
Abstract
Objective
To explore the effect of aspirin on the thermoregulatory responses of men during exposure to 12°C air (acute cold exposure) for a period of 120 minutes and recovery in 25°C air (rewarming) for 120 minutes.
Methods
Seven male subjects (26.1 ± 2.4 yr) underwent pre-experimental testing to determine peak VO2 and body composition. Participants underwent 3 trials in which they ingested the following for 1 week prior to each experimental trial: a capsule filled with cellulose (placebo), 81 mg · day−1 of aspirin (low-dose aspirin), or 650 mg · day−1 of aspirin (high-dose aspirin). Each trial consisted of a 30-minute baseline period, 120 minutes of exposure to 12°C air, and 120 minutes of recovery in 25°C air. Mean skin temperature and rectal temperature (Tre) were measured, and heat production was calculated.
Results
During both acute cold exposure and rewarming, analysis of variance revealed a main effect for time (P < .05) with respect to Tre, mean skin temperature, and heat production. However, there were no significant differences between the treatments or treatment by time interactions.
Conclusions
These data demonstrate that aspirin had no significant effect on the thermal and metabolic responses during acute cold exposure and rewarming.
Keywords
Introduction
Aspirin is the most commonly used over-the-counter drug, attributed to its having both central and peripheral nervous system effects. It blocks prostaglandin synthesis by nonselective inhibition of cyclooxygenase. 1 As such, aspirin has antipyretic, analgesic, anticoagulant, and anti-inflammatory properties. 2 With regard to temperature homeostasis, aspirin lowers fever by inhibiting prostaglandin synthesis in the hypothalamus. 3 It would follow that aspirin might lower body temperature in nonfebrile individuals, but animal4,5 and human6,7 literature has not shown consistent results.
In wilderness medicine, the prevention of hypothermia is of utmost concern. Prior work in our lab 8 and others 9 has shown a strong link between cardiovascular function and thermal homeostasis in cold conditions. In addition to the insulation provided by body fat and the increase in heat production via shivering thermogenesis, a resting individual will attempt to conserve heat via peripheral vasoconstriction and the countercurrent heat exchange mechanism. This ultimately increases insulation because less blood will perfuse the cutaneous circulation, thereby lessening heat loss to the environment. Recent work has shown that chronic low-dose aspirin in humans lessens cutaneous vasodilation during heat stress, 10 but the effects of aspirin on cold-stressed individuals is yet to be determined. Rewarming following a cold stress typically results in a short-term drop in core temperature as skin temperature rises and heat production declines. 11 This has been termed “the afterdrop” but, currently, no information is available in regards to the influence of aspirin on this phenomenon. Because aspirin decreases core temperature and the thermoregulatory response is increased during a cold stressor, there is potential for an additive effect of these factors on an individual's response during acute cold exposure.
With the incidence of cardiovascular disease on the rise, it is likely that recreational athletes and tourists may be on a low-dose aspirin regimen. In addition, most first-aid kits contain high-dose aspirin for headaches and muscle aches. Therefore, individuals who are exposed to a wilderness survival situation and are taking aspirin may have an increased chance for hypothermia because of its potential impact on body temperature.
Thus, in the current investigation, we sought to determine the effects of a 1-week regimen of high-dose aspirin, low-dose aspirin, and placebo on thermoregulation during 2 hours of acute cold exposure in 12°C, and 2 hours of rewarming in 25°C. We hypothesized that both low-dose aspirin and high-dose aspirin would cause a greater decline in rectal temperature compared to placebo during this 4-hour laboratory study.
Methods
Subjects and Pre-Experimental Testing
Seven healthy men between the ages of 18 and 40 years volunteered to participate in this investigation. None were taking medication and each person signed an informed consent in accordance with the guidelines set forth by the Kent State University Human Subjects Review Board, which approved this study.
