
Abstract
Heat illness is a condition that is sometimes seen in those undertaking physical activities. This case report focuses on a female hiker who developed heat stroke during a trek in the Dachstein region of Upper Austria. The patient's presentation was initially unclear and could only be confirmed by the use of a thermometer. This had a significant impact on the medical decision-making process during a complex rescue operation.
Introduction
Hyperthermia is an abnormally high body temperature due to an insufficiency of thermoregulation without a general threshold value. It is often, but not exclusively, caused by exposure to excessive heat or exertion and can lead to life-threatening complications such as heat stroke, which is defined as a core temperature of ≥40°C and is characterized by headache, nausea, vomiting, neck pain or stiffness as a sign of meningeal irritation, dizziness, convulsions, paralysis, altered or loss of consciousness, and organ failure.1–3 These symptoms often can be found in other diseases. Therefore, temperature monitoring and appropriate treatment should be routinely considered, especially in the context of the current climate emergency, because hyperthermia is more likely to occur in the alpine environment.
Case Report
In the summer of 2021, a group of 4 hikers undertook a tour in the Dachstein region of Upper Austria. Their intention was to traverse the Krippenstein plateau, ascending by cable car and descending via a steep path, a route of approximately 13 km and a maximum altitude of 2000 m on a dry limestone plateau, estimated to take a whole day. All 4 hikers were in good general health and of average physical condition. The weather conditions were stable and mild, with temperatures reaching up to 25°C, humidity of 55%, and wind speed of 7 kilometers per hour (km·h–1) under clear skies, resulting in a heat index of 25. Overnight conditions stayed stable, with temperatures going down to 13°C after midnight, without clouds and a wind speed of 2 km·h–1.
The group was equipped and dressed appropriately for such a hike. They started later than they intended (1100), and the crossing of the plateau was uneventful until they started to descend along a poorly marked path in the early evening. At around 2100, a 28-year-old woman suddenly lost consciousness and remained unresponsive, prompting an emergency call.
The Austrian Mountain Rescue Service responded with 28 rescuers and called for additional medical assistance due to the unclear scenario and the prolonged evacuation in nighttime conditions. In this terrain, airborne rescue was not possible. Two emergency physicians arrived on the scene within 2 h of the call with advanced medical equipment, including a patient monitor.
The evacuation was already underway, with the patient presenting with a Glasgow Coma Score (GCS) of 8 (eye opening to pain, no verbal response, localized motor response), deviation of the eyes to the right, and hot, dry skin without a rash.
The patient showed drowsiness and agitation and did not tolerate noninvasive blood pressure (NIBP) measurement or a tourniquet for intravenous access. Respiratory rate was 25 breaths/min with very deep breaths and peripheral oxygen saturation (SpO2) >90% at all times. Blood glucose was normal (8 mmol·L–1), and the patient had strong femoral pulses and a sinus tachycardia of 140 beats/min. Body mass index was 25.6 kg·m–2. These findings did not yet lead to a neurologic diagnosis to explain the patient's condition.
Temperature monitoring was established with a portable patient monitor (for electrocardiogram, NIBP, temperature, and SpO2) carried up by the physicians. A probe was inserted in the inguinal fold (because rectal or axillary access was not tolerated by the patient), and the initial reading of 40.7°C, clarifying the picture and suggesting a heat-related etiology such as heat stroke with subsequent cerebral edema.
The evacuation took ∼5 h, with periods of rappelling followed by steep, secured descents. The patient was immobilized on a stretcher and vacuum mattress and left uncovered. Active cooling could not be performed because snow or water was not present under summer conditions. During the evacuation, the patient’s body temperature decreased to 39.1°C, with a steady decrease in heart rate to 100 beats/min and respiratory rate to 15 breaths/min at the time of handover to the emergency medical service. Assisted ventilation was never performed, and supraglottic devices were not tolerated at any time because the neurologic status remained unchanged with the GCS not rising >9.
The patient was transferred to a regional hospital, intubated, and admitted to the intensive care unit. A computed tomography scan of the brain showed no evidence of cerebral edema. However, blood tests showed signs of multiorgan injury: acute renal injury with rhabdomyolysis, hepatic injury without coagulopathy, and systemic inflammatory response of unknown origin (Table 1). The urine drug screen was negative, and echocardiography showed a reduced ejection fraction of 40%. A computed tomography scan of the chest, abdomen, and pelvis revealed a menstrual cap. This was subsequently removed. Only after initial stabilization was it discovered that the patient had left the menstrual cup in place for a week when a daily change is recommended for this device.
