
Abstract
Objective
To evaluate the Sharpened Romberg Test (SRT) as a measure of ataxia in subjects with mild acute mountain sickness in order to determine its sensitivity and specificity.
Methods
The SRT was performed in 23 subjects during ascent to 5260 m.
Results
The SRT was more often abnormal than the traditional heel-to-toe test, and at the highest altitude it was related to higher median Lake Louise symptom scores with predictive values of 60% sensitivity and 89% specificity. Our evaluation of the SRT appears to agree with similar studies on ataxia showing a lack of correlation between ataxia and symptoms of acute mountain sickness at altitudes below 5260 m.
Conclusion
The SRT was easy to perform and provided a quantitative assessment of truncal ataxia in the field without the need for specialized equipment.
Keywords
Introduction
Objective neurological signs are not usually associated with acute mountain sickness (AMS), but the development of truncal ataxia may be a useful indicator that the benign, self-limiting problem of AMS is developing into the potentially fatal syndrome of high-altitude cerebral edema (HACE).1,2 Ataxia is presently assessed by the Lake Louise scoring system and heel-to-toe tandem walking test. 3 These have replaced the previously used Environmental Systems Questionnaire 4 and the classic Romberg test. 5 The current clinical tests for ataxia are at best only semiquantitative and, in our experience, rarely positive in subjects with moderate to severe AMS.
To study ataxia more accurately, other authors have used static platform posturography and have shown that stability of stance deteriorates significantly at high altitude, 6 but postural ataxia may not be related to other symptoms of AMS. 7 Static platform posturography requires expensive and sensitive equipment that is generally used in experiments in pressure chambers or mountain huts. It may be difficult to use in field experiments and is not practical for ordinary mountain expeditions; therefore, we have been seeking ways of measuring ataxia at altitude more easily. Our initial results with a wobble board 8 showed no relation between ataxia and Lake Louise AMS scores but a possible relation with cerebral oxygenation. However, age was an important determinant in ataxia scores by this method, and the test required several attempts before learning was achieved, thereby making it impractical in the field. 9
Modified versions of the Romberg test have been used in a variety of areas in medicine.10,11 The Sharpened Romberg Test (SRT) 12 is now widely used in the assessment of divers recovering from decompression sickness.13,14 It has been accepted as a useful measure of ataxia because it can be easily quantified and is more sensitive than the standard test. 15 For these reasons, we hypothesized that the SRT might be extended to the assessment of ataxia at altitude. The aims of this study were to evaluate the SRT as a measure of ataxia in subjects with mild AMS and whether such measurements of ataxia related to other features of AMS or to cerebral regional oxygenation.
Methods
Subjects and Study Design
Twenty-three healthy unacclimatized subjects (mean age 40.6 years, range 22–65) were assessed during ascent to 5260 m. Baseline readings were recorded at an altitude of 150 m (Birmingham, UK). The group then traveled by air to 3610 m for days 1 to 5, by bus to 4750 m for days 5 to 8, and by bus again to 5260 m for days 8 to 12 (Bolivia). One subject left the study for nonmedical reasons on day 6. One subject was withdrawn from the study because of HACE developing on day 6. One subject was taking acetazolamide for prophylaxis of AMS, and 3 subjects started acetazolamide on days 6, 8, and 9 because of increasing altitude sickness; otherwise, no other medications were being used for AMS or which would have interfered with balance or the central nervous system. Alcohol was not allowed in the 10 hours preceding testing.
Clinical Assessment of AMS
Self-completed Lake Louise questionnaires 3 were completed each morning and evening. A score of 3 or higher from the questionnaire alone indicated AMS. An additional question on balance was asked with the following scores: 0 = no loss of balance, 1 = mild unsteadiness, 2 = moderate unsteadiness, and 3 = difficulty in standing. Two experienced physicians performed clinical assessment of a standard heel-to-toe test—walking along a straight line 3 m long—on the day after arrival at 3610 m (day 2), on arrival at 4750 m (day 5), on days 6 and 7 at 4750 m, on arrival at 5260 m (day 8), and on day 9 at 5260 m. The assessment of the heel-to-toe test was scored by the clinical assessment method suggested by the Lake Louise consensus, 3 with balancing maneuvers or worse being taken to indicate a positive test.
Sharpened Romberg Test
Each subject stood erect on a level surface wearing flat shoes with his or her feet aligned in a strict tandem heel-to-toe position, arms crossed over the chest, and the open palm of the hand falling on the opposite shoulder. Once stable, the subject closed his or her eyes and attempted to maintain that position for 60 seconds. If the subject failed to maintain the position by movement of either arms or feet or by opening his or her eyes, the time taken to failure was noted. If not achieved, the subject attempted up to 3 further trials of 60 seconds, and a sum of the times was recorded. If the first test was successful, no further testing was required and the subject assumed a score of 240 seconds (60 × 4). If a test of 60 seconds was completed on the second or third trial, all subsequent tests assumed a score of 60.
