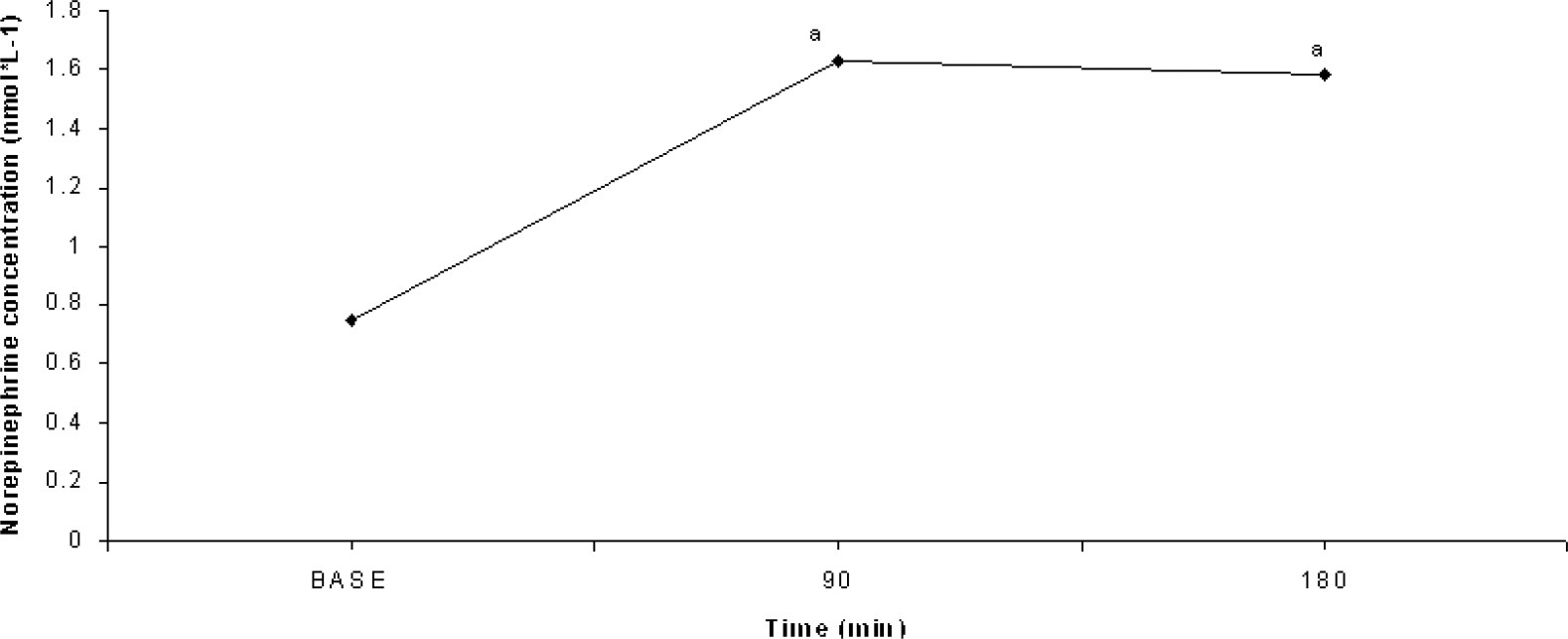
Main effect for time for norepinephrine concentrations (mean ± SD) (P = .011). “a” indicates significant difference from baseline.
Cortisol
There was no difference in CORT concentrations between SDEP and CON trials (10.81 ± 6.10 nmol·L−1 and 8.54 ± 6.10 nmol·L−1; P = .07, ES = 0.36) and no significant main effect for time (P = .84, ES = 0.02). No significant interaction was determined (P = .58).
Glucose
There was no difference in GLU concentrations between SDEP and CON trials (6.71 ± 1.52 mmol·L−1 and 7.00 ± 1.97 mmol·L−1; P = .59, ES = 0.03) and no main effect for time (P = .56, ES = 0.06). No significant interaction was determined (P = .46).
Non-Esterified fatty acids
There was no difference in NEFA concentrations between SDEP and CON trials (0.47 ± 0.32 mmol·L−1 and 0.60 ± 0.37 mmoL−1; P = .19, ES = 0.179). A significant main effect for time was demonstrated (P < .001, ES = 0.78) (Figure 2). Post hoc analysis revealed significant differences between all time points. Furthermore, no interaction was determined (P = .46).