Test results at hospital admission.
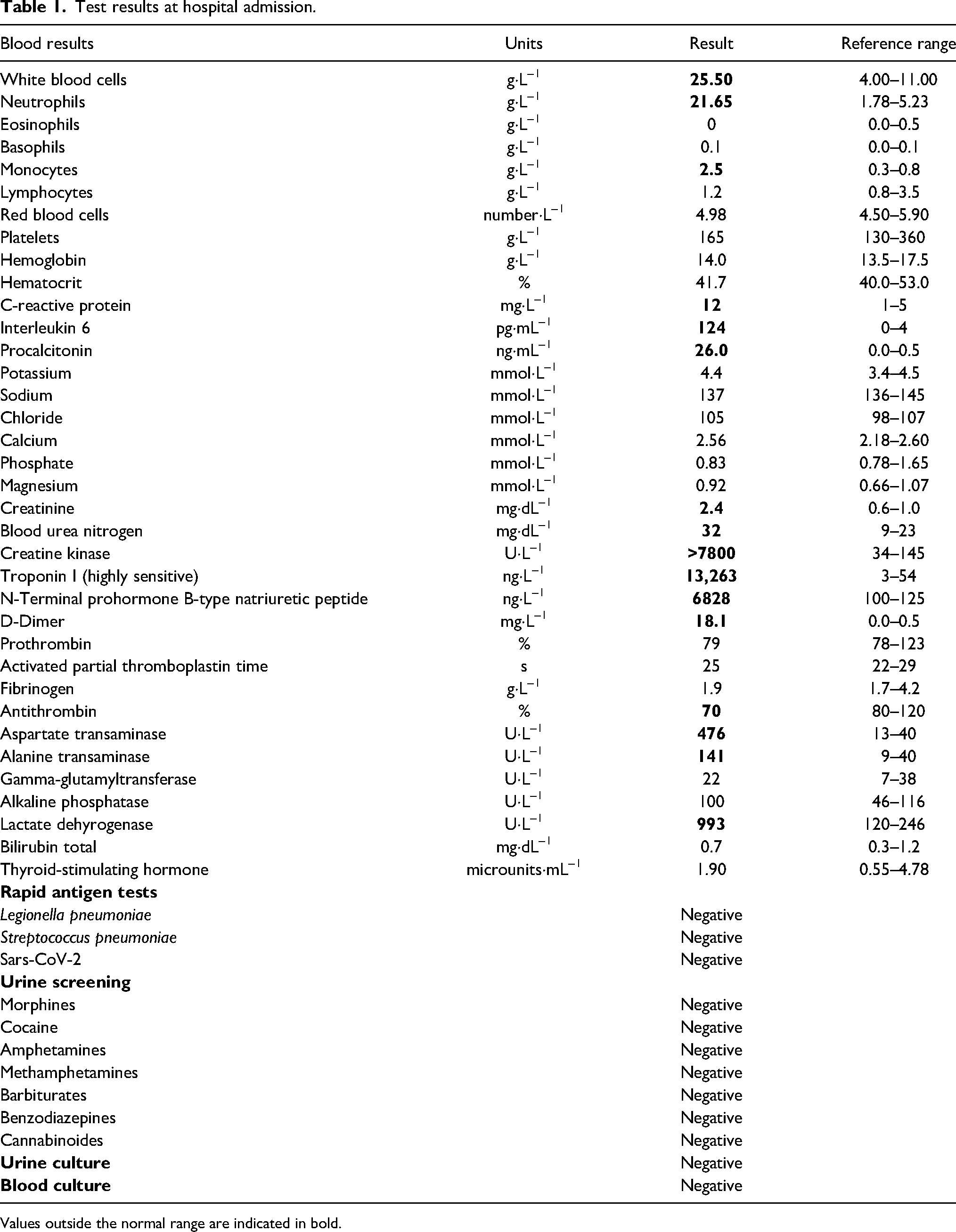
Values outside the normal range are indicated in bold.
Antibiotic therapy for possible occult infection, potentially arising from the retained menstrual cup, and hemodialysis were initiated, and organ function recovered steadily. The patient was extubated after 2 d and was discharged and repatriated to her home country without neurologic impairment after 11 d in intensive care and a total hospital stay of 18 d.
