
Abstract
Objective
To determine whether volunteers (with or without prior medical training) can correctly apply pressure immobilization (PI) in a simulated snakebite scenario after receiving standard instructions describing the technique.
Methods
Twenty emergency medicine physicians (residents and attendings) and 20 lay volunteers without prior formal medical training were given standard printed instructions describing the application of PI for field management of snakebite. They were then supplied with appropriate materials and asked to apply the technique five separate times (twice to another individual [one upper and one lower extremity] and three times to themselves [nondominant upper extremity, dominant upper extremity, and one lower extremity]). Successful application was defined
Results
The technique was correctly applied as judged by the preset criteria in only 13 out of 100 applications by emergency medicine physicians and in only 5 out of 100 applications by lay people. There was no significant difference in success rates between physicians and lay volunteers. Likewise, there was no significant difference in success based on which extremity was being wrapped. More detailed analysis revealed that the major contributor to failure was inability to achieve recommended target pressures.
Conclusions
Volunteers in a simulated snakebite scenario have difficulty applying PI correctly, as defined in the literature. The major source of failure is an inability to achieve recommended pressure levels under the dressing. New methods of instructing people in the proper use of PI or new technologies to guide or automate application are needed if this technique is to be used consistently in an effective manner for field management of bites by venomous snakes not known to cause significant local wound necrosis.
Introduction
There are estimated to be over 3000 snakebites in Australia each year, about 500 of which are inflicted by venomous snakes and result in 2–3 fatalities. 1 Throughout the world, specific antivenom is the definitive treatment for snake venom poisoning, but it is generally only available in a hospital or clinic setting. Numerous factors such as cost, need for advanced capabilities in administering the drug, and potential life-threatening reactions tend to limit use of antivenom outside of a hospital setting. Thus, field management techniques have been developed in an effort to delay absorption and spread of venom until the snakebite victim can get to the hospital where antivenom is available. The pressure immobilization (PI) technique is a first-aid measure that was developed by the Australians in the 1970s. 2 This technique involves wrapping as much of the bitten extremity as possible with a bandage (e.g., crepe or elastic bandage). The extremity is then immobilized with a splint or sling. The victim's activity must be minimized as much as possible while being evacuated to a hospital. The theorized mechanism of action involves inhibition of venom uptake by the lymphatics and superficial veins. 2 It has been demonstrated in a human mock venom model that the pressure levels achieved beneath the encompassing bandage must be within a relatively narrow range (55–70 mm Hg applied to the lower extremity and 40–70 mm Hg to the upper extremity) for venom absorption to be delayed. 3 Pressures outside these ranges were ineffective.
Small studies in primate models2,4,5 and anecdotal cases in humans 6 –8 have demonstrated the benefit of this technique in limiting snake venom spread. Others, however, have reported notable failures with the technique.9,10
When individuals are taught the technique, the instructions are usually to apply the wrap with the same tension “as you would apply to a sprained ankle.” 11 To our knowledge, no one has systematically evaluated whether such instructions are adequate to enable individuals to apply the technique correctly, so that it will have a high likelihood of being effective. It was the purpose of this study to evaluate whether two groups of individuals (those with no prior formal medical training [lay subjects] and emergency medicine physicians [medical subjects]) could, when given standard printed instructions, apply the PI technique correctly.
Subjects and methods
Forty volunteers (20 lay subjects without prior medical training and 20 emergency medicine physicians) were recruited for this prospective study. The lay subjects consisted of Stanford University undergraduate students recruited in public areas on campus. These students were screened to ensure that they had no prior formal first aid or wilderness medicine training. The emergency medicine physicians were all recruited from the Stanford University Division of Emergency Medicine and included 7 residents and 13 attending physicians. After consenting to the study, each volunteer was given a copy of standard written instructions describing and illustrating the proper method of applying PI for field management of a snake bite (Figure 1). 11 Volunteers were not informed of the precise purpose of the study and were not given specific target values for pressure in mm Hg, as these data are not routinely included in instructions given to those learning the technique.
