
Abstract
Objective
To identify the frequency and pattern of spinal injury sustained in mountaineering accidents.
Methods
All patients with spinal injuries sustained while mountaineering who were treated at the Queen Elizabeth National Spinal Injuries Unit from 1992 to 2001 were studied. Information was obtained from hospital notes, and each patient completed a questionnaire.
Results
Twenty-one patients with spinal injuries sustained in mountaineering accidents were identified. Fourteen patients (67.7%) were experienced mountaineers. Four (19.0%) were rock climbing, 6 (28.6%) were winter climbing, 6 (28.6%) were hill walking, and 5 (23.8%) were winter walking. Ten patients (47.6%) sustained cervical injuries, 5 (23.8%) sustained thoracic injuries, 5 (23.8%) sustained lumbar injuries, and 1 (4.8%) sustained cervical and lumbar injuries. Nineteen patients (90.5%) sustained fractures, 1 (4.8%) sustained a dislocation, and 1 (4.8%) sustained a fracture dislocation. Seventeen patients (81.0%) were neurologically intact, 2 (9.5%) sustained complete cord injury, and 2 (9.5%) sustained incomplete cauda equina lesions. Ten patients (47.6%) required internal fixation of their fractures. Fourteen patients (57.1%) sustained other significant injuries.
Conclusions
This is the first study specifically aimed to describe patterns of spinal injuries and their outcomes in mountaineers. The group we studied had sustained fractures at differing spinal levels with no specific injury pattern. The incidence of cord injury was lower than in other spinal injury patient groups. The majority had also sustained other significant and potentially distracting injuries. Prehospital care providers should maintain a high suspicion of spinal injury in this group.
Introduction
Mountain rescue teams in Scotland rescue more than 300 individuals every year. 1 Many of these individuals have sustained serious injuries, most commonly resulting from falls. 1 Mountain rescue teams are called upon to rescue and treat these injured casualties in remote and often inhospitable environments.
Two previously published studies considered injuries sustained by Scottish mountain climbing casualties.2,3 One study 3 examined 333 casualties rescued in Scotland during a 2-year period. The study described an incidence of spinal fractures in Scottish mountaineers of 6 cases per year; however, it did not describe the details and levels of fractures. The second study 2 was not specific about spinal injuries sustained.
Spinal injured patients are a uniquely vulnerable group, with the major risk of spinal cord damage. Management of acute spinal injury patients therefore presents a special challenge to all prehospital care providers, and we are not aware of any previous studies in these patients with injuries occurring as a result of mountain accidents.
We wished to examine this group with the aim of improving knowledge and understanding of such injuries in walkers and climbers for mountain rescue and medical personnel.
Methods
We carried out a retrospective study with the spinal injuries unit database. This computerized patient database contains detailed information on 1400 patients treated in the unit from 1992 to 2001 and includes details of the cause of injury. We identified patients who had sustained a spinal injury while they were mountaineering in Scotland in this 10-year period. We also reviewed the hospital case notes of these patients.
A questionnaire was completed for all patients in the group by telephone or by mail (see Appendix, available at
Injuries sustained while skiing and climbing incidents occurring on crags near roads were excluded.
Setting
The Queen Elizabeth National Spinal Injuries Unit (SIU) is sited in a university teaching hospital in the west of Scotland. The SIU offers a service to all patients in Scotland (population 5.1 million) with actual or threatened spinal cord damage. Computed tomography and magnetic resonance imaging are available in the regional neurosurgical unit situated in the adjacent building. Operative spinal fixation, if required, is performed in the unit. In 2000 the unit received 200 acute admissions.
Patients are referred from hospitals throughout Scotland. They are transferred to the unit by land ambulance or helicopter when their condition allows. Some mountain casualties are transferred directly by helicopter from the accident scene to the accident and emergency department in the hospital. In many cases, prolonged distances are involved in the transfer of patients to the unit. The majority of mountaineering accidents in Scotland occur in areas that are more than 100 km from the SIU. 1
Results
Twenty-one patients with spinal injuries sustained in mountaineering accidents were treated at the SIU during the study period. Patient age range was from 16 to 71 years (mean 34 years). Sixteen (76.2%) were male.
