
Abstract
Objective
There have been no studies to date exploring the nature of injuries and illness experienced by individuals in a National Park in the southeastern United States. The purpose of this study was to determine the incidence of such illnesses and injuries to visitors in Shenandoah National Park.
Methods
This study was a retrospective review of the case incident reports from Shenandoah National Park from 2003 to 2007. Data obtained included age, sex, time and date report was received, medical symptoms, trauma type, location of injury, mechanism of injury, level of care, time to patient, time to disposition, disposition type, location, and activity at time of event.
Results
There were 159 total cases, corresponding to a reported incident rate of 2.7 persons reported injured or ill per 100 000 visitors to Shenandoah National Park. A total of 23.3% of all reported injuries occurred in persons less than 18 years of age. The most common reported adult injury was soft tissue injury, with the most common anatomical location being the distal lower extremity. The most common activity in which adults were involved at the time of the injury was hiking. Of the pediatric trauma cases, the most common mechanism of injury was a fall. Of the adult medical illnesses, the most common complaint was chest pain.
Conclusions
The pattern of adult and pediatric trauma is consistent among several geographically different National Parks in the United States and represents an injury pattern that all wilderness/outdoor care providers need to be competent to treat. Among adult visitors, the most common medical complaint was chest pain, a complaint more prevalent at Shenandoah National Park compared to other parks. Knowing that trauma injury patterns are relatively similar to those of other parks but that medical illness is more locale specific can help health care providers tailor their resource allotment and health management protocols.
Introduction
As outdoor activities become increasingly utilized as methods of recreation, health care providers will be forced to recognize the unique niche that wilderness medical care occupies in the general patient population. Between 1999 and 2003 an estimated 97.6% of the population 16 years of age or older participated in an outdoor activity of some kind. 1 The number of participants engaged in outdoor recreational pursuits has been increasing. For example, hiking days are projected to more than double in the southern United States by 2050. Backpacking days in the southern United States are expected to increase by 2.31 times and camping by 2.82 times the current rate. 2 As the population of individuals pursuing outdoor activities grows, it will become important for health care providers to understand the nature of injuries experienced by outdoor enthusiasts in their specific area of patient care.
Shenandoah National Park was established in 1935 and encompasses 197 468.76 acres running north to south through central Virginia. There are 516 miles (830 km) of trail and 236 miles (380 km) of road within the park. The Appalachian Trail traverses the Blue Ridge Mountains through the park for 101 miles (163 km). Unique to Shenandoah National Park is Skyline Drive, a paved road that runs 105 miles (169 km) through the length of the park on the top of the Blue Ridge Mountains. Skyline Drive provides access to 79 579 acres of designated wilderness area in Shenandoah. The highest point in the park is Hawksbill Mountain, at 4051 feet (1235 m) in elevation. On average 1 140 000 persons visited the park per year from 2003 through 2007. 3 Access to much of Shenandoah National Park is within 100 miles (161 km) of Washington, DC, and the U.S. News and World Report Hospital Directory returned 11 hospitals within a 50-mile (81-km) radius of Luray, VA, the location of the park headquarters and approximately in the midsection of the park. 4 Shenandoah National Park provides an example of a southeastern National Park that is located in close proximity to a major metropolitan area that has access to numerous emergency care facilities.
Studies5,6 have been performed to investigate the health care issues experienced by Appalachian trail hikers, which comprise a small number of park visitors. However, no studies to date have documented, analyzed, and compared the nature of traumatic injuries and illnesses experienced by participants engaged in outdoor recreation in a southeastern US National Park and requiring National Park ranger, Emergency Medical Services (EMS), or search-and-rescue involvement. The purpose of this study was to determine the incidence of such illnesses and injuries to visitors in Shenandoah National Park. Such data will assist in both improving the allocation of limited resources and in educating not only the public who visit such regions but also the professionals caring for the safety and health of visitors to the National Parks.
Methods
This study is a retrospective analysis of the documented traumatic incidents and medical problems occurring in Shenandoah National Park from 2003 through 2007 that resulted in the compilation of a case incident report file. These reports are completed by a number of different groups, including search-and-rescue personnel, paramedics after activation of the EMS system, and park rangers. The numbers of visitors estimated to be visiting the park were obtained according to an established protocol performed by Shenandoah National Park personnel. This protocol consisted of counting vehicles at park entrance stations and multiplying by a person-per-vehicle modifier that is dependent upon location and time of year. 7 Back country was defined by Shenandoah National Park medical responders as an event occurring on a trail, whether or not care was given on the trail or at a designated medical facility. Front country was defined as occurring along Skyline Drive, in a designated camping area or in one of the lodges (K. Beck-Herzog, written communication, July 2008). All case incident reports between January 1, 2003, and December 31, 2007, were reviewed. Reports were provided by the Shenandoah National Park Public Relations Officer in accordance with the Freedom of Information Act.
Emergency Medical Services reports were first screened by the authors according to 1) inclusion criteria and 2) exclusion criteria. Inclusion criteria included a medical problem or traumatic incident experienced by a visitor pursuing an outdoor recreational activity and resulting in activation of the Shenandoah National Park emergency response system or requiring involvement of Shenandoah National Park emergency response personnel. Outdoor recreational activity was defined as any activity occurring outside for personal enjoyment. All ages and both sexes were included. Exclusion criteria included any illness or injury that occurred indoors or in a vehicle or injury or illness to Shenandoah National Park personnel or staff while engaged in employment activities.