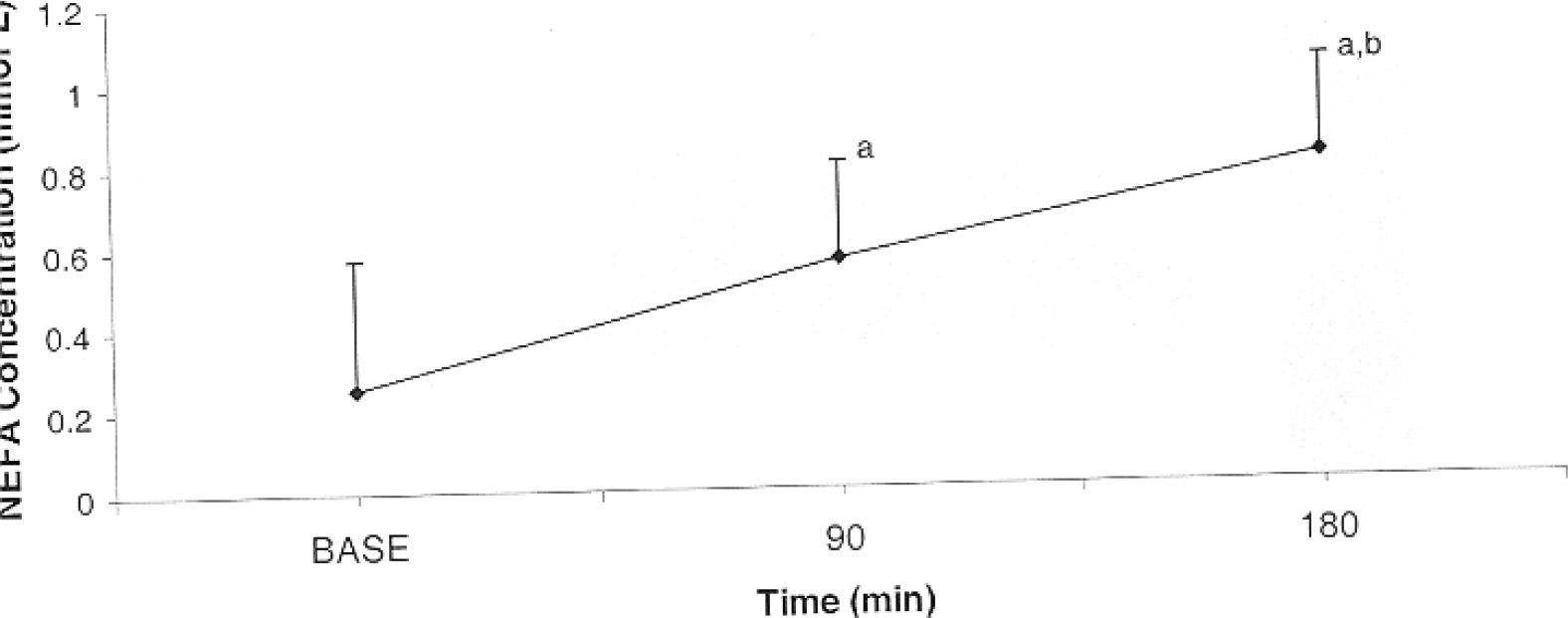
Main effect for time for non-esterified fatty acids concentration during cold exposure trials (mean ± SD) (P < .001). “a” indicates significant difference from baseline; “b,” significant difference from 90-minute time point; and BASE, baseline.
Discussion
The purpose of this study was to determine if 180 minutes of cold exposure at 12°C had an effect on the hormonal and metabolic concentrations of sleep-deprived individuals. Previous investigations have demonstrated hormonal changes during SDEP11,12 and cold exposure. 27 Therefore, the combination of these 2 stressors may alter hormonal response. Because both SDEP and cold exposure are physiological stressors that are partially regulated by the HPA axis, the combination of these stressors may attenuate hormonal response, thereby affecting available fuel (ie, GLU and NEFA) or altering thermoregulation. The hormonal and metabolic responses during the CON trial agree with previous research literature in the area of cold exposure at rest.4,22,27,28
Overall plasma NE concentrations were similar between SDEP and CON trials. Previous studies have shown that SDEP increases sympathetic nervous activity,7,11,29 but these studies have not considered the synergistic effect of SDEP and cold exposure. Therefore, it is difficult to discern the synergistic effect the combination of these 2 stressors may have. It may be that there is no additive effect in the increase NE when SDEP and cold exposure are combined; therefore, the cold exposure may have masked the physiological effect of SDEP. Fiorica et al 23 noted increases in NE in the combined SDEP and the CATs as well as the CATs alone but found no difference between the 2 trials. However, their study was in an uncontrolled environment.
Plasma NE concentration demonstrated approximately a 2-fold increase from BASE and the 90- and 180-minute time points of the CATs. Young et al 30 also demonstrated a 2-fold increase in plasma NE during 5°C cold exposure for 90 minutes. Leppaluoto et al 27 demonstrated increases in NE after 120 minutes of cold exposure.