Tests were performed at 150 m (baseline), on the morning after arrival at 3610 m (day 2), on the next morning at 3610 m (day 3), on the evening of arrival at 4750 m (day 5), on the next morning at 4750 m (day 6), and on the morning after arrival at 5260 m (day 9). All subjects on the expedition volunteered to participate and actively collaborated with the recorder to achieve as good of a result as possible.
Regional Cerebral Oxygenation
Infrared spectroscopy
16
with a Critkon 2020 monitor (Johnson and Johnson Medica LTD, Newport, UK) was used to measure regional cerebral oxygenation (rS
Statistics
The presence or absence of AMS was analyzed by chi-square tests, differences in AMS scores were analyzed by Wilcoxon rank sum test, and rS
Results
Results for the SRT are summarized in Table 1. At baseline, the SRT results were normal (240 seconds) in 22 of the 23 subjects. One subject scored 171 seconds. At 3610 m, 10 of the 23 subjects (43%) had abnormal SRT results, but abnormal results did not relate to the presence or absence of AMS. Mean age was not significantly different in those with abnormal SRT results (48.8 years; SD 13.3) compared with those without ataxia (38.8 years; SD 12.4). On the next morning, 10 subjects had abnormal SRT results, but only 1 of the 23 subjects had AMS. At 4750 m, 5 of the 22 subjects (22.7%) had abnormal SRT results, but none had AMS. On the next morning, 3 of the 22 subjects had abnormal SRT results, but again no relation was with 8 subjects who had AMS.
Number of subjects with abnormal and normal results for the Sharpened Romberg Test (SRT) and the heel-to-toe test (HTT) and with or without acute mountain sickness (AMS)†
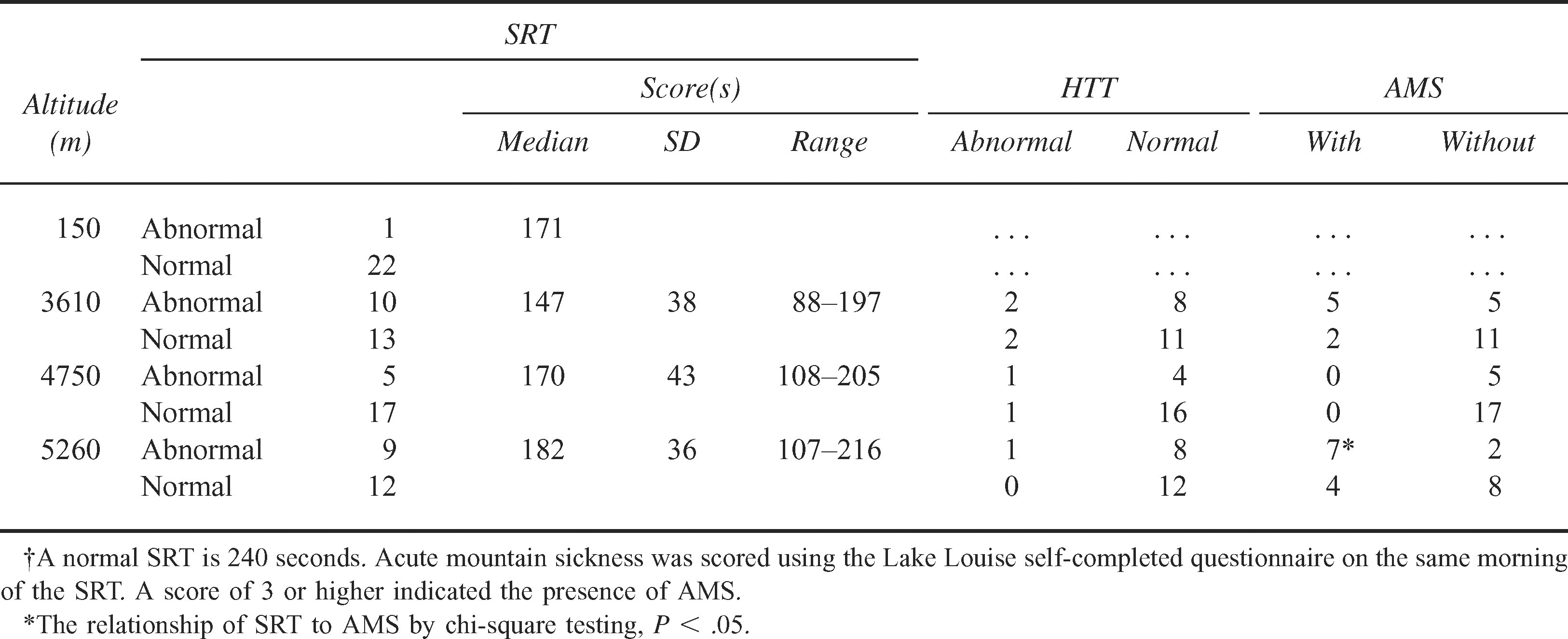
Nine of the 21 subjects (43%) had abnormal SRT results after arrival at 5260 m, and 11 had an AMS score ≥3 (chi-square P < .05). Mean age was not significantly different in those with ataxia (46.4 years; SD 10.4) compared with those without ataxia (40.6 years; SD 14.3, P < .3). The sensitivity of the SRT in predicting AMS was 71% at 3610 m and 60% at 5260 m and specificity increased from 69% to 89% at 5260 m.