Incident reports were entered into a Microsoft Access database. Medical illnesses and traumatic injuries were analyzed separately, as were pediatric cases and adult cases. Adults were defined as those individuals who were 18 years of age and older. Months were defined based on the standard divisions of the Roman calendar.
Traumatic incidents were analyzed for the following variables: year, month, age, sex, time the call was received, mechanism of injury, nature of injury, location of injury on the body, time to patient contact, time to disposition, disposition type, location in Shenandoah National Park, the activity in which the patient was involved at the time of injury, whether the injury was a back-country or front-country incident, what level of life support the patient required (Basic Life Support vs Advanced Life Support [ALS]), and whether or not the event was fatal. Anatomic locations of injury were subdivided into the following categories: distal lower extremity (foot, ankle, shin, lower leg), proximal lower extremity (knee, thigh), chest, back, distal upper extremity (hand, wrist, and forearm), proximal upper extremity (elbow, upper arm, shoulder), and head (head, neck, and face). Time to disposition was defined as the time from when the call was received by Shenandoah National Park employees to the time the patient was released from Shenandoah National Park employee care. The categories of disposition were defined as follows: transfer to a helicopter; transfer to an ambulance or squad car; and release. “Release” included patients who declined transport (against medical advice) or who were advised to pursue further medical follow-up with transfer by private vehicle after treatment in the field. Distinctions between events requiring Basic Life Support or ALS services were included by Shenandoah National Park personnel on the case incident sheets; the actual ALS service required was not recorded for each individual incident.
The medical variables that were recorded from each case were as follows: year, month, age, sex, presenting complaint, time the call was received, time to patient contact, time to disposition, disposition type (defined in the same way as trauma), location in the park, activity in which the patient was involved, level of support provided (Basic Life Support vs ALS), front-country or back-country status, and whether or not the event involved a fatality.