There was no difference in plasma EPI concentrations between SDEP and CON trials. Previous research has shown increases in EPI production during SDEP.11,29 The findings of the current study may have been different if a greater amount of SDEP or different types of SDEP (ie, longer SDEP or discontinuous vs continuous SDEP) had been used.11,29 Furthermore, cold exposure may have exerted a greater physiological stressor than the SDEP, thereby masking the physiological effects of SDEP. No change in plasma EPI concentrations were recorded over time, which is in agreement with other research. 31 It should be noted that these findings measured changes only in EPI during cold exposure and not combined with SDEP.
There was no difference in the plasma CORT concentrations between SDEP and CON trials or over time. Because of CORT's integral role as a stress hormone, its response during the current study is important because of its role in regulating fuel and its peripheral effects on thermoregulation. Previous research has shown increases in plasma CORT concentrations 7 as well as reductions in CORT during SDEP. 10 Leppaluoto et al 27 and Wilson et al 25 found decreases in CORT during cold exposure, but the trials were shorter (ie, only 120 minutes) and colder (ie, 10 and 2°C, respectively). Therefore, the combination of the 2 stressors may have negated each other's individual responses. Furthermore, both the length and the temperature of the trial may have an effect on CORT concentration.
There was no difference between T3 and T4 concentrations between SDEP and CON trials or over time. Previous findings regarding SDEP are equivocal. Furthermore, the studies that have assessed changes in T3 and T4 status after SDEP have been only during resting SDEP and not combined with cold exposure. Hackney et al 32 found no change in T3 and T4 status, whereas others have found increases in these 2 thyroid hormones 12 or increases in TSH, which would alter T3 and T4 concentrations.13,14 Gary et al 14 attributed differences in the findings to differences in activity levels or cognitive performance that occurred during the SDEP period. The lack of change in T3 and T4 in the present study is in agreement with previous research.25,26 Therefore, the stressors may not have been extreme enough to cause a change in these variables. Furthermore, the SDEP may have caused a change in the circadian responses of these 2 hormones, thereby eliciting a lack of change during the SDEP trial. 33
There was no difference in INS concentrations between SDEP and CON trials. Little research measuring the combined effects of SDEP and cold exposure has measured INS. Decreases in INS response during acute high plasma GLU concentrations have been demonstrated during SDEP. 7 No change in GLU concentrations occurred over time; therefore, a change in INS sensitivity would not be expected. Furthermore, Gonzalez-Ortiz et al 5 found a decrease in INS sensitivity after 24 hours of SDEP. Clearly, more research needs to be completed in this area of study before researchers can begin to make more definitive conclusions.
There was no change in plasma GLU concentrations between SDEP and CON trials. Previous research in the area has shown increases in blood GLU during SDEP. 7 This is not surprising because there was no change in the fuel-regulating hormones’ (ie, CORT and catecholemines) concentrations in the current investigation. The variation in findings may be attributed to previous research in this area not combining SDEP with cold exposure. Therefore, the inclusion of cold exposure may have altered the effect. Furthermore, there was no change in plasma GLU concentrations at BASE and the 90- and 180-minute time points. This does not necessarily suggest that there was not an increased use of blood GLU, rather, only that blood GLU levels were maintained.
There was no difference in NEFA concentrations between SDEP and CON trials, but a significant 28% increase in NEFA was found from BASE to the 180-minute time point. Previous research combining SDEP and cold exposure has not previously measured SDEP; therefore, it is difficult to compare with the current body of literature. The increase in NEFA is important to fuel utilization during cold exposure because of the large availability of energy that is available from the breakdown of lipid, which allows for GLU sparing. 34 Previous research has also shown increases in NEFA during cold exposure.27,34 The increase in NE demonstrated over time is not surprising because the sympathetic nervous system is important in the regulation of adipose tissue mobilization of NEFA during cold exposure. 35
Conclusions
There was no difference in both hormonal and metabolic variables between SDEP and CON trials. The lack of significant differences in the hormonal and metabolic responses to the combination of cold exposure and SDEP may have been because of the ability of the individual to continue to respond physiologically despite the stressor. Furthermore, the lack of change in hormonal status may also have been because of the body's ability to respond peripherally to the combined stressors and not elicit central mechanisms of thermoregulation. It should also be noted that this study had low statistical power. Therefore, on the basis of these data, it appears that SDEP combined with protracted cold exposure is not a great enough stressor to cause a differentiated response in the thermal or metabolic parameters. Further research should examine the effects of SDEP on physiological responses during cold exposure of longer duration, the varying thermal stressors, and the different types of SDEP protocols (ie, continuous vs discontinuous).
Footnotes
Funding
The authors would like to thank the test volunteers for their participation and cooperation in this study and the Wilderness Medical Society for the financial grant support of this research endeavor.