
Abstract
Objective
To describe injuries and illnesses treated during an expedition-length adventure race and combine the results with those from previous studies to identify common patterns of injury and illness during these events.
Methods
The 2003 Subaru Primal Quest Expedition Length Adventure Race was held in Lake Tahoe, CA, from September 5 to 14, 2003. Eighty teams of 4 individuals participated. During the event, medical volunteers providing on-site medical care recorded each medical encounter on a medical encounter form. This information was used to describe the injuries and illnesses treated and was combined with previous investigations to identify common patterns of injury and illness during these events.
Results
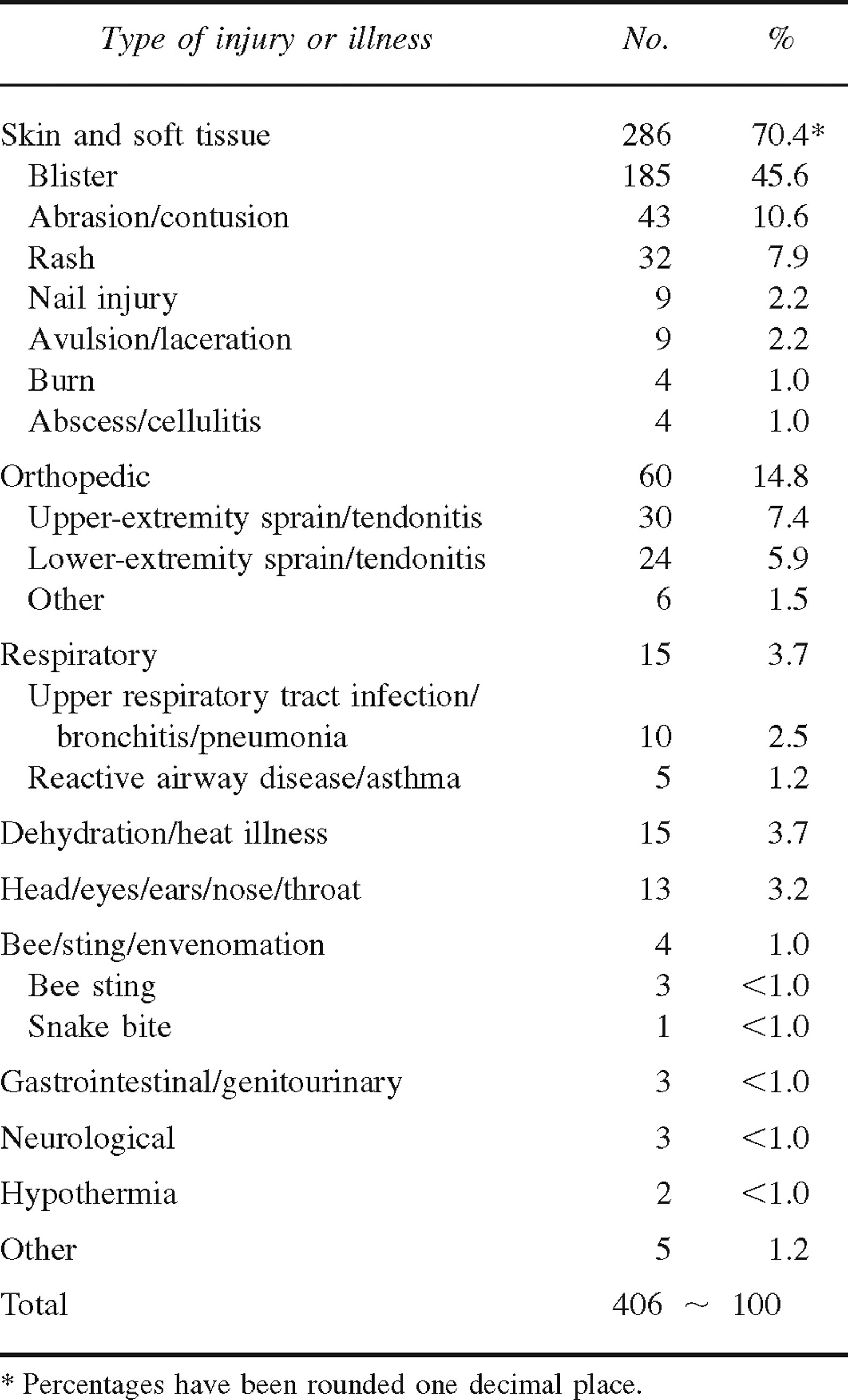
During the 10-day study period, 356 patient encounters and 406 injuries and illnesses were recorded. The most frequent reason to require on-site medical care was injury of the skin and soft tissue (70.4%), with blisters the single most common of these injuries (45.6%). Other reasons were orthopedic injury (14.8%), respiratory illness (3.7%), and heat illness or dehydration (3.7%).