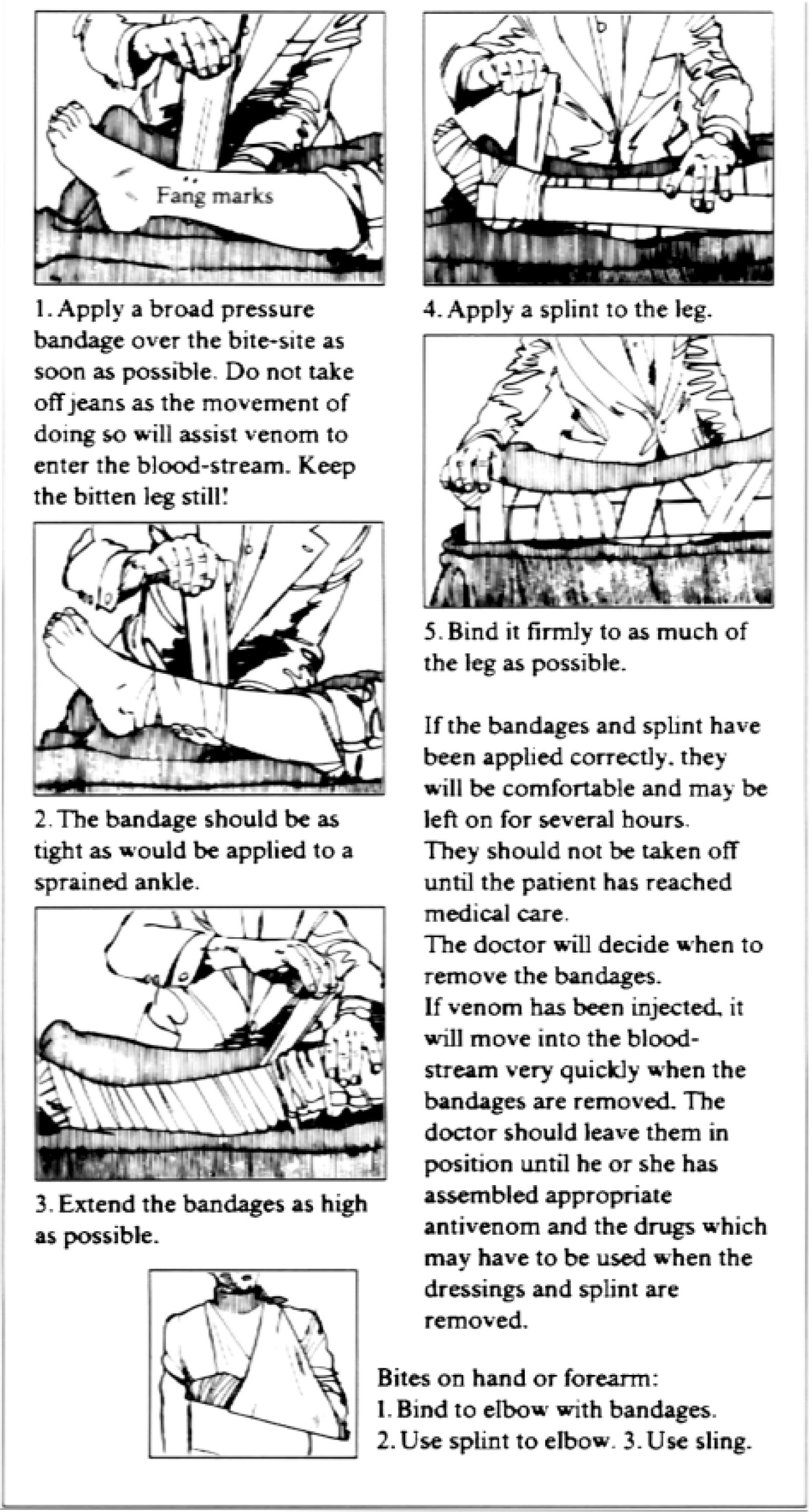
The Australian pressure immobilization technique instructions given to volunteers participating in this study. Reproduced with permission from Sutherland SK,
For each application of the technique, a specially designed skin interface pressure (SIP) measurement device was placed at the simulated snakebite site. This device consisted of a foam-filled plastisol-coated balloon (25 × 60 × 8 mm) connected by flexible PVC capillary tubing to a handheld case containing a SenSym SDX05D4 pressure transducer, Burr-Brown INA126P instrumentation amplifier, and Soar 3020 digital voltmeter. Voltmeter readings were manually recorded and later converted to mm Hg, using a calibration table that took into account the SIP device's gain and offset characteristics. The balloon was equilibrated to atmospheric pressure before each use to eliminate temperature and barometric artifacts. Subjects were blinded to their pressure measurements.