Self-Reporting Ataxia
Five subjects on 7 occasions reported loss of balance in the questionnaire completed on the same morning but before the SRT results were measured. On 6 of the 7 occasions, the SRT results were abnormal at the same time. However, the SRT results were abnormal on 31 of the 106 occasions when no ataxia was reported.
Heel-To-Toe Test
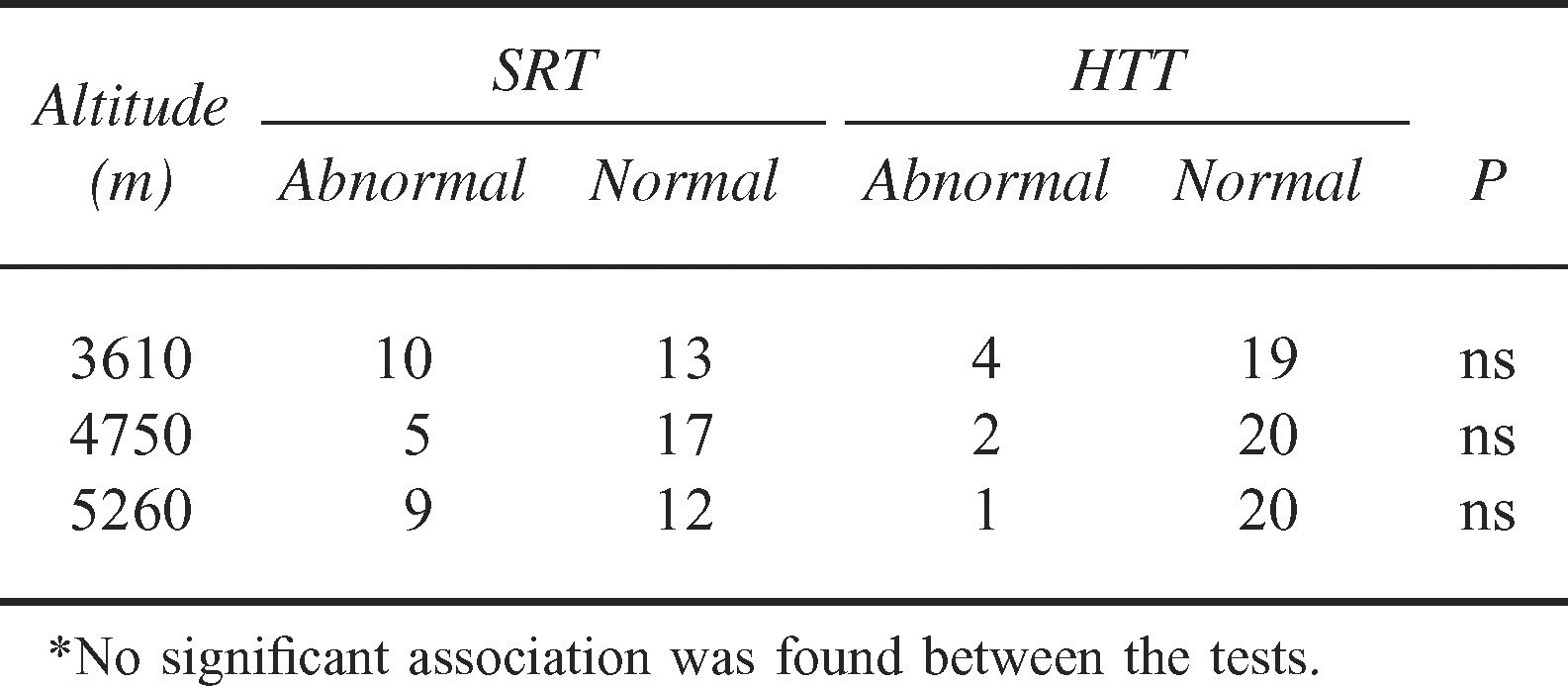
Four of the 23 (17%) tests were abnormal after arrival at 3610 m, 2 of the 22 (9%) were abnormal at 4750 m, and only 1 of 20 (5%) were abnormal at 5260 m (Table 2). Of the 7 occasions when an abnormal heel-to-toe test was recorded, an abnormal SRT result was noted in 4 tests and a normal SRT result was noted in 3 tests, whereas 19 of the 59 (32%) normal heel-to-toe tests were associated with abnormal SRT results. The sensitivity of the heel-to-toe test in predicting the result of the SRT varied between 11% and 20% and the specificity varied between 85% and 100% at the different altitudes. The small number of positive heel-to-toe abnormalities did not allow calculation of the sensitivity and specificity of this test in predicting AMS. However, AMS was present on only 2 of the 7 occasions when a positive heel-to-toe test was recorded.