One of the authors reviewed all of the case reports for exclusion and inclusion criteria to prevent interobserver variation. Both front-country and back-country incident reports were reviewed by one author, and only events determined to have occurred outside were selected.
This study was approved by the institutional review board at the University of Virginia.
Results
There were 159 total incidents: 65 incidents of adult trauma, 29 incidents of pediatric trauma, 57 incidents of adult medical illness, and 8 incidents of pediatric illness that met exclusion and inclusion criteria. There were 24 case reports that did not meet criteria and were not included in the study. A total of 23.3% of all reports documented events occurring in persons less than 18 years of age. There were 11 cases that could not be differentiated as adult or pediatric cases as the result of an unrecorded age on the case report file; these cases were not included in the study. There were 5 810 951 visitors to Shenandoah National Park for this period, with a monthly distribution as outlined in Figure 1. 8 This corresponds to an injury rate of 2.7 persons injured or ill per 100 000 visitors to Shenandoah National Park (1.6 total trauma and 1.1 total medical cases).
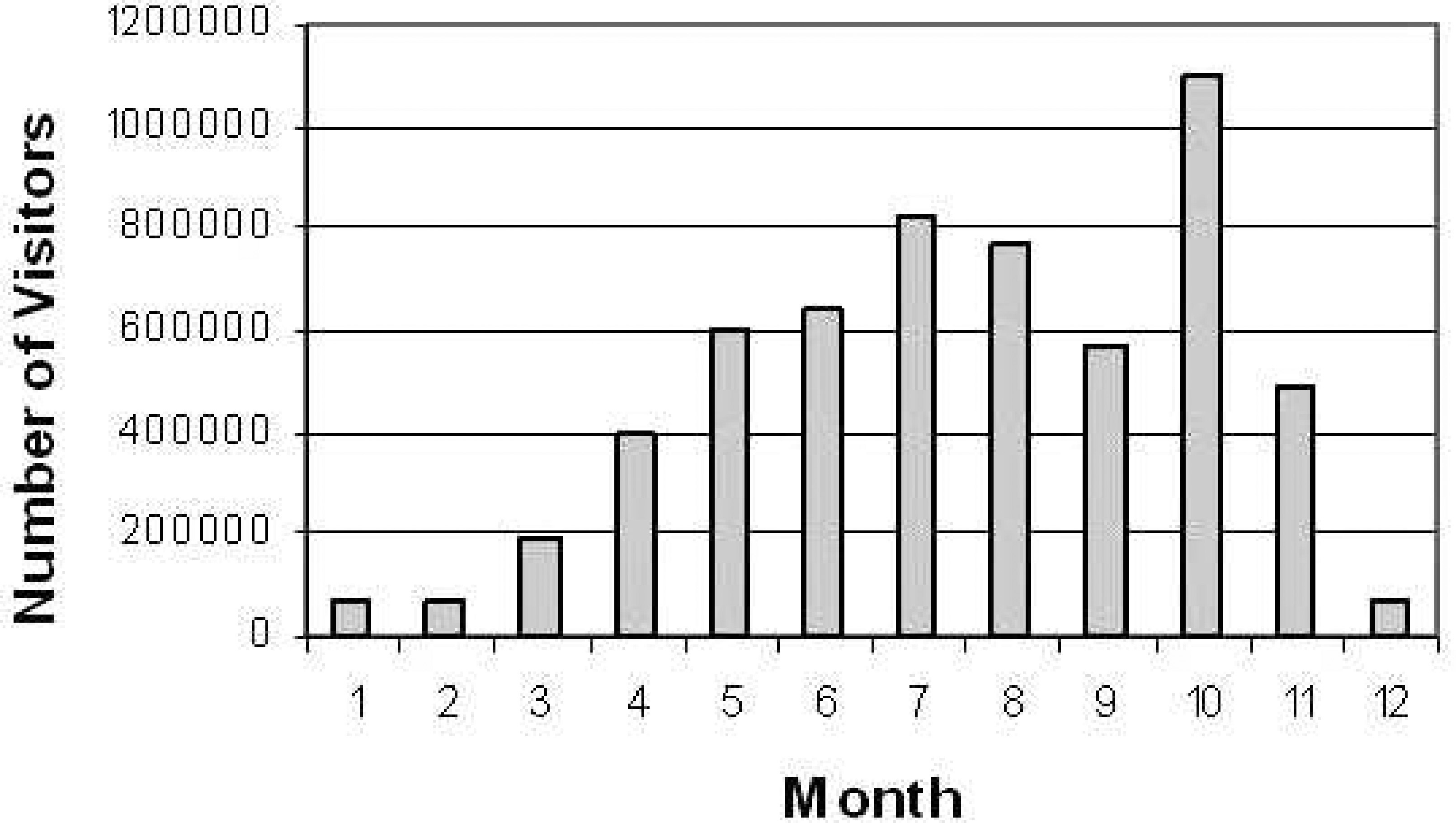
Visitors to Shenandoah National Park by month from 2003 to 2007.
Of the 65 adult trauma cases, 32 involved male patients and 31 involved female patients, with average ages of 38.6 ± 15.3 and 44.5 ± 16.9 years, respectively. For 2 adult trauma victims, sex was not recorded. Adult trauma cases occurred predominantly during May (15.4%), as seen in Figure 2. This peak in trauma cases corresponded closely to the heaviest visitor usage months, as reported by Shenandoah National Park. However, in the usage statistics there was a second peak of visitors in October that was not reflected in the trauma case reports. It is possible that this phenomenon is due to the relative increase of visitors in the park who are in vehicles to view the fall foliage, with a subsequent decrease in outdoor activity as a result of the change in temperature. As seen in Table 1, the most common reported injury due to trauma in adults was soft tissue injury (33.8%). Interestingly, there were 2 reported cases of traumatic injuries incurred from collisions between bicyclists and black bears.
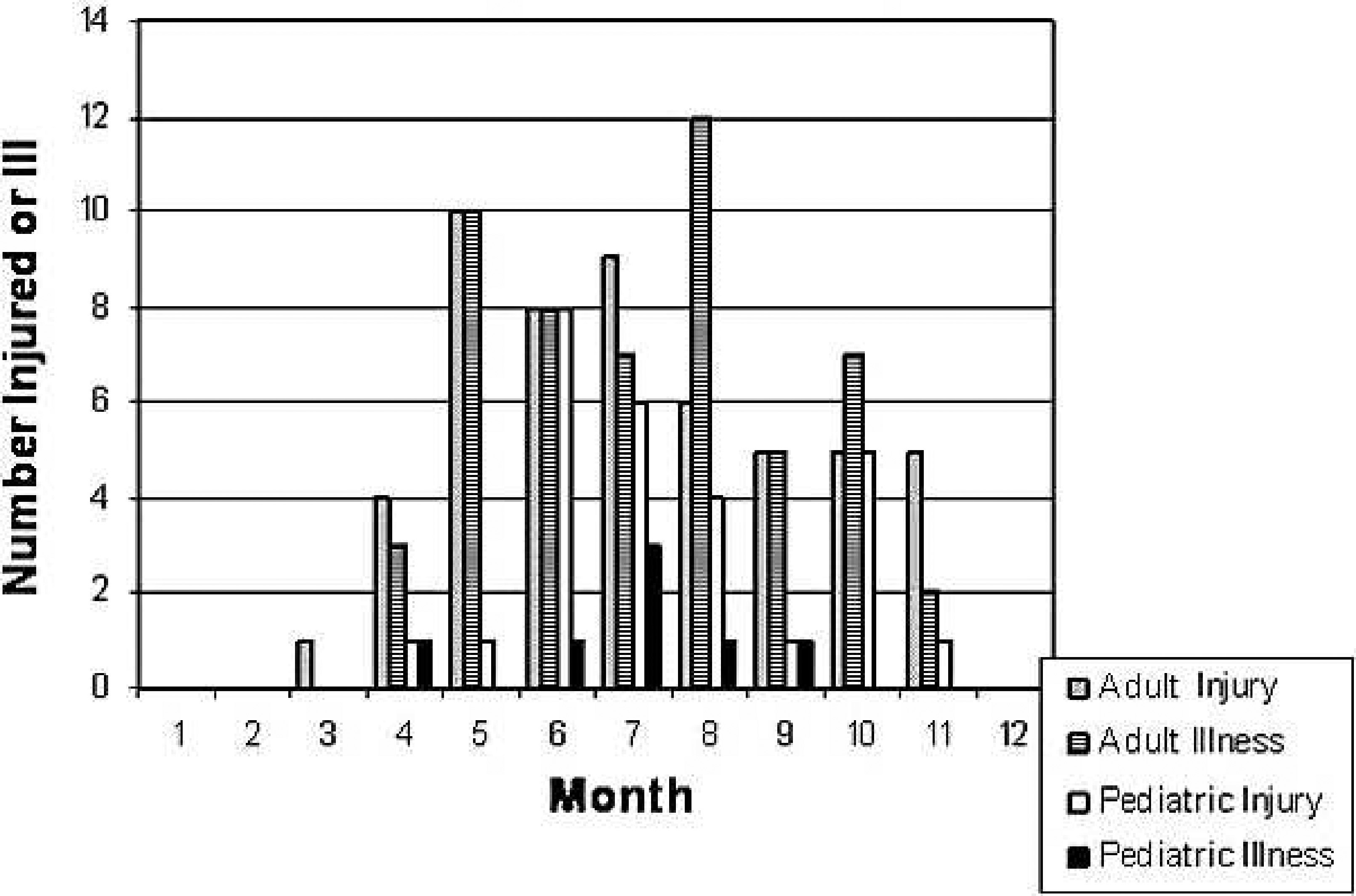
Distribution of adult and pediatric injuries and illness by month.
