
Abstract
Objective
Rock climbing’s popularity continues to rise, with people of all ages regularly participating in the sport. Climbing literature suggests climbers get injured mostly in their upper extremities. Most studies on climbing injury analysis are conducted retrospectively, with all the inherent problems of a retrospective setup (no exact time collection, biased injury perception, etc). Prospective data are still missing.
Methods
We prospectively evaluated all attendees of a major German indoor climbing gym in Stuttgart, Germany, with bouldering and lead climbing facilities. Attendee’s age, sex, and time spent climbing were electronically recorded on each visit. All acute injuries were graded using the Medical Commission of the Union Internationale des Associations d’Alpinisme Score. Injury cause, belayers’ and climbers’ experience, and outcome were additionally analyzed.
Results
During a 5-year period (2007–2011), 515,337 visits to the climbing wall were registered, of which 63.6% were by male visitors, 36.4% female, within an age of 8–80 years (median, 34 years). The average time of climbing was 2 hours 47 minutes. Thirty climbing injuries were recorded, 22 were in male and 8 in female climbers with a total mean age of 27.5 ± 10.6 years. Acute injuries happened in 6 cases while bouldering, in 16 cases while lead climbing, in 7 cases while top roping, and in 1 case as a third person (not climbing or belaying) while watching another climber. Bouldering injuries were mostly the result of falls onto the mat, whereas in lead and top rope climbing various scenarios happened. Fifteen (50%) injuries were Medical Commission of the Union Internationale des Associations d’Alpinisme grade 2, 13 (43%) were grade 3, and 2 (7%) were grade 4, with no fatalities. The overall injury rate was 0.02 injuries per 1000 hours of climbing activities.
Conclusions
This was the first study to accurately record time spent indoor climbing digitally and evaluate the acute injuries prospectively in a large cohort. There were few injuries sustained, suggesting indoor climbing has a low risk of acute injury per 1000 hours of participation. The injuries were of minor to moderate injury severity, and no fatalities occurred. Several injuries could have been avoided, and further injury-prevention concepts should be developed.
Introduction
The rise in popularity of indoor rock climbing started about 15 years ago and still continues. Nowadays almost every major city in Germany has at least one large indoor climbing gym; the number of competitions held in theses gyms is on a constant rise as well. Although some forms of rock climbing, such as solo climbing or alpine traditional climbing, and clean climbing show a larger injury risk, indoor and bolted sport climbing have proved to be relatively safe. 1 –8 The overall number of injuries is small, and the injuries are mostly of minor severity.1,2 Nevertheless there is still a risk of a fatal injury. A lower overall injury risk was observed for indoor climbing than for outdoor rock climbing.1,2 Limb 9 reported 0.027 injuries/1000 h and Schöffl and Winkelmann, 8 0.079 injuries/1000 h for indoor climbing. For competition climbing, which is mostly performed indoors, or at least at an artificial wall, an injury risk of 3.1/1000 h is reported. 10 Most of these studies recorded data retrospectively and therefore may be biased. In comparison with other sports, the injury rate per 1000 hours of sports performance is a widely used parameter. Until now these hours were only calculated but never exactly recorded for climbing studies.1,2 Also, retrospective analysis with questionnaires does not report fatalities. We therefore performed a prospective analysis of all attendees in a major indoor climbing gym during a 5-year period with a direct electronic time recording.
Methods
We prospectively evaluated all attendees in a big climbing gym in a major German city during a 5-year period. Climbing time was directly documented electronically. Every climber has a membership ID card that is swiped and recorded digitally on entry and when exiting the gym. The aim of the study was to evaluate the acute injury rate per 1000 hours of sports performance and to evaluate the injury severity. The exact age of climbers was registered beginning from the age of 13; children younger than 13 were not registered individually. Nevertheless, children are allowed to climb in guided groups from an age of 8 years on, and their climbing time is thus considered as an individual of group training. Younger children only climb occasionally with their parents, but this climbing time was not registered for this study. Thus, for the age analysis only the median is considered from the age of 13 years. Further influencing factors were also analyzed including climbing experience (beginner, intermediate, expert, or professional; Table 1). The grading is based on technical climbing skills training (belaying, rope work, etc), not the actual climbing skills related to grades of climbing difficulty levels. For example, one of Germany´s top climbers who is a top-ranking World Cup athlete only qualified as expert but not as professional, as he has no additional degree as a climbing instructor. Also, the climbing experience of the belayer was classified accordingly.
