
Abstract

The evolution of theory and practice in toxinology and the personalities involved holds as much fascination as the creatures that inflict these potentially mortal injuries. Perhaps the earliest text on snakebite is the papyrus held at the Brooklyn Museum of Art. Dating from Dynasty XXX or the early Ptolemaic Period (305
Through the 19th and early 20th centuries, little advance had been made on the problem of first aid for snakebite. Martin 7 in Sydney and then Fairley 8 at the Walter and Eliza Hall Institute of Medical Research in Melbourne probed the value of ligature use for Australian snake venoms in rabbits, sheep, and goats. Martin highlighted the role of both the lymphatics and the veins in the absorption of various venoms. In the 1940s, Barnes and Trueta 9 in Oxford extended this important concept by demonstrating that lymphatic obstruction or complete limb immobilization prevented the absorption of venom from black tiger snakes and Russell's vipers, but not cobras, in an anesthetized rabbit model.
A Boy Scout in Australia in the 1970s would have been oblivious to this history. He would have been instructed at length about the risks from a venomous elapid snake while out in the bush. Such instruction was appropriate in a region that boasts the 11 most toxic snakes in the world 10 and where contact between humans and snakes is frequent. He may not have been aware that highly refined, equine-derived, life-saving antivenoms, active against all the common Australian elapid snake species, were widely available. What he did know was the importance of correct first aid for snakebite. He would have carried the standard-issue snakebite kit of the time, which contained a rubber tourniquet, a device for wound incision, and some potassium permanganate crystals. What he did not know was that his first-aid management of snakebite was about to be revolutionized by the work of Struan Sutherland (1936–2002) (Figure 1) and his team in the Department of Immunology Research at the Commonwealth Serum Laboratories in Melbourne.

Struan Sutherland demonstrating the pressure-immobilization technique on a volunteer in 1979. © Straun Sutherland. Used with permission.
Sutherland's group was responsible for many of the advances in Australian venom research. With the publication of his landmark paper in Lancet 11 on what has come to be known as the “pressure-immobilization technique or bandage” or eponymously as the “Sutherland wrap,” Sutherland left what is arguably his most important legacy to the field of toxinology in Australia. He appreciated that the conventional teaching of the time—that snakebite should be managed in the field with an arterial tourniquet—was not only impractical but also potentially dangerous. Just as Fontana cautioned, Sutherland knew that few patients would be able to tolerate a ligature for more than a short period of time. In rural Australia, where prehospital transport times were likely to be prolonged, its efficacy was irrelevant because it would have to be removed long before definitive care was reached. In this landmark research, Sutherland combined these practical issues of first-aid care with the pathologist's understanding of the preceding literature that the toxic components of Australian snake venoms are of molecular weights that are preferentially transported by the lymphatics. The impact of the Lancet paper was buttressed by Sutherland’ preparatory pioneering work on venom- and toxin-detection methods 12 and his careful development of a more clinically realistic nonanesthetized primate model. The resulting pressure-immobilization technique was rapidly adopted and has remained the standard of care in the first aid of snakebite victims in Australia.
Although only a few decades old, “Rationalisation of First-Aid Measures for Elapid Snakebite” highlights how much medical writing and the standards that journals demand of their authors have changed over the years. Presented to a current-day reviewer, the paper in its published form could receive many criticisms. At the ethics-committee level, it is likely that Sutherland and colleagues today would have difficulty receiving the necessary approval to conduct such a study on nonanesthetized monkeys, despite monkeys being anatomically similar to humans and that such studies would produce more valid conclusions than would preceding experiments on anesthetized nonprimates. The pressure chosen to replicate that of a firm crepe bandage in the study (see Figure 2) is reported as being based on the subjective assessment of one of the authors. Some of the studies were performed on animals that were anesthetized with open ether, but we are not told how many animals or what depth of anesthesia were used. The use of anesthetized animals further calls into question the applicability of the results to real clinical situations. It is noteworthy that the method evolved during the study, with the initial application of a firm crepe bandage and splint changing to that of a pressure chamber without immobilization in the later experiments. Perhaps the most striking feature is the selective reporting of the results. We are told that 25 monkeys were studied, but we are presented with the results for only 11. The reason for this selective reporting is not stated, with varying reported group sizes for the different treatment modalities studied.