Type and anatomic location of injury in adults
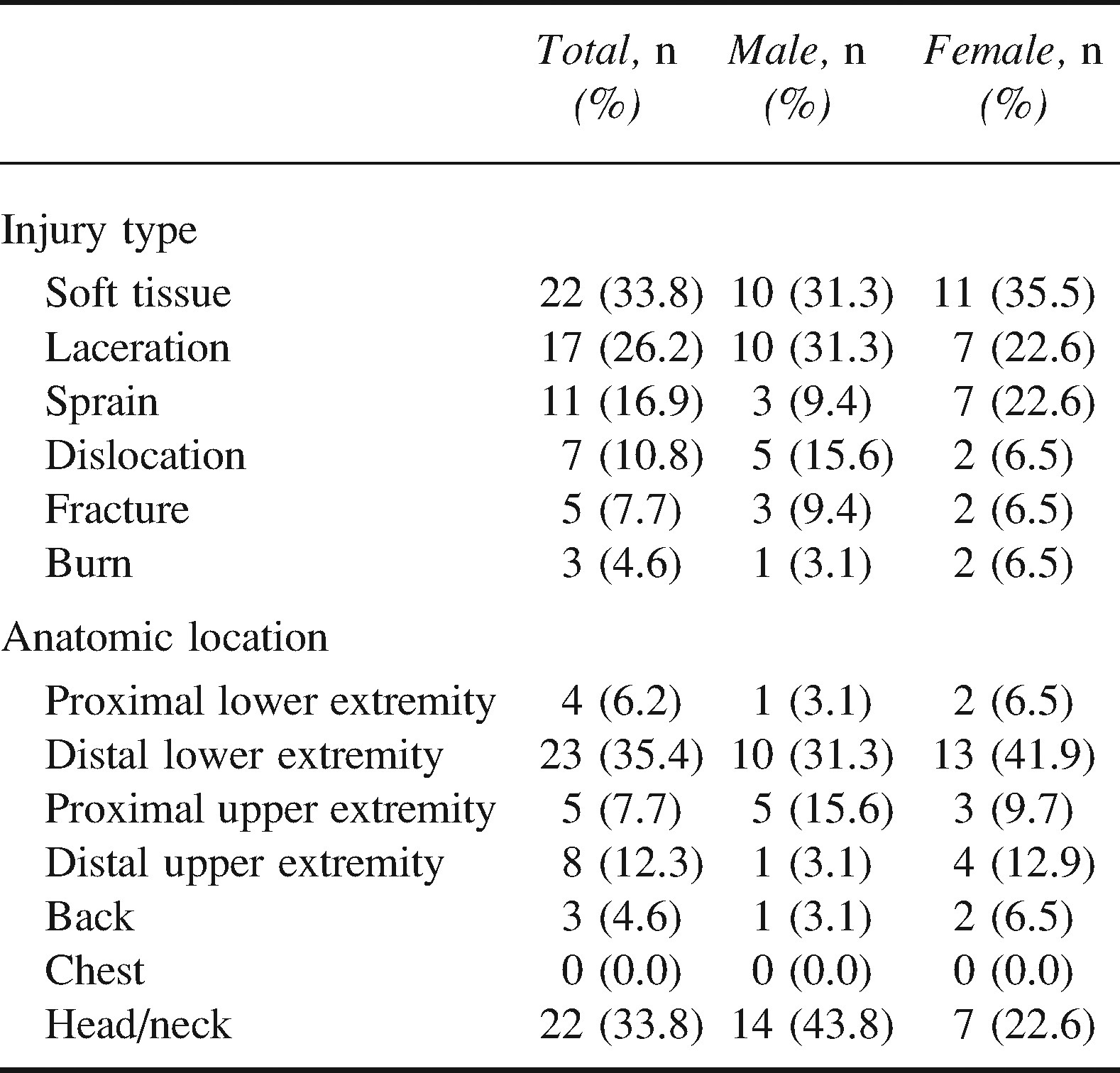
The most common anatomical location of adult traumatic injury was the distal lower extremity (35.4%), as seen in Table 1. Men experienced a greater percentage of the head traumas reported. The most common activities in which adults were involved at the time of the traumatic injury were hiking, biking, and camping (58.5%, 13.8%, and 9.2%, respectively). There were no fatalities from trauma, and 6 patients required ALS.