The subjects were provided with multiple elastic bandages (width: 4 inches; length: 4.5 feet), Sam Splints (The Seaberg Company, Inc., Newport, OR), and arm slings as materials to be used in applying PI. After reviewing the printed instructions on PI application, they were asked to apply the technique five separate times, in the following order: their own nondominant arm, their own dominant arm, their dominant leg, an investigator's arm, and an investigator's leg. Successful application was defined
Four components of successful application of pressure immobilization in the field
To avoid interobserver bias, a single investigator (JN), knowledgeable in the technique, graded the success or failure of each application. Each elastic bandage was used in no more than eight applications before being discarded, to avoid variability resulting from elastic fatigue.
Success scores between the two groups of volunteers were compared using the
This study was approved by the Stanford University Human Subjects in Medical Research Panel.
Results
Out of 200 total applications by 40 volunteers, PI was done completely correctly (getting all four aspects of the technique correct) in only 18 instances: 13 applications done by Emergency Medicine physicians and five by lay volunteers (Table 2). Success rates were not statistically different between the two groups. There was also no difference in success rates between the various extremities being treated. The major obstacle to complete success was an inability to achieve the recommended target pressures when applying the bandage as tightly as one would for a sprained ankle (Figure 2). Most subjects underestimated the amount of tension necessary to achieve target pressure. Subjects also failed to begin the wrap at the bite site, as per the instructions, almost half the time (44% of the time for medical volunteers and 45% of lay subjects). In all applications, volunteers achieved the other two measures of success: complete wrapping of the extremity and immobilization.
Performance measures in medical personnel and lay volunteers applying pressure immobilization according to standard written instructions. Each volunteer applied the technique a total of 5 times (for 100 total applications per group)