Climbing experience
Documentation Of Climbing Time
The major aim of the study was to evaluate the acute injury rate per 1000 hours of sport performance as exactly as possible. To evaluate the climbing time, all individual attendees to the gym were registered electronically checking in and out during a time frame of 5 years (2007–2011). From this measured time of attendance, 20 minutes for a change of clothing was deducted. The remaining time was then considered “climbing time,” or “climbing activity time” (including belaying time of the climbing partner, warm-up, etc). When people came as part of a climbing course, no individual time registration was accurately possible (less than 10% of all attendees). In these cases, the average climbing time of all attendees was used. All measured climbing activity times of more than 5 hours were replaced through the overall average climbing time, as more than 5 hours probably was an error caused by neglecting to check out electronically. All climbing times of less than 1 hour were erased as less than 1 hour was probably not a climbing visit.
Injuries
All injuries that required immediate medical attention, through either a paramedic or a doctor on site (all cases in which an ambulance was called), were recorded as injury events, and a follow-up was performed. This includes the possibility that an accident was recorded even if the climber was uninjured as every case in which an ambulance was called was defined as an injury event. It also implicates the possibility of an injury not being recorded if the climber sought medical help afterward. Chronic overuse injuries were not analyzed. All injuries were graded using the Medical Commission of the Union Internationale des Associations d’Alpinisme (UIAA MedCom) score 11 (Table 2). Follow-up on the injury, reconvalescence, and an assessment of possible permanent damage was performed. Further, influencing factors such as climbing experience (Table 1), style of climbing (top rope, lead, boulder), injury cause, belay technique, and injury cause were analyzed.