Fourteen patients (67.7%) in the study group described themselves as experienced, which was defined as having climbed more than 50 Scottish mountains higher than 3000 feet. Activities at the time of injury varied. Four casualties (19.0%) were rock climbing with use of ropes at the time of the accident, 6 (28.6%) were winter climbing, 6 (28.6%) were hill walking, and 5 (23.8%) were winter walking. Nineteen patients (90%) sustained their injury as a result of falls, and 2 (10%) were caught in avalanches.
The levels of spinal injury are shown in the Figure. Nineteen injuries (90.5%) were fractures, 1 (4.8%) was a dislocation, and 1 (4.8%) was a fracture dislocation. Ten (47.6%) patients required internal fixation of their fractures. Fourteen of the patients (57.1%) had at least 1 other significant injury, including long bone fractures and head and chest injuries.
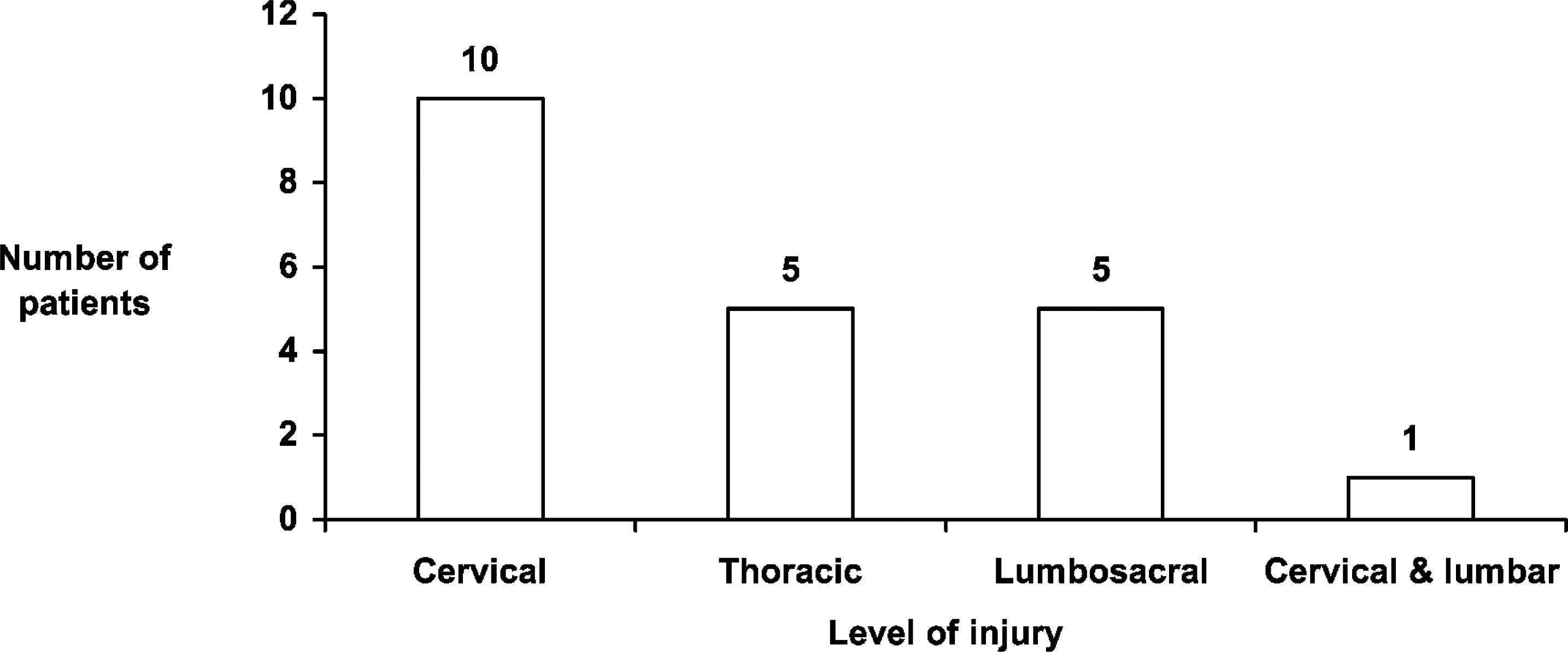
Level of spinal injury (n = 21).
Seventeen (81.0%) patients were neurologically intact. Two (9.5%) patients sustained complete cord injuries, 1 at the level of the 4th cervical vertebra and 1 at the level of the 12th thoracic vertebra. Two patients (9.5%) sustained incomplete cauda equina lesions.