Discussion
We present the case of a patient with elevated body temperature and cardiorespiratory and neurologic symptoms of unclear etiology. Differential considerations at the time, prior to knowing the body temperature, included the following: 1) seizures were possible, but the patient had no such prior history, and no seizures were witnessed by her friends or responders; 2) intracerebral hemorrhage, tumor, or stroke was unlikely to occur in a young, healthy individual with no medical history; and 3) exhaustion as the main cause was possible, but the patient was hemodynamically stable prior to collapse and did not appear to be excessively fatigued. In this case, the diagnostic pathway could be effectively narrowed by establishing continuous temperature monitoring. 1
Hyperthermia and fever are both characterized by elevated body temperature but differentiated by their trigger stimuli. 4 Fever and infection may have contributed to the elevated body temperature, but to an unclear extent. Elevated interleukin 6 and especially procalcitonin suggest an infective cause as a cofactor, but this could not be proved by microbiologic findings (initial blood cultures were taken on admission and vaginal swabs 4 d after admission). Furthermore, the patient had no history of systemic inflammatory or autoimmune diseases.
Unprotected exposure to sunlight and the sudden onset of symptoms, however, pointed to exertional heat stroke as the underlying cause with the confounding variable that the heat index on that day was low.
Immediate conductive cooling would have been an effective way to lower body temperature and stabilize the patient. 2 In this environment, neither snow nor water was available, and water supplies carried by the rescuers were scarce and reserved for drinking.
The patient experienced agitation from NIBP measurement, resulting in continuous cuff activity due to motion artifacts and thus no valid measurement. Instead, peripheral pulses were monitored and found to be strong at all times. Fluid resuscitation would have been a preferred option in a severely hyperthermic patient with additional systemic inflammatory respsonse. 5 However, fluid resuscitation was deferred pending patient deterioration because the quantity of crystalloid fluids available was small.
The microcirculation remained relatively uncompromised. In the emergency room, the first lactate values did not exceed 1.9 mmol·L–1, steadily decreasing thereafter, with base excess −8.8 and mild hyperventilation.
Sedation often would be an appropriate measure to reduce stress, but because the patient was calm without medical intervention, did not appear to be in an epileptic state, and was also showing intact airway reflexes (swallowing), it was kept as an option and never performed.
Protective intubation would have been a possible consequence of sedation or a compromised GCS of <9. In an alpine environment with a belayed evacuation lasting several hours without sufficient oxygen, narcotics, and a ventilator, this would definitely cause more problems.
The patient was transported supine rather than in the lateral decubitus position for 2 reasons: the terrain was initially very steep, leading to a semiprone position with less chance of vomiting, and the stretcher used, equipped with a central wheel, could easily be tilted to the side if necessary.
Throughout the mission, the rescue team discussed the competing priorities of optimizing therapy, avoiding evacuation delays, and complicating logistics. Decisions in such circumstances are different from algorithms or guidelines and require clinical experience. The medical considerations seemed appropriate in the situation once the body temperature could be measured and monitored continuously. The cause of severe hyperthermia stayed unclear, with outside temperature, exertion, and occult infection all potentially contributing to it.
Toxic shock syndrome as the sole cause of the patient's condition was possible, but it was challenged by the examining gynecologist. The discovery of a menstrual cup in situ may have had an impact on the rapid deterioration of the patient's condition 6 while her 3 companions remained uncompromised in a comparable state of fitness and training. Vaginal examination showed greenish discharge. Swab cultures of the discharge taken 4 d after hospital admission were negative, but these findings may have been false-negative results because they were obtained after the start of systemic antibiotic therapy.
Conclusion
We have presented a case of severe hyperthermia in an alpine environment with both exertional heat stroke and possible occult infection as contributing etiologies. Severe hyperthermia is an uncommon event in temperate climates in exercising individuals and therefore may be unrecognized or misinterpreted due to the wide range of nonspecific symptoms and the lack of temperature measurement. 2
Monitoring devices have become powerful tools even in remote emergency situations and should be considered in prolonged operations to identify trends in the patient's clinical condition. They may help direct treatment when resources are limited or when a demanding evacuation precludes following guidelines or standard procedures.
Especially with climate change, heat stroke should be considered in the differential diagnosis of altered mental status in temperate environments.
Footnotes
Acknowledgments
The authors thank Peter Paal for technical assistance and Nathaniel Thiem for language review.
Author Contribution(s)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.