Injury and Illness Severity Classification (IIC)—UIAA MedCom Score 11
Results
During a 5-year period (2007–2011), 515,337 visits to the climbing wall were registered: 63.6% were male, 36.4% were female, within an age of 8–80 years (median, 34 years; Figure 1). The average time of climbing was 2 hours 47 minutes ± 1.71.
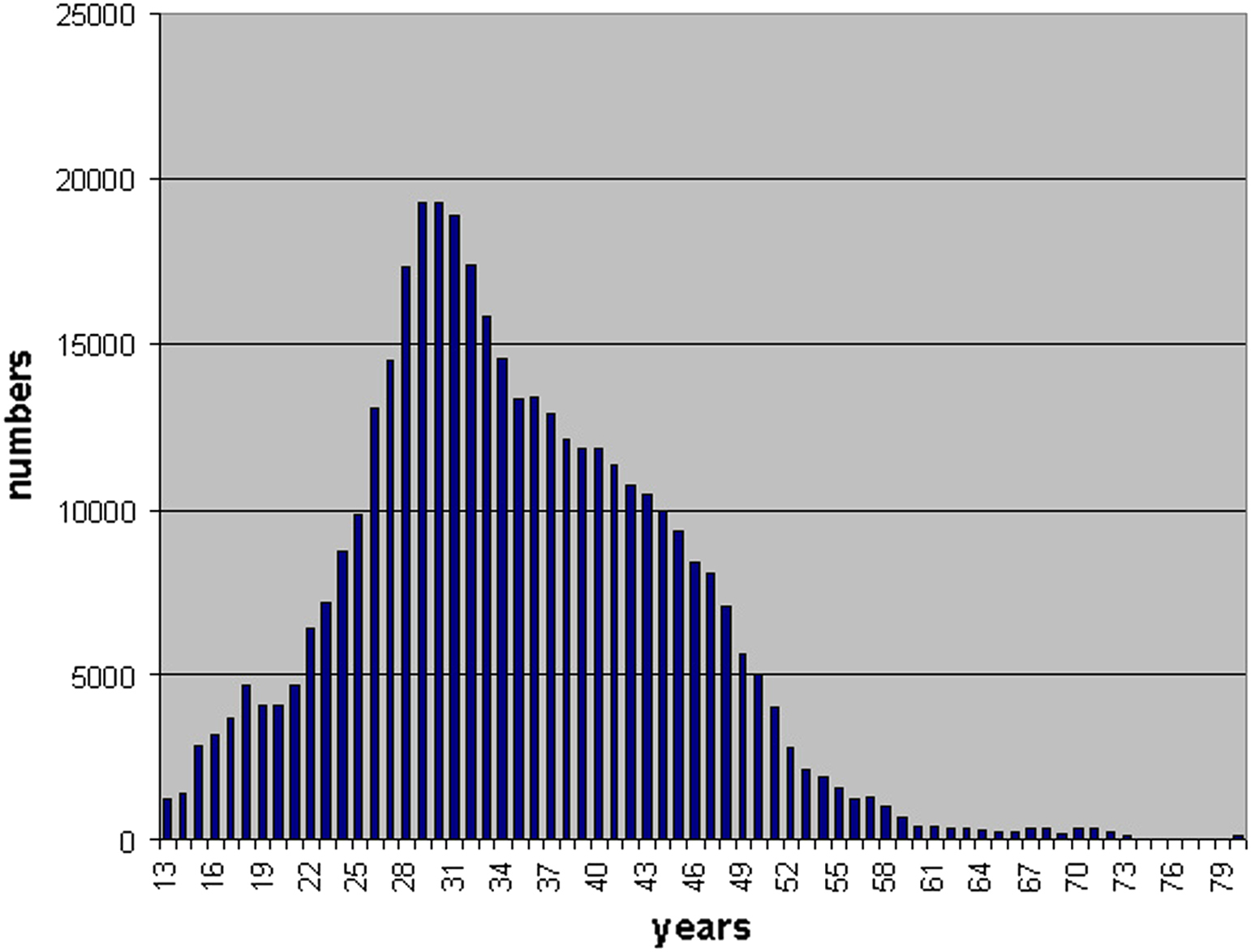
Age distribution.
During the study period, 32 acute injury events were recorded. Two of these were in nonclimbers (spectators) and therefore were deducted. One of these was a 7-year-old who fell on the stairs and bit his lip, the other was a 40-year-old male nonclimber with a cardiac incident.
Of the climbing injuries, 22 occurred in male and 8 in female climbers with a total mean age of 27.5 ± 10.6 years. For the injury distribution, grading, and analysis, see Table 2. Injuries happened in beginner climbers in 5 (16.7%), in intermediate climbers in 16 (53.3%), in experts in 6 (20%), and in professionals in 3 (10%) cases. Injuries happened in 6 cases while bouldering, in 16 cases while lead climbing, in 7 cases while top roping, and in 1 case as a third person (not climbing or belaying) while watching another climber. Bouldering injuries were mostly the result of falls onto the mat, whereas in lead and top rope climbing, various scenarios occurred. Fifteen injuries were UIAA MedCom grade 2, 13 were grade 3, and 2 were grade 4 injuries (Table 3).
Injury events
T, top rope; L, lead; B, bouldering; O, others.
Climbing experience belayer is not considered in boulder accidents, the “Munter hitch” belay technique is also known as the “Italian hitch” or “crossing hitch” or “HMS”.
The acute injury risk in males was 1 injury per 47,742 hours of sports and in females 1 injury per 46,735 hours. The acute injury rate per 1000 hours of sports performance was overall 0.02/1000 h and equal in women and men. For the relative injury risk see Table 4.