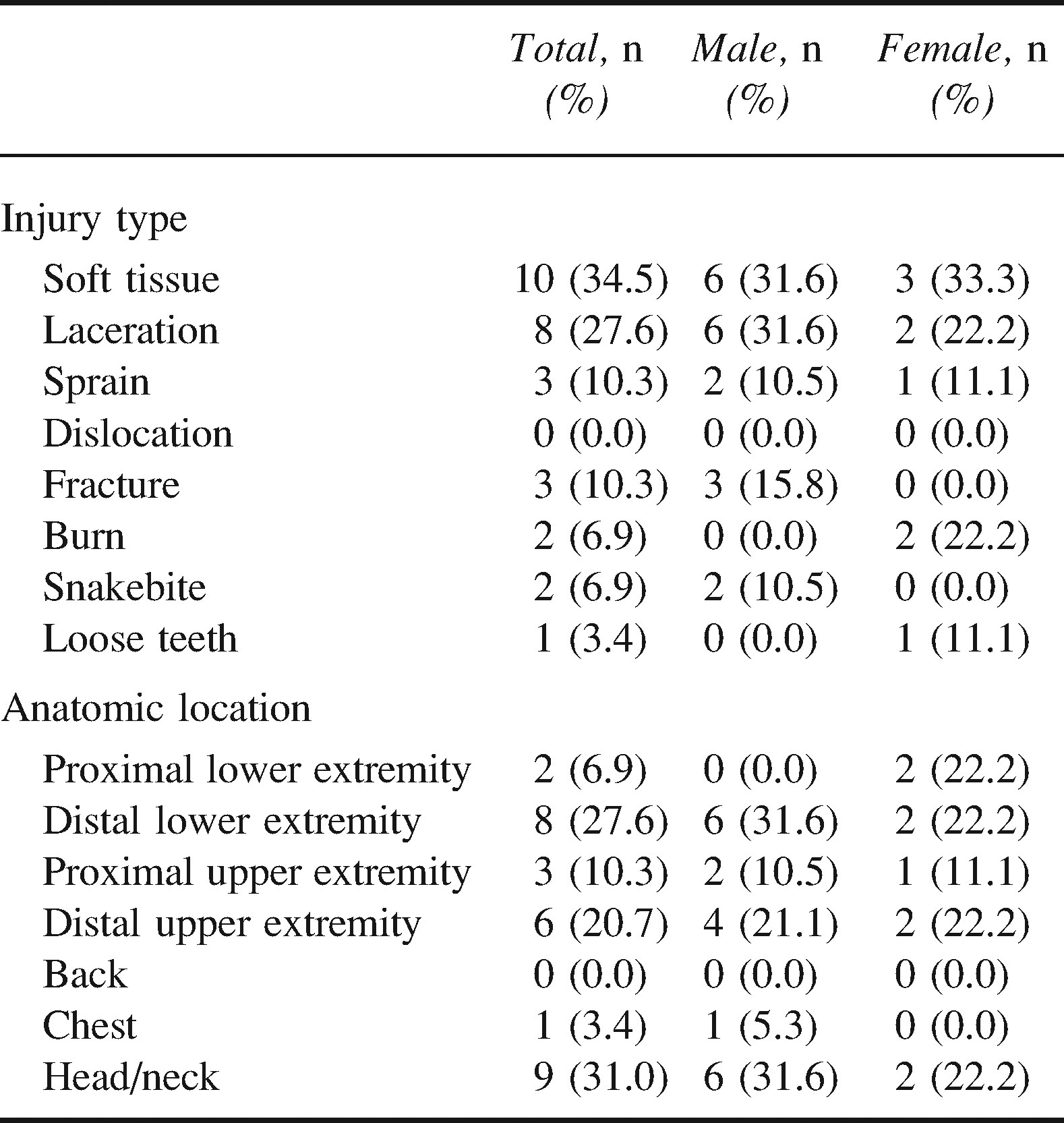
There were 29 pediatric trauma cases: 19 males, 9 females, and 1 for which sex was not recorded. Average age for pediatric male trauma patients was 9.9 ± 4.7 years, and for females, average age was 10 ± 3.8 years. The most common month of injury was June (27.6%), as noted in Figure 2. The most common mechanism of injury was a fall, followed by burns (69.0% and 6.9%, respectively). There were 2 recorded snakebites; the snake species were not recorded. The most common anatomic locations and types of pediatric injuries are found in Table 2. The most common activities in which the injured were involved were hiking, unrecorded activity, camping, and biking (44.8%, 27.6%, 20.7%, and 6.9%, respectively). As seen in Table 3, the most common method of disposition was release to private transportation or leaving against medical advice (72.4%). No pediatric trauma cases required ALS.