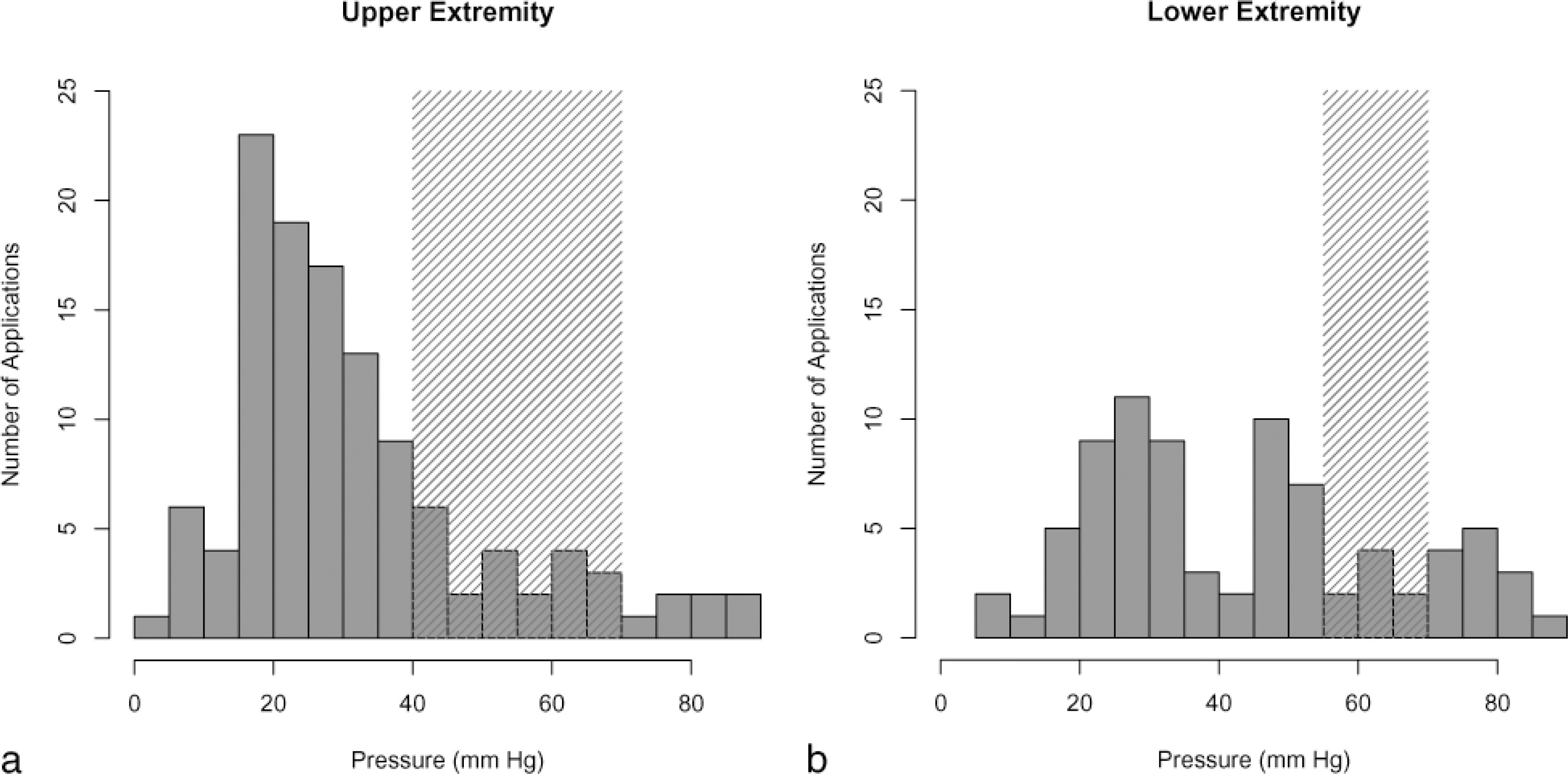
Summary of pressures generated for each application of pressure-immobilization (PI) to
Discussion
Snakebite mortality continues to be a problem, especially in Africa and Southeast Asia. It is estimated that in India, there are 10,000–50,000 snakebite fatalities a year, and there are about 1000 deaths each year in Burma (Myanmar) alone, where it is the fifth leading cause of death. 13 Although the snakebite mortality rate in Australia has fallen more than tenfold since the introduction of antivenom over 70 years ago, 1 there are still hundreds of envenomations there every year. In the United States, there are around 7000 venomous snakebites each year, 14 with approximately six deaths. 15 For many years people have sought an effective field management technique to limit the morbidity and mortality of venomous snakebite. Sutherland et al. first described the PI technique in 1979. 2
PI has been proven to limit the spread of certain snake venoms in animal models4,5 and has, anecdotally, appeared to be beneficial in some human cases of venomous snakebite. 6 –8 It has become the standard first-aid technique for snakebite officially recommended by the Australian Resuscitation Council and that country's National Health and Medical Research Council. 16 However, clinical failures with the technique have been noted as well.9,10
Prior research has shown that it is important to apply the technique correctly for it to be beneficial. Importantly, the pressures obtained under the wrap need to fall within fairly narrow ranges (40–70 mm Hg for the upper extremity, and 55–70 mm Hg for the lower). Howarth et al. 3 demonstrated, using a radio-labeled mock venom, that pressures outside these ranges actually enhance central spread of venom. Their theory is that pressures that are too low do not adequately impede venom spread, and pressures that are too high actually increase venom absorption as a result of fine muscle contractions stimulated by the tight bandage, resulting in increased muscle pumping action.