Injury risk
Discussion
Various studies 1 –8 have analyzed the injury risk in climbing activities already, yet little work has been done prospectively and no study could determine climbing time exactly. 2 With the present analysis we could collect the climbing time very accurately, as all individual climbers checked in and out electronically. The acute injury risk per 1000 hours of climbing sport activity was consistent during the 5-year period, and the sex distribution was even. Sex distribution in the literature is inhomogeneous. Jones et al 6 found an odds ratio of 1.01 of male sex for a climbing injury, whereas Josephsen et al 5 found little or no influence of sex. Neuhof et al 3 also described that more male than female climbers had a history of at least 1 climbing injury. In our present study, 22 injuries were in males and 8 were in females. Considering the fact that more male climbers were registered, the relative injury risk was evenly distributed between both sexes. Climbing experience is not a guarantee for not having an accident, as the climbing experience of the belayer counts as well. In the present study 3 climbers of the professional group were injured, but in 2 cases the injury cause was not the climber’s fault but that of the belayer (in 1 incidence the belayer was an expert and in 1 an intermediate). Only in 1 of these cases did the climber get injured; in the other the belayer who performed the belaying fault got injured himself. In the third case the injured professional climber was bouldering, thus no belayer was involved.
Climbing Style
As expected most injuries happened during lead climbing, followed by top roping and bouldering. Nevertheless, the high number of 7 cases (23%) of injuries while top roping seems surprising, as top rope is considered as rather safe. 2 Some of these injuries in top roping were just incidental, for example, shoulder (No. 21) or patellar dislocation (No. 26). Others were owing to belay mistakes, for example, giving too much slack rope or, more serious, tying the knot wrong (also in 1 case in lead climbing). To avoid these mistakes the German Alpine Club recommends the standard of a “partner check” before leaving the ground, 12 which was lately also noted in the medical literature for patient safety. 13 The partner check consists of 4 steps: check that all harness fastenings are locked, check your partner’s knot, check that the screw gate belay carabiner and belay device are locked and used in their proper ways, and check that the free end of the rope is tied onto the rope bag. 12 Each of these 4 steps should be performed by both climbers. This point is crucial to avoid these injuries and must be performed in all types of climbing. However, the most serious top rope