Type and anatomic location of injury in pediatrics
Adult and pediatric disposition type: total and percent
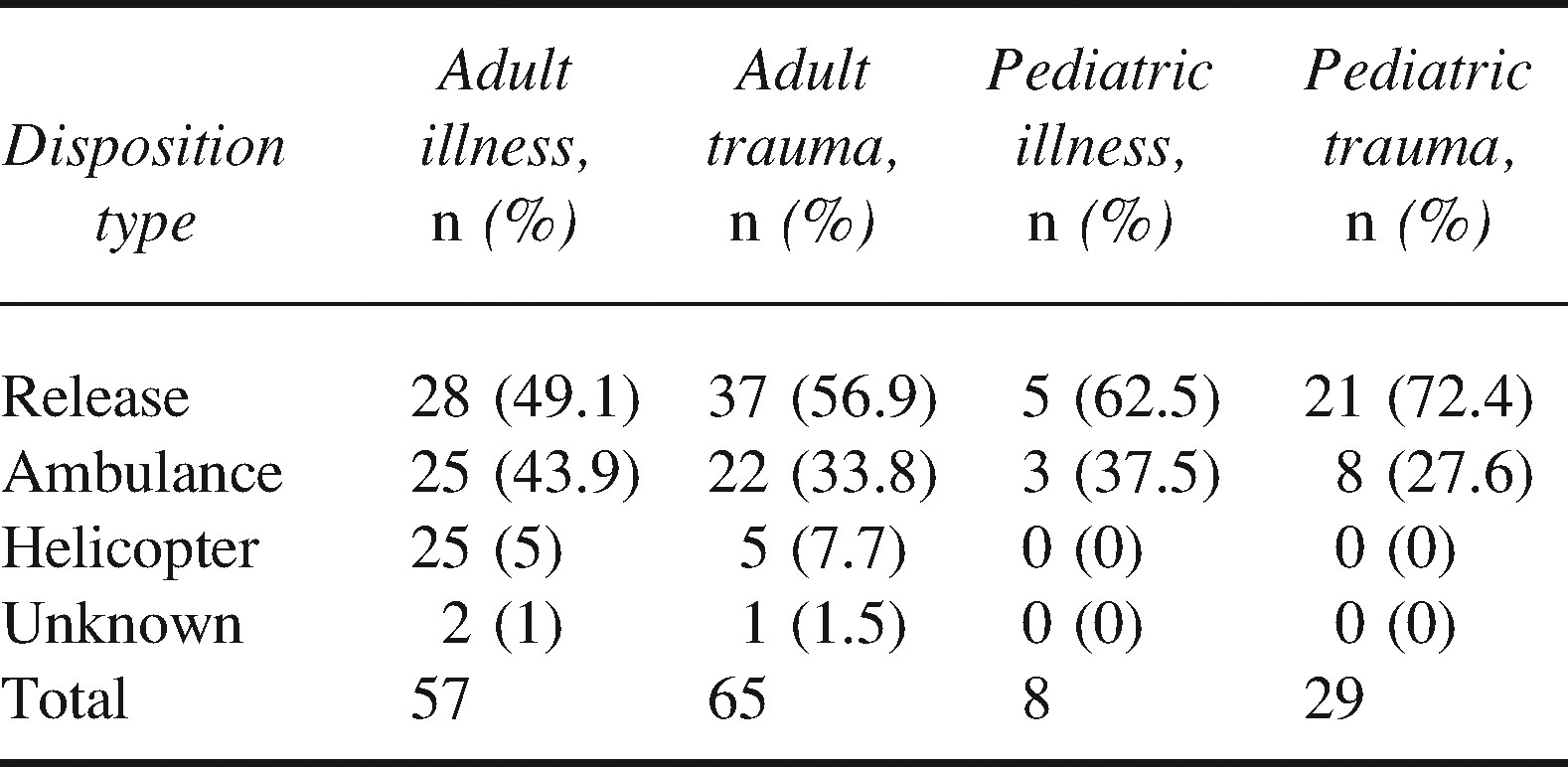
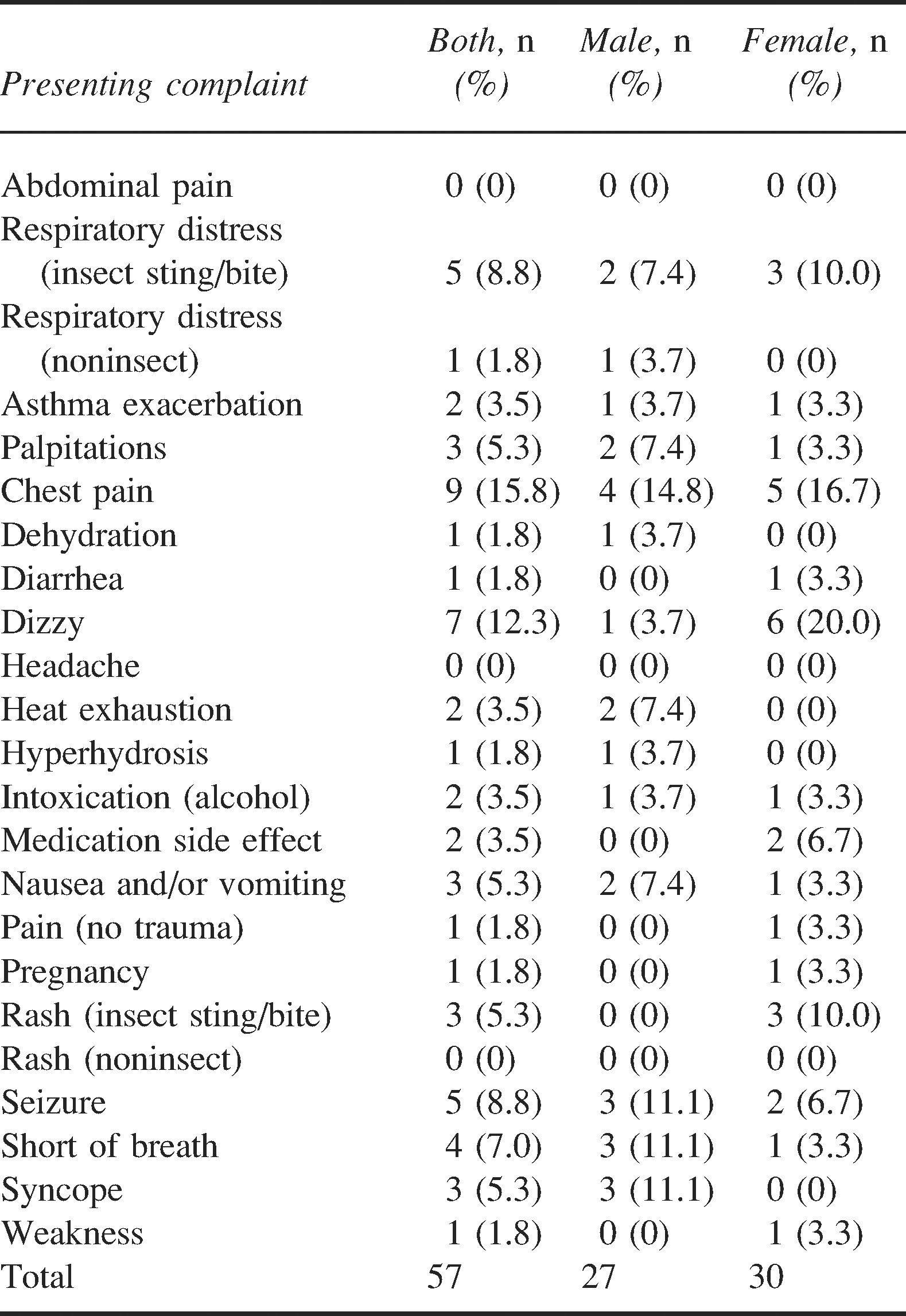
There were 57 adult medical illness cases: 27 male and 30 female, with an average age of 53.4 ± 16.0 and 44.3 ± 20.0 years, respectively. The greatest number of adult medical cases occurred in the month of May (17.5%), as seen in Figure 2. The most common medical complaint among adult visitors was chest pain, as seen in Table 4. Among the insect stings and bites causing either respiratory distress or rash, 5 were described as hymenoptera stings, and 1 was described as a bite from an unidentified large black insect. The remaining incidents were listed as sting/bite from an unidentified insect. The most common activities in which the patients were involved at the time of the onset of the medical issue were hiking, miscellaneous or unspecified activities, and camping (63.2%, 19.3%, and 17.5%, respectively). There were a total of 7 calls requiring ALS. The majority of medical cases were released to ground transport, as seen in Table 3. The only 2 fatalities that met inclusion and exclusion criteria were due to medical problems, one with documented chest pain, and the other victim was found deceased by hikers.
Adult medical illness by gender
There were 8 pediatric medical cases: 4 males and 4 females (average age: 9.5 and 13.3 years, respectively). None of the medical cases required ALS. The most common activity in which patients were involved at the time of the event was camping (n = 5). The list of ailments includes abdominal pain, respiratory distress due to an unrecorded insect sting/bite, dehydration, headache, pain not due to trauma, and rashes (2 due to stings from hymenoptera and one not due to insects).