During the first visit to the laboratory, height and weight were measured via a stadiometer and balance beam scale, respectively. Percent body fat was determined by a 7-site skinfold measurement,12,13 and body surface area was calculated as previously described. 14 Peak aerobic fitness (peak VO2) was then determined following standard procedures. 8 Briefly, subjects pedaled on an electronically braked cycle ergometer (Lode Excalibur 1300 W, The Netherlands) until volitional fatigue. The workload started at 60 watts and increased by 20 watts each minute. A metabolic cart (Parvo Medics True Max 2400, Sandy, UT) was used to determine VO2 peak.
Aspirin Dosing Regimen
The current investigation employed a single-blinded within-subjects design. The participants were unaware of the ingestion order, but the research team knew that the placebo (cellulose) was always taken first, followed by low-dose aspirin (81 mg · day−1), and lastly high-dose aspirin (650 mg · day−1). This nonbalanced design was chosen because of concern over how high-dose aspirin may impact platelet function (low-dose aspirin inhibits platelet Thromboxane B2 for approximately 7–10 days), and this would have necessitated conducting studies in the summer months (ie, after a 30-day washout period), when thermoregulation could have been affected due to seasonal effects. 15 All participants underwent a 7-day dosing period (placebo, low-dose aspirin, high-dose aspirin) prior to each cold stress and rewarming session because 7 consecutive days of low-dose aspirin ingestion has been shown to reduce platelet Thromboxane B2 by more than 95%. 16 The 81 mg · day−1 dose was chosen because it is the recommended dose by the American Heart Association to help lower the chances of a heart attack. The 650 mg · day−1 dose was chosen because it consists of 2 normal, over-the-counter aspirin pills, which most people consume when attempting to treat a headache.
Experimental Trials
Each experimental trial consisted of a 30-minute baseline period (25°C), 2 hours acute cold exposure (12°C), and 2 hours rewarming (25°C). Because of the 7-day ingestion periods (placebo, low-dose aspirin, high-dose aspirin) and subsequent washout periods, all experimental trials were separated by approximately 2 weeks. Subjects were instructed to refrain from alcohol and physical activity for 24 hours preceding each trial. Additionally, subjects were instructed to refrain from consuming any food, caffeine, or caffeine-containing beverages for the 12-hour period prior to reporting to the lab. On the morning of the trial, subjects took their pills with 2 pieces of toast.
Upon arrival at the Applied Physiology Laboratory, subjects were instructed to void and insert a rectal probe (ER400-12, Respiratory Diagnostic Products Inc, Irvine, CA) 13 cm beyond the anal sphincter for the purpose of monitoring Tre. Subjects were also outfitted with skin thermistor probes (Model #409B, Yellow Springs Instruments Inc, Yellow Springs, OH) on the tricep, chest, thigh, calf, and forearm. Thermistors were secured with Hy-Tape for the purpose of measuring mean skin temperature. 17 Temperature probes were then interfaced with a data acquisition system (iNet-100HC, Omega Engineering Inc, Stamford, CT) that was, itself, interfaced with a desktop personal computer. Expired air samples were collected using the metabolic cart; the Weir equation was used to determine heat production (W/m2). 18 Baseline measurements (25°C) were obtained as the subject sat quietly on a plastic lounge chair, wearing only boxer shorts (approximately 0.07 Clo).
After completing the baseline period, the subject was wheeled into the environmental chamber (Western Environmental, Napa, CA) where they were required to remain seated and quiet during acute cold exposure at 12°C air for 120 minutes. After 120 minutes of acute cold exposure, rewarming began when the air temperature of the chamber was increased to 25°C (duration approximately 15 minutes). Body temperatures were monitored continuously and recorded at predetermined time-points while expired air samples were collected for 5 minutes at the end of each 30-minute interval (Figure).