climbing injury (No. 11) happened as a sequela of 2 mistakes. The leading climber climbed a route in lead style in which a top rope was already correctly installed. He did not climb the full length of the route and thus did not clip the final belay point with a double screw gate carabiner (which is the standard of the gym) providing absolute safety on the top, as there was a top rope already set up there. Instead he stopped at the last belay point before the anchors and got lowered down. The climbers should have pulled through the previously used lead climbing rope. They did not. The second climber did not then use the correctly set-up top rope but the incompletely rigged rope of his partner. He climbed up, unclipping all carabiners, including his highest and last belay point. Thus, he unclipped all his belays, which resulted in a free fall onto the ground when he tried to sit in his top rope.
Injury Cause
The most frequent injury cause was a belay mistake in 10 of 30 cases. This suggests that better belay training could be a means of injury prevention in the future. Coauthor G.H. is currently working on the development of a fall simulator to enable better belay training. In bouldering, falls onto the mat were the most frequent injury causes. These falls onto the mat frequently result in sprains and dislocations. We are currently working with the national bouldering team on fall training with methods adopted from martial arts. If these trainings were included in general boulder training, these types of injuries might be reduced. Nevertheless, there are no scientific studies yet to prove its effectiveness on boulder injury prevention. Whether other equilibrium and reflex training, such as slack line or postural training, has any benefit also needs to be further evaluated. Closure of the mats’ intersections is recommended as injury prophylaxis 2 ,8,14,15 and is already mandatory for international climbing competitions. One rare injury cause in our study was a dental injury caused by a climber’s mistake (Figure 2). In clipping the rope above the head, some climbers hold the rope with their teeth to free the hand to pull up more rope. In this case (No. 3), the climber fell just in the moment when he had the rope in between his teeth. As a natural sympathicotonic reaction, he clenched his teeth during the fall, keeping the rope between them until the rope tightened. The rope pull caused a serious jaw fracture and multiple avulsed teeth. To avoid this injury in the future, climber education is necessary, and thus this case has already been discussed in climbing-specific literature. 15
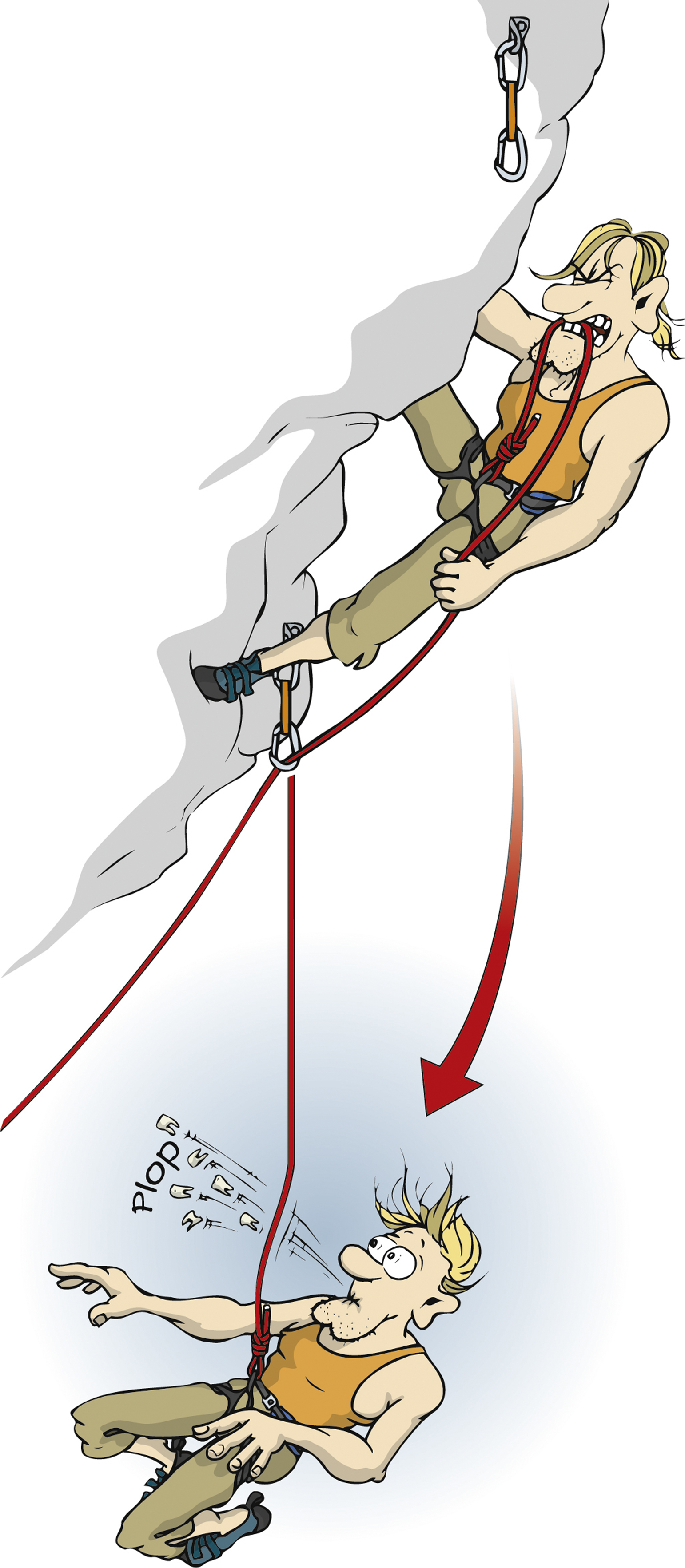
Pathomechanism of the dental injury. Illustration used with permission from the German Alpine Club (DAV).