Discussion
As seen in Table 5, there are fewer injuries or illnesses per person entering Shenandoah National Park than there are for other parks. Exclusion criteria were similar between the studies, with the exception of a study of 7 California National Parks, 9 which did not exclude based on location in the park, and a study in Yellowstone National Park, which did not exclude injury occurring to personnel. 10 As noted by Stephens et al, 11 direct comparisons between illness and injury that have occurred in different parks may be difficult because of differences in inclusion and exclusion criteria and visitation volume calculations. While the inclusion and exclusion criteria in the studies found in Table 5 are not identical, it is not felt that these are significant enough to describe the difference in the quantity of injury and illness between the parks.
National Park study comparisons*

The types of traumatic injury experienced by victims in Shenandoah National Park were similar to those reported in the data obtained from Washington State National Parks and Yellowstone National Park.10,11 The percent of injuries resulting in fracture or dislocation that necessitated the filing of a case incident report were, with the exception of the Yellowstone National Park study, which was based on EMS run sheets, 26%, 18.5%, 8.8%, and 5.5% in Washington State National Parks, Shenandoah National Park, Yellowstone National Park, and the 7 California National Parks, respectively (K. Beck-Herzog, written communication, July 2008).10,11 In Yosemite National Park, fractures represented the most common (20%) reason for a search-and-rescue call. 12 Despite geographical differences between the parks, there are still a significant number of injuries in Shenandoah that result in fractures or dislocations.