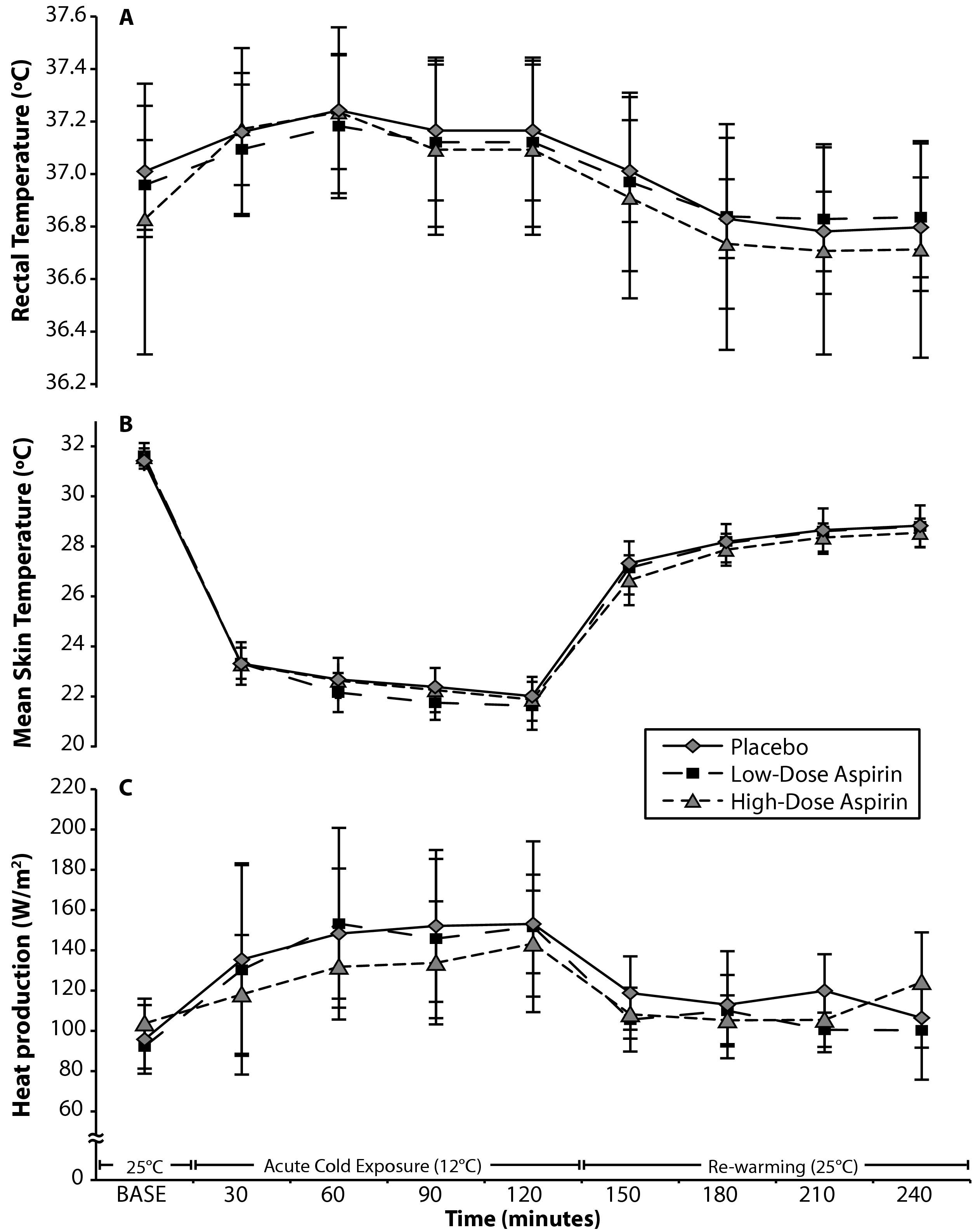
Thermal and metabolic responses to 120 minutes of acute cold exposure followed by 120 minutes of rewarming. A, rectal temperature. B, mean skin temperature. C, heat production. All changed over time but there were no treatment differences. Data is presented as mean ± SEM.