Types Of Injury And Injury Grade
More injuries in our study involve the lower extremity (12) than the upper extremity (6) or the trunk (6). So far, most research indicates that the upper extremity is the most injured body region in nonalpine rock climbing. 1 ,2,16–22 However, in another recent study on rock climbing injuries, traumatic injuries involved the lower extremities (foot, toe, and ankle) in 50%, whereas upper extremities accounted for 36% of the injuries. 22 Neuhof et al 3 found an even injury distribution between the upper (42.6%) and lower extremities (41.3%). Most injuries involved fractures, sprains, and dislocations, which is consistent with the literature. 2 ,3,23–25 Nine injuries left a permanent disability (2 of these were only a high probability). This question has not yet been addressed scientifically. For the exact injury description, see Table 1.
Fifteen (50%) of the injuries were grade 2 injuries according to the UIAA MedCom score, 11 13 were grade 3, and 2 were grade 4. Luckily, no fatality occurred. Few studies used a common scoring model so far. Schöffl et al 1 performed a post hoc National Advisory Committee for Aeronautics (NACA) classification of the injuries reported in the present studies. Overall, the majority of injuries in outdoor and outdoor climbing were of minor severity (NACA 1 and 2). Finally, after the implementation of the UIAA MedCom score in 2010, 26 a climbing and mountaineering sport-specific scoring model that also accounts for the patient’s outcome exists. Neuhof et al 3 surveyed 699 injuries of 1962 sport climbers and found 81.4% were UIAA MedCom grade 2, 18.2% were grade 3, and 0.4% were grade 4, for a total of 6 injuries. Grade 1 injuries were neglected in this study, as well as in the present analysis. This is also consistent with the studies of Limb, 9 Schöffl and Winkelmann, 8 and Schöffl and Küpper. 10
Time-Related Injury Risk
The main focus of the present study was a prospectively conducted acute injury risk evaluation. Our study is the first that precisely registered climbing time, whereas others could only use retrospective data with a possible bias. 1 –3 The acute injury risk per 1000 hours of sports performance was 0.02 and was evenly distributed between both sexes. It was also almost evenly distributed during the five years analyzed. The injury risk is comparable to that shown in other studies for indoor climbing8,9 and equal to the study of Neuhof et al, 3 who analyzed acute injuries in bolted sport climbing indoors and outdoors. In comparison with many other sports, 1 the injury risk is small and the injury severity mostly minor with a potential fatality risk.
Conclusions
Bolted sport climbing, especially indoors, has continuously demonstrated over several studies, including the present one, an acute injury risk of 0.01 to 0.03 injuries/1000 h of sports performance. The injury severity is mostly minor to moderate, with the potential of a fatal accident still present. Our study demonstrated that several of the injuries would have been avoidable through a reduction of individual mistakes. The German Alpine Club advocates a system of a partner check, 12 a system that is also promoted in the medical risk management discussion. 13 Mistakes such as “tying the wrong knot” can be avoided. Nevertheless, this would have avoided only 2 injuries in our study, case numbers 8 and 28. Belay mistakes were quite common in the present study, so further training should emphasize belayer technique and not only the falling lead climber. 27 Dynamic belay techniques may help to serve as potential injury prevention. One limitation of the present study is the fact that it was conducted only in 1 gym, which might be particularly well run and therefore may present a better safety record than other indoor climbing walls. As the general injury risk in climbing is low, some climbers might underestimate the existing dangers that are also present in indoor climbing. Therefore, fall simulators might be useful to train the belayer about the dangers, forces, and techniques to minimize the consequences of a climber’s fall. The analysis of injury cause is essential to discover new injury mechanisms, 2 for example, the dental injury through the rope between the climber’s teeth in case number 3 and preventive precautions. As there are still no internationally recognized qualifications or criteria to become an indoor climbing instructor, there should be further potential to standardize and improve these qualifications and thus increase the safety records of indoor climbing gyms. The German Alpine Club also discusses the necessity of a climber’s license to guarantee the necessary climbing and belaying skills for a safe performance of the sport. Even if this might seem a bit arbitrary to someone who has climbed for 30+ years, it may increase the safety of all participants. Nevertheless, no scientific proof is yet given that a climber’s license would actually decrease an injury risk.