Discussion
Mountain rescue teams in Scotland rescue approximately 300 casualties each year. Approximately half of these individuals have sustained injuries or illnesses.2,3 Little is known about the specific nature of their injuries and their prehospital care needs, as few studies have been carried out.
The Queen Elizabeth National SIU provides a unique focus for the management of spinal injury from a geographically distinct area. As a national service, the unit accepts all traumatic spinal injury patients with significant cord injury and approximately one third of cord-intact patients from a population of 5.1 million. We therefore believe that it is unlikely that any patients with paralysis have not been included in this study.
Two previously published studies include descriptions of spinal injuries in mountaineers.5,6 In one, 5 the results of necropsies carried out in a convenience sample of 42 mountaineers who died in mountain accidents in Scotland revealed that 14 victims had sustained spinal injuries: 8 cervical, 5 thoracic, and 1 lumbar fracture. Interestingly, in this group 7 of the 8 cervical fractures were at or above the fourth cervical vertebra. A similar distribution of spinal injuries is described in a study examining mountain accidents in Sierra Nevada during a 5-year period. 6 Of 215 injured climbers, 9 had sustained spinal injuries: 4 cervical, 3 thoracic, and 2 lumbar. Neither study comments on the presence or absence of associated cord injury.
Spinal injuries in mountaineers appear to be heterogeneous and do not follow any specific pattern. This is probably related to the variety of mountain activities, mechanisms of injury, and the differing heights of falls.
More than half of the patients in this group had other significant injuries in addition to spinal injury. The Advanced Trauma Life Support system of patient care highlights the difficulties in identifying spinal injuries on clinical assessment alone without the aid of radiological imaging. 7 This is especially the case where the patient is experiencing pain from another “distracting” injury.
Assessment of a well-clad casualty in a cold environment is particularly difficult. Prehospital care providers should have a high suspicion of spinal injury in patients injured in the mountain environment. This should be the case even in the absence of symptoms or signs and especially when other injuries are present.
Of all patients admitted to the SIU, 35% have a complete spinal cord injury. In the study group, however, only 2 patients (9.5%) had complete cord injuries, and 2 (9.5%) had incomplete cord injuries. This difference may be related to a number of factors. The mechanisms and force of injury in mountaineering accidents may differ from those of other types of accidents that cause spinal injury in SIU patients, most commonly road traffic accidents (Scottish Trauma Audit Group, Royal Infirmary of Edinburgh, oral communication, 2001). Also, this difference may be attributed to the often prolonged prehospital times in the mountain environment. Individuals sustaining complete spinal cord injury in the remote mountain setting may die from their injuries or hypothermia because of the relatively prolonged time for prehospital care providers to arrive and the time for transport to hospital. Individuals may survive similar injuries if they occurred in an urban environment.
We would suggest that the low incidence of spinal cord damage in the study group also demonstrates that injured individuals are being handled and transported appropriately by mountain rescuers in Scotland.
The optimal equipment for spinal immobilization for prolonged evacuations is a cervical collar and vacuum mattress. The vacuum mattress is more comfortable than a spinal board 8 and is less likely to give rise to pressure areas. The vacuum mattress is molded to the casualty, providing maximal immobilization of the whole spine. It is not possible to transport spinal boards to casualties in the mountain environment because of their size and weight.
All mountain rescue teams in Scotland are equipped with vacuum mattresses and cervical collars, which provide optimal spinal immobilization. 5 We suggest that this practice continue. Logrolling and optimal handling of patients is also possible with the relatively large number of trained personnel who are present at a rescue.
Many individuals who undertake mountain sports and sustain injuries are young; the average age in this group was 34 years. The social, psychological, and economic effects of injury in this group are considerable. This is especially the case with spinal injuries, which have prolonged recovery and rehabilitation times in addition to possible impaired functional outcome.
This study included only spinally injured mountaineers admitted to the SIU. Although we believe that all Scottish patients with cord injury are treated at the SIU, a number of patients with spinal fractures but no cord injury are treated by clinicians in other hospitals.
Conclusions
This is the first study specifically aiming to describe patterns of spinal injuries and their outcomes in mountaineers. The group we studied had sustained fractures at differing spinal levels with no specific injury pattern. The incidence of cord injury was lower than in other spinal injury patient groups. The majority had also sustained other significant and potentially distracting injuries.
Although Scottish mountains are relatively small by world standards, they provide a wide range of mountaineering environments, often in arctic conditions. We suggest that our findings may be relevant to mountaineering in the greater ranges.