Statistical Analysis
All statistical analyses were performed with SPSS (version 18; SPSS Inc, Chicago, IL). A 3-treatment (low-dose aspirin, high-dose aspirin, and placebo), 9-way analysis of variance was conducted for each of the dependent variables (Tre, mean skin temperature, and heat production). In those situations where the repeated observations violated the assumption of sphericity, the subsequent P values for the within-subjects effects were adjusted using the Greenhouse-Geyser estimate. The level of significance was set a priori at P ≤ .05 and all data is presented as mean ± SEM.
Results
The participants in this study were of average height, weight, body fat, and peak aerobic fitness (Table 1). Following repeated measures analysis of variance, Tre, mean skin temperature, and heat production all revealed a main effect for time, but none demonstrated an effect for treatment or treatment by time interaction. As expected, Tre increased during acute cold exposure and decreased during rewarming (Figure, A), mean skin temperature decreased during acute cold exposure and increased during rewarming (Figure, B), and heat production increased during acute cold exposure and decreased during rewarming (Figure, C). There were no treatment differences at any time point. As such, we rejected our initial hypothesis that a 7-day aspirin regimen would facilitate a greater decline in Tre during the 4-hour experiment.
Participant characteristics
Discussion
Under the conditions of the current experiment (ie, moderate cold exposure and moderate rewarming of nonhypothermic men), aspirin had no effect on thermoregulation. While this was in contrast to our hypothesis, a number of areas for future research can be garnered from this investigation.
The responses of Tre, mean skin temperature, and heat production (Figure) were consistent with previous studies in this area. 19 Although it appears that high-dose aspirin reduced Tre during the baseline period, this trend was not significant in our small sample (n=7) of healthy young men. During acute cold exposure and rewarming, the responses in these variables were nearly identical regardless of treatment. Aspirin has both thermoregulatory and cardiovascular effects, but it appears that the body's defense of maintaining core temperature in 12°C air is unaffected by a 7-day aspirin regimen. This response may be due to several factors, including the variation in fitness levels of the participants, the variation in the actual aspirin dosage per kg of body weight ingested by the participants, or an inadequate degree of cold stressor.
A number of limitations and questions arise from this study. The first and most important issue is whether hypothermic subjects would show a different response than the nonhypothermic subjects in this study. One could argue that the air temperature in the current study was not cold enough to elicit a treatment effect if, in fact, one did exist. This is unlikely because an approximately 10°C reduction in skin temperature and a 2- to 3-fold increase in heat production was seen, indicating that thermoregulatory adjustment (ie, shivering and vasoconstriction) had occurred. The lack of counterbalancing, the small number of subjects, and the single-blinded design are not ideal, leaving the possibility that the subjects developed some degree of acclimation by the third visit (ie, the high-dose aspirin treatment). Esophageal temperature was not used in this study despite it being a more sensitive measurement of body temperature. 20 Therefore, it is possible that aspirin has an effect that we were not able to detect due to these limitations. Irrespective of aspirin treatment, interindividual differences in body weight and aerobic fitness may have impacted one's response to the cold exposure, thereby increasing variability in the measurements. Lastly, whether aspirin affects the intermediate modulators of thermoregulation (eg, hormones, platelets, and peripheral blood flow) under these conditions was not measured and remains to be determined.
Conclusions
People with atherosclerotic heart disease typically consume low-dose aspirin each day; athletes take high-dose aspirin to treat a headache or muscle soreness. Our data do not support an important effect of aspirin on whole body thermoregulation during exposure to 12°C and subsequent rewarming.
Footnotes
Acknowledgments
This investigation was supported by a grant from Research and Graduate Studies at Kent State University. The authors wish to thank Anne Muller for her assistance in preparing the figures.
This project was presented as an abstract at the 2005 ACSM National Meeting, Nashville, TN.