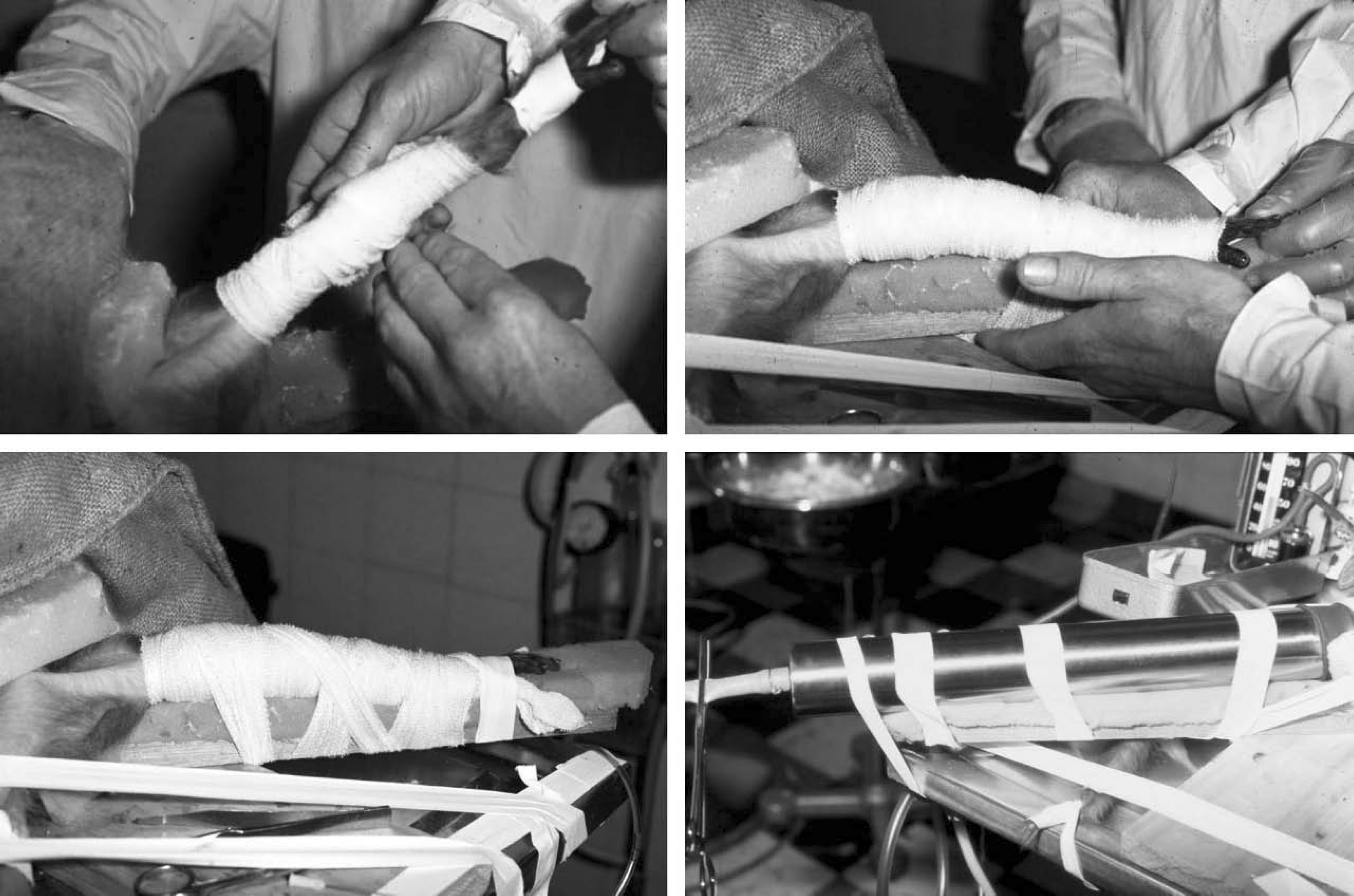
Photographs demonstrating the application of the pressure-immobilization technique to the right leg of an experimentally envenomed macaque in 1979. The final photograph shows the pressure chamber enclosing the affected limb. © Straun Sutherland. Used with permission.