Our study is the first to formally evaluate whether people can actually apply the technique correctly when given “standard” written instructions, as used by the Australians. It is clear that, in most cases, when lay people or individuals with significant medical training attempt to apply the technique, wrapping the extremity as tightly as they would for a sprained ankle, they get the pressures wrong (usually underestimating the degree of tension that needs to be applied). It is interesting that there was no difference in success rate, depending on what extremity was being treated (i.e., volunteers were as unable to achieve appropriate pressures when applying the technique to another individual as they were when applying it to their own dominant upper extremity). Given the very low overall success rate, detection of any real differences in rates between the study groups would be hard.
It could be argued that pressures generated in applying PI to a real snakebite victim might be more likely to be correct because most “errors” in application stemmed from underestimation of the tension needed. It is possible that, with the stress of a real snakebite scenario, the tension applied to the wrap would be greater.
It would appear from our study that new approaches to teaching the PI technique might be necessary. It may be better to attempt to spread familiarity with the technique by doing public demonstrations of PI application and allowing people to actually experience how tight a “correct” application feels. This could be done in public health fairs and in public first-aid courses with the use of a pressure-measuring device to document that appropriate pressures have been achieved. Alternatively, it might be possible to develop devices specifically designed for use following the bite or sting of a venomous creature that would ensure that appropriate pressures are generated. Such a device might consist of a sleeve designed to be slipped over the bitten extremity and then inflated, with a pop-off valve designed to signal correct inflation and to prevent excess pressures. Further research and development, in terms of both educational and technological approaches to this technique, are needed.
One limitation of this study was that subjects did not receive any feedback on how tightly they had applied the pressure wrap. It is possible that they would have been more likely to achieve correct tension in the wrap if they had received such feedback after an initial application. We chose to blind our subjects to this information to simulate the way the public is currently generally instructed in the technique. Future research should explore whether subjects have greater success applying PI after receiving feedback based on prior attempts. In addition, retention by subjects of the ability to properly apply PI at some future time (e.g., 6 months to a year) after optimal training would be an interesting study of the perishable nature of this skill.