Conclusions
The results of this and previous studies demonstrate a common pattern of injury and illness that includes a high frequency of skin and soft tissue injury, especially blisters. Injuries and illnesses such as altitude illness, contact dermatitis, and respiratory illness varied considerably among events. The number of patient encounters per athlete is similar among the studies, providing an approximation of the number of medical encounters expected given the number of participants. These results should assist medical providers for future events; however, it is imperative to carefully review the individual event to best predict the frequency of injury and illness.
Introduction
In adventure races or wilderness multisport endurance events, participants compete over a course that requires performance of multiple disciplines typically including climbing or rappelling, flat- and white-water boating, mountain biking, orienteering, trail running, and trekking. Events are held in wilderness environments and range in duration from 4-hour “sprint” races to “expedition-length” races lasting from 36 hours to 10 days.
The origin of adventure racing may be traced to early multisport events, including Hawaii's Ironman Triathlon, which began in 1978, and New Zealand's Coast to Coast, which began in 1983. Adventure racing has grown in popularity and is now one of the fastest growing sports in North America and throughout the world, with high-profile expedition-length races such as the Eco-Challenge, the Primal Quest, and the Raid Gauloise.
In addition, numerous shorter races are held worldwide each year. At the time of this writing, there were 140 scheduled races in North America sanctioned by the United States Adventure Racing Association for 2005. 1
There are several previous descriptions of the provision of medical support and the injuries and illnesses treated during adventure races. 2 –8 This study describes injuries and illnesses treated during an expedition-length adventure race. In addition, the results are combined with previous investigations to identify common patterns of injury and illness during these events. The information should prove useful to those providing on-site medical support for future, similar events.
Materials and methods
The 2003 Subaru Primal Quest Expedition Length Adventure Race (PQ 2003) was held in Lake Tahoe, CA, from September 5 to 14, 2003. Eighty coeducational teams of 4 individuals each (320 athletes total) began the 455-mile course that included approximately 245 miles of mountain biking, 85 miles of trekking, 55 miles of flat-water boating, 30 miles of in-line skating, 30 miles of white-water boating, and 10 miles of orienteering.
Teams varied from having a lot of experience with corporate sponsorship to those having little or no experience in expedition-length adventure racing. As required by the rules of the event, each team had at least 1 member of each sex. Teams were composed of 3 men and 1 woman or 2 men and 2 women. The participants ranged in age from 20 to 54 years, and one third were women. During the event, the average temperature was 13°C (range of −1°C to 26°C) with an average humidity of 53%. Altitude ranged from sea level to 12 000 feet.
More than 40 vol.nteer medical personnel, including physicians, nurses, paramedics, emergency medical technicians, wilderness first responders, and medical students, provided on-site medical support. Care was delivered in 10 medical tents under the guidelines developed by the Race Medical Director, who is board certified in emergency medicine, and outlined in the Race Medical Support Plan. The medical tents were located along the racecourse at “transition areas” where athletes transitioned from one discipline to another. In addition, a helicopter and 3 ambulances equipped with advanced life support were on site during the event.
All patient encounters were recorded on medical encounter forms. Information included racer number, a description of the injury or illness, the treatment rendered, the clinical course, the presumptive diagnosis, and the disposition. The information contained on the forms was used for the study. Medical encounters with race staff, crewmembers, and other nonracers were excluded. The study received approval from the Human Subjects Division at our institution.
Finally, the results of our investigation were compared with those of previous studies in an attempt to identify common patterns of injury and illness during these events.
Results
During the 10-day study period (September 5–14, 2003), 356 patient encounters and 406 injuries and illnesses were recorded. The discrepancy resulted from athletes presenting with more than 1 injury or illness at a single time. When this occurred, it was recorded as 1 encounter but each injury or illness was counted separately. Skin and soft tissue injuries accounted for 70.4% of all encounters, with blisters accounting for 45.6% of all these injuries. Other encounters included orthopedic injuries (14.8%), respiratory illness (3.7%), and dehydration or heat illness (3.7%). A complete list of the type and frequency of injury and illness is shown in the Table Table. Six athletes required transport to the hospital. The reasons for these transports were cellulitis, closed head injury, compartment syndrome, hypothermia, pneumonia with reactive airway disease, and renal colic.