Number of subjects with abnormal and normal results for the Sharpened Romberg Test (SRT) and the heel-to-toe test (HTT)*
Regional Cerebral Oxygenation
The mean (SD) rS
Discussion
The SRT was easy to perform in the field, requiring only a flat surface in a quiet environment and 1 observer with a watch. The test appeared to have no learning effect, which was confirmed by another study of fit individuals. 14 Our results showed that truncal ataxia was a clinical feature occurring in a significant number of subjects ascending to high altitude. Test scores improved during acclimatization at 3160 m and 4750 m but were not reevaluated at 5260 m. Age did not appear to have a significant effect on the results, unlike our findings of ataxia measured on a wobble board or the findings of other studies that used the SRT.10,12,17
An association with Lake Louise symptoms scores was demonstrated at 5260 m only, though the relatively small number of subjects may have precluded us from assessing this at lower altitudes where the AMS scores were lower. The SRT appeared to be more sensitive than the heel-to-toe test, with over 3 times the number of abnormal readings on days arriving at altitude. Although the self-reporting of ataxia appeared to be highly specific, the large number of positive SRT results in subjects not reporting ataxia would make the questionnaire a very insensitive method of assessment.
The SRT would also have some limitations as a field test in the mountains, with physical elements of the environment, variable mental application of the participant, drugs, alcohol, orthopedic conditions, and possible fatigue all able to influence the ability of the participant to give his or her best test effort. There is also discussion about how long the test should be conducted; therefore, it is not standardized. 13
Analysis of the SRT scores for the 5 subjects who either started acetazolamide for increasing altitude sickness or were developing HACE would have been helpful in showing the SRT's usefulness. However, in 2 subjects, there was no measurement of the SRT in the preceding 12 hours. In 1 subject, the measurement was normal 12 hours before his AMS score changed from 1 to 3. In another subject, the SRT measurement was normal 10 hours before he deteriorated quickly, and he was thought to be developing significant HACE. In another subject, the SRT measurement was abnormal (192 seconds) 17 hours before he was thought to be developing HACE. In all 5 subjects, heel-to-toe testing was normal 12 hours before their illnesses.
Baumgartner et al
7
used a static posturography platform on ascent to 4559 m and reported similar findings to our own, with ataxia occurring at altitude in almost half the subjects, but their results were not associated with AMS assessed by the Environmental Symptoms Questionnaire. Cymerman et al
6
assessed postural instability and AMS during exposure to simulated altitude of 4300 m and failed to show correlation with either the prevalence or the severity of AMS.
6
This is in keeping with our results that showed no connection with AMS scores by the Lake Louise method at equivalent altitudes to the scores of these other studies. However, we did find an association at a higher altitude (5260 m). Baumgartner and Bartsch
18
recorded that, unlike symptoms of AMS, ataxia did not improve with short-term oxygenation. Our findings support their hypothesis that the postural ataxia induced by moderate to high altitude may result from hypoxia affecting specific parts of the brain that are not involved in the pathogenesis of AMS and that these hypoxia-related effects, unlike AMS, need more time for recovery. Our findings on rS
Recovery from ataxia as measured by the SRT was significantly slower than AMS at 3610-m altitude but not at 4650-m altitude with repeated assessment on subsequent days. Further studies on ataxia at altitudes above 5000 m are needed to ascertain whether a relationship exists with other features of AMS and to document the time course of ataxia during acclimatization. For the SRT to be useful for predicting AMS, regular measurements twice daily would appear to be necessary, and even then rapid deterioration may still occur after a normal result. Further studies are required to determine the usefulness of the SRT in the diagnosis of AMS and HACE.
Conclusion
The SRT provided a simple quantitative assessment of truncal ataxia, which could be performed in the field without the need for specialized equipment. An abnormal result was found more commonly in the SRT than in the standard heel-to-toe test and was associated with other symptoms of AMS at 5260 m. The relationship of the SRT to other clinical features of AMS at lower altitudes requires further study.
Footnotes
Funding
The Mount Everest Foundation supported this work.
*
Presented at the 13th International Hypoxia Symposium, Banff, Canada, February 18–22 2003.