Putting any possible methodological weaknesses aside, the real test of the pressure-immobilization technique is clinical outcomes. Sutherland's own observations give us some clues as to the likely efficacy of this technique in clinical practice. It is important to note that his experiments used a dose of tiger-snake venom estimated to be 6 times the certain lethal dose for monkeys of this weight. As a result of a carefully described technique to mimic the deposition of venom from a real tiger-snake fang, these monkeys would have been expected to die rapidly from a combination of the neuropathic and coagulopathic effects of the venom. Despite this, Sutherland was unable to detect any of the components of tiger-snake venom in the plasma of the fully treated group, suggesting that venom absorption had been retarded to the point of being almost eliminated.
The results that Sutherland observed in his monkeys are in accord with the anecdotal experience of many clinicians involved in the treatment of elapid snakebite in Australia. They will recount instances where a snakebite victim has had initial prompt application of a correctly applied pressure-immobilization bandage in the field and arrived at the hospital completely without symptoms. They will have seen in some patients the rapid development of an envenomation syndrome once pressure immobilization is removed and before antivenom can be given. Anecdote and case series may not seem an adequate level of proof of the efficacy of the pressure-immobilization technique; however, its adoption in Australia was so rapid and complete that to study it in a clinical randomized trial would no longer be feasible or ethical. However, many, if not most, snakebite victims continue to present to medical care without adequate pressure immobilization, 13 for the ‘real world’ value of this technique and its limitations remain the subject of some discussion in Australia. 14 In this context, an important observation from the Lancet paper is often overlooked. Whether considering the control or experimental animals, near-peak venom levels were achieved within 20 minutes either of venom injection or of removal of first aid. Thus, to be most effective, pressure immobilization should be put in place within a few minutes of the bite. At what point this technique becomes completely ineffective remains an open question. An additional and potentially very important question is the possible therapeutic value of this technique.
Several studies suggest that the prolonged use of pressure-immobilization bandaging may have some therapeutic value. Sutherland noted that the monkeys that received this type of first aid for experimental tiger-snake envenomation generally developed a less severe coagulopathy. In addition, subsequent studies revealed that funnel-web spider venom–induced neurotoxicity was abrogated by pressure-immobilization first aid. 15 Building on these observations, Dr John Oakley, 16 an Australian working at Rumginae Hospital in Western Province, Papua New Guinea, recently examined the outcome of patients given prolonged pressure-immobilization technique or bandage after death-adder bites. His retrospective, uncontrolled study suggested that prolonged use of pressure-immobilization technique or bandage, followed by graded cautious release, was effective at managing most cases of death-adder envenomation. Thus, if antivenom is in limited supply, prolonged use of pressure-immobilization first aid may help reduce the severity of the neurotoxicity after death-adder envenomation.
Sutherland's work should lead us to consider the wider role of the pressure-immobilization technique in the field of toxinology. In Australia, the technique is advocated for the management of other envenomations such as those of the funnel-web spider and the blue-ringed octopus, but again the definitive experimental evidence to support this is lacking. More recently, the widely recommended use of pressure immobilization for the management of box-jellyfish envenomation has been called in to question because of concerns that the pressure component may exacerbate nematocyst discharge and thereby worsen rather than improve the patient's state. 17 This debate is ongoing but highlights the need for clinical trials to support the conclusions drawn from laboratory evidence. Sutherland concluded his paper with a suggestion that the technique could potentially be applied to “a wide range of snake venoms and even non-reptilean (e.g., scorpion) venoms.” This remains the greatest challenge of his work. He did perform some preliminary work that suggested a role in non-Australian elapid and crotalid envenomation.18,19 Resistance to this wider application of pressure immobilization has centered on concerns about potentiating local tissue toxicity by trapping venom locally rather than allowing it to circulate centrally. 3 The rationale for this concern initially appears sound when the significant local toxicity of species such as North American crotalids is compared with the limited local effects of most Australian elapids. Perhaps paradoxically, immobilization without pressure remains a routine first-aid recommendation for crotalid bites. 20 The challenge is to study this hypothesis in a suitable animal model in the first instance. The opportunity, should the animal studies show promise, is to study the pressure-immobilization technique prospectively and in a randomized way in populations where its use has not been considered.