Discussion
In the development of a race medical support plan, one should base staffing, equipment, and supplies on anticipation of need. One of the biggest challenges facing providers of medical support for these events, however, is anticipating the type and frequency of injury and illness that will be encountered. Although there are several studies describing injury and illness during adventure races, because of the wide variety of geographic and environmental conditions in which these events are held and the different disciplines included, it is unclear to what degree the results can be generalized and applied to other events. 3 –6 This study describes injuries and illnesses treated during an expedition-length adventure race and, in combination with previous studies, identifies some common patterns of injury and illness during these events. This information should prove useful for providers of medical support for future, similar events.
Injury and illness by type and frequency
In both investigations, the most frequent reason to require medical care during the event was skin and soft tissue injury, accounting for 70.4% (PQ 2003) and 48.0% (PQ 2002) of medical encounters. 4 Blisters were the single most common reason to require medical care, accounting for 45.6% (PQ 2003) and 32.8% (PQ 2002) of medical encounters. 4 These results would suggest that providers of on-site medical support for future events should be prepared to treat a large number of skin and soft tissue injuries, especially blisters.
Abrasions (or contusions) and rashes were the next most frequent reasons to require medical care, accounting for 10.6% and 7.9% of medical encounters. All the rashes were plant-induced dermatitis from poison ivy encountered during a trekking section of the course. In the study of PQ 2002, rashes were less common, accounting for only 1.3% of medical encounters. 4
Tendonitis of the upper extremity accounted for 7.4% of medical encounters. The majority of these injuries were sustained during the first section of the race that was 55 miles of open-water kayaking. During PQ 2002, there was no open-water kayaking section, and the majority of orthopedic injuries involved the lower extremity, with few cases of upper-extremity tendonitis. 4
During PQ 2002, respiratory illness and altitude illness accounted for 18.2% and 11.9% of medical encounters.4,6 In our investigation, respiratory illness accounted for only 3.7% of medical encounters, and there were no cases of altitude illness. In comparing the results from PQ 2002 with those from PQ 2003, the discrepancy in the occurrence of altitude illness is easily explained by the difference in both starting altitude and altitude gain during the 2 events. The reason for the difference in frequency of respiratory illness is less clear. Townes et al 4 offer poor air quality from forest fires in the area and the outbreak of a viral respiratory illness during PQ 2002 as possible explanations for the high incidence of respiratory illness observed in their investigation. Given the potential morbidity and mortality from delayed treatment of respiratory illness, these results suggest that on-site providers should be prepared to care for a large number of patients for respiratory illness during these events.
There are some common injury and illness patterns that should prove useful for medical personnel supporting future events. It is clear that medical personnel should be prepared to treat a large number of skin and soft tissue injuries, especially blisters. This has important implications in terms of staffing, training of staff, and stocking of supplies. It also highlights the importance of having providers such as podiatrists available to provide direct patient care and training of both racers and staff.
Certain types of injury and illness, including altitude illness, orthopedic injury, respiratory illness, and rash, appear to be more variable among events. It is therefore essential to consider factors such as the course, location, environmental conditions, altitude, weather, and disciplines included when trying to anticipate injury and illness in the development of a medical support plan.
For example, the frequency of altitude illness should be roughly predictable based on the altitude of the course. Tendonitis of the upper extremity may be associated with events with lengthy sections of open-water boating. In addition, one might anticipate a higher frequency of rash, including plant-induced dermatitis, in an area where certain plants or microbes are indigenous.
One limitation of the study is that different providers completed the medical encounter forms, resulting in inherent variation in the determination and accuracy of the diagnosis recorded. An example is heat illness, which potentially represents a wide range of diseases. In addition, the medical encounter forms contained only a presumptive diagnosis, and no follow-up or final diagnosis was obtained. Finally, because expedition-length adventure races occur in a wide range of environments and conditions with a variety of disciplines, even when the results are combined with previous studies some caution should be used when applying the results to other events.
Provision of on-site medical support for expedition-length adventure races is both exciting and challenging. The results of our investigation further support the previous finding that providers of on-site medical support should be prepared to treat a wide variety of both injury and illness.3,4 The results of this and previous investigations indicate that it is possible to anticipate the type and frequency of certain injuries and illnesses; however, each event is unique, and it is essential to understand the variables that might influence injury and illness for an individual event. One should “hope for the best but prepare for the worst” in developing a medical support plan. It is hoped that as more events are held and investigations undertaken, more complete and accurate information will become available to improve on-site medical care for participants in these events.
Footnotes
1
The authors report no conflict of interest and have received no external sources of funding in preparation of this manuscript. Offprints will not be available from the corresponding author.