Another possible limitation to the study was that an elastic bandage was used for PI application, as opposed to a crepe bandage recommended by some authorities. 17 Current recommendations for the technique do, however, suggest that any form of flexible material can be used to apply the wrap (including clothing, towels, pantyhose, etc.). 17 It was our intent to use a product that is readily available to the public and often found in first-aid kits— the elastic bandage.
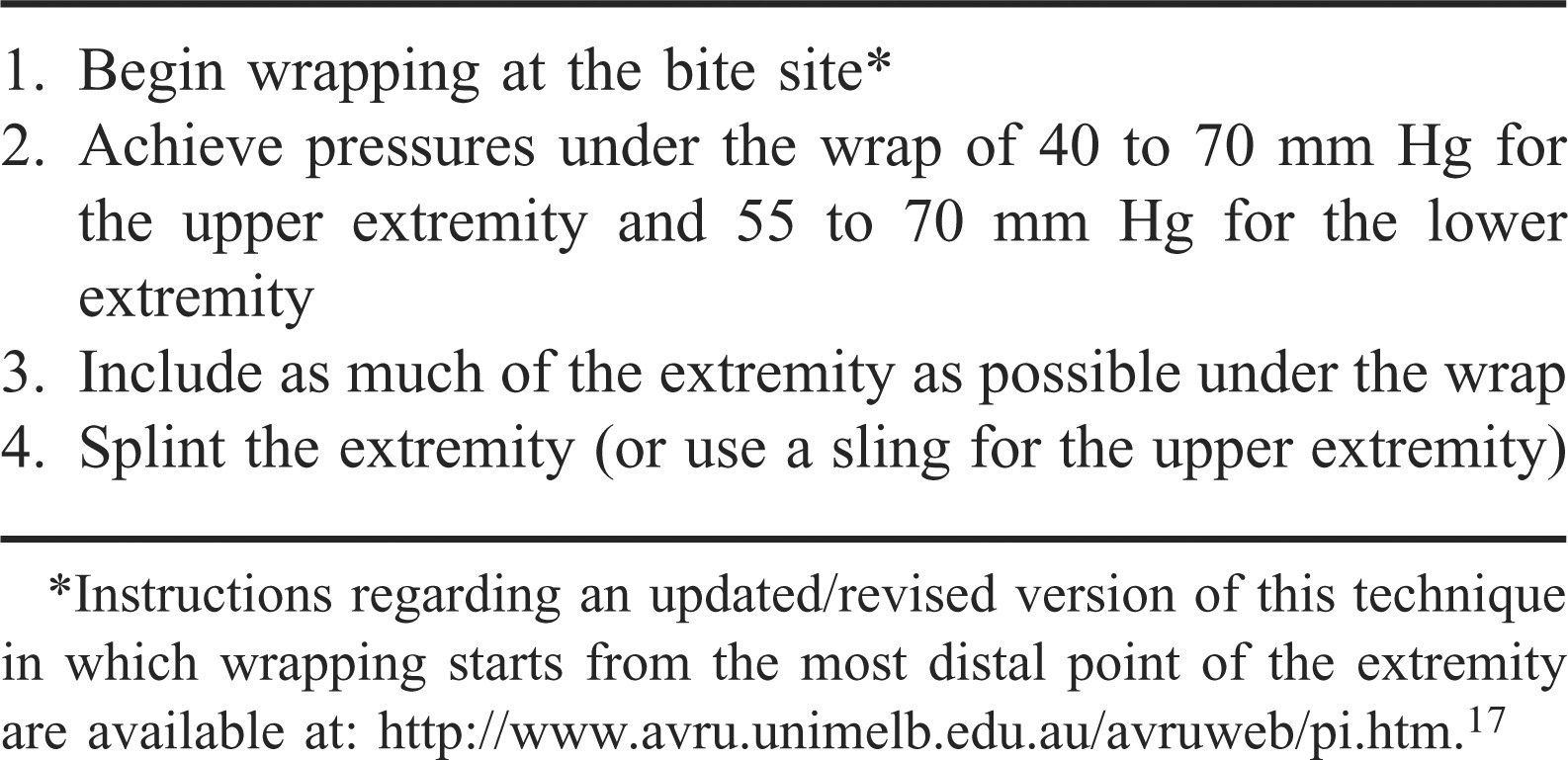
It should also be emphasized that there has been a recent change in the recommendations for application of PI. The new recommendation is to begin wrapping at the most distal point on the bitten extremity, as opposed to beginning at the bite site. 17 This change was made in an effort to make the technique simpler for people to apply, though either technique appears equally effective. The fact that, despite instructions, both groups of volunteers (physicians and lay people) failed to begin the wrap at the bite site in almost half of all applications supports this change in recommendation. A future study including this change in recommendation is planned.
Although PI, when applied correctly, appears to be very effective in limiting spread of many snake venoms (and spread of venoms of other creatures such as Australian funnel web spiders, the box jellyfish, blue-ringed octopus, and cone snails 17 ), this does not mean that it is an appropriate field management approach for bites by all venomous snake species. It is possible that application of this technique following the bite of a venomous snake known for its necrotic venom effects (e.g., many pit vipers) might do more harm than good. Severely restricting spread of necrotizing venom from the bite site could worsen the ultimate degree of local tissue damage. Given that approximately 99% of snakebites in the United States are caused by pit vipers, 14 and victims are at significantly greater risk of losing tissue than they are of losing their lives even without the use of any field management techniques, PI may not be appropriate for use in most venomous bites in this country. Exceptions would include bites inflicted by coral snakes, by sea snakes off the coast of southern California, and by imported exotic elapids not known to cause necrosis.
Conclusion
Volunteers have difficulty applying the proper amount of pressure when using PI in a simulated snakebite scenario, and new methods of teaching the technique or alternatives to automate its application are needed.
Footnotes
Acknowledgments
We thank Eric E. Sabelman, PhD, Research Biomedical Engineer for the Palo Alto Veterans Administration Rehabilitation Research and Development Center, and Consulting Associate Professor, Stanford School of Medicine, for his assistance in providing the skin-interface pressure system measurement device used in this study. We also thank Sam Seaberg for donating the Sam Splints used in this study.