The anatomic location of injury in Shenandoah National Park mirrored the distribution of injury found in Sequoia/Kings Canyon. 13 Distal lower extremity injuries were the most common location of trauma in the Washington State National Parks, in the 7 California National Parks, and in Yosemite National Park search-and-rescue missions, as was the case for Shenandoah National Park. One exception was that injuries to the head and neck did not appear to occupy as prominent a role in the western parks. 9 –12 There were no fatal head injuries in Shenandoah National Park during the study period, and 18 (85.7%) of the head or neck injuries were due to falls from standing. The average age was 45.5 ± 15.3 years. While there was a greater number of head injuries in Shenandoah National Park, the majority of these injuries represented minor trauma and could reflect differences in demographic variables, such as age or outdoor activity skill level. Despite the slightly increased prevalence of head injuries, similar types of injured patients appear to compose the majority of injuries that present to park staff or EMS, despite large differences in geographical location. Even in environments with unique geographical characteristics, injury and illness to the lower extremity still comprise the majority of the presenting injuries.14,15
In Shenandoah National Park, a smaller percentage of injured and ill patients required transfer to helicopter than did those in Washington State National Parks (Table 3) (11% vs 38%, respectively). In addition, no children required helicopter evacuation from Shenandoah National Park, while 7% of children in Washington State National Parks required helicopter evacuation. 11 Injuries that occurred in Shenandoah National Park were less likely to require air support, possibly because of the accessibility of much of the park to vehicle transportation and the close proximity of the neighboring hospitals. Other possible reasons for this difference could be that the terrain does not have as many objective hazards as the other parks or that the activities undertaken in Shenandoah National Park are less likely to end in serious injury.
In Shenandoah National Park, the percent of incidents involving persons under the age of 18 years (23.3%) was similar to the percent who presented in Mount Rainer National Park and Olympic National Park (23%). The prevalence of children with injury due to trauma was similar in both parks, with soft tissue injuries and lacerations being the predominate injuries. 11 Again, this emphasizes that despite being very different geographically, patients are experiencing similar injuries in both parks. While there were few medical events reported in individuals under 18 years of age, some trends are apparent. Insect stings/bites accounted for a greater percentage of total medical illnesses resulting in the filing of a case report in children than in adults, a trend noted in Washington State National Parks. 11
Among pediatric victims of traumatic injury, the head and neck and distal lower extremity comprised the vast majority of injuries in male patients, while female pediatric patients had a wider range of injures. This pattern of lower extremity injury among younger participants in outdoor recreational activities has been noted 16 previously among members of National Outdoor Leadership School trips and further illustrates the generalizable nature of presenting injuries.
Of interest is the sex distribution of traumatic events in individuals under the age of 18 years. Males composed the majority of traumatic cases in patients less than 18 years of age (65.5%). This predominance of traumatic injury in young males was also noted in pediatric fatalities in western Washington State and in injuries in Sequoia and Kings Canyon.13,17 This result is in contrast to a study previously published by Twombly and Schussmann, 18 who documented that female students on an Outward Bound course experienced more injuries. However, that study was performed on self-assessments of severity, not health care–provider-documented injury. In addition, the study 18 was performed on participants on a wilderness course, not on the general lay public. While young females on outdoor courses might subjectively experience injury more frequently than men, more young male patients present for acute medical care in Shenandoah National Park, a trend also demonstrated in Washington State National Parks. 11
The most common activity preceding injury or illness was hiking. As previously documented by several authors,9,11,19 hiking has been the most common activity in which patients were engaged at time of injury, and this is an activity that results in distal lower extremity injuries. For the majority of the injuries presenting to park personnel, EMS, or search and rescue in Shenandoah National Park, patients with traumatic injury or illness were participating in similar activities and experiencing similar patterns of injury as victims in other western National Parks.
The presenting complaints of adult medical patients were different among Shenandoah National Park, the 7 California National Parks, and the search-and-rescue victims in Yosemite National Park. Shenandoah patients more commonly presented with symptoms of chest pain, while patients in the California National Parks more typically presented with nonspecified pain without injury (nonchest), shortness of breath, or dizziness. 9 Those in Yosemite National Park presented with dehydration, hypovolemia, and hunger. 12 We hypothesize that this trend reflects the difference in the prevalence of underlying medical conditions, most notably heart disease. Heart disease deaths are much more prevalent in the southeastern United States compared with the western states. 20 The difference could also be exacerbated by the relatively easy access to Shenandoah National Park, thus allowing a greater number of relatively inactive persons access to wilderness areas. Other possible confounding variables are that there are fewer winter activities available to the outdoor enthusiast in Shenandoah and that the altitude of most of the park is lower than the altitudes of many of the western parks. It is interesting to note that seizure was a common presenting problem of male patients in Shenandoah National Park and the 7 California National Parks. 9
This study was limited in several ways. First, there are many access trails into Shenandoah that do not require vehicle access into the park, which could lead to underestimates for total visitors to the park. In addition, as a result of the high hospital density surrounding Shenandoah National Park and the access to Skyline Drive, it is reasonable to believe that many injuries go unreported as a result of self-care and evacuation.
Consequently, as only case incident reports were analyzed, minor events and major events in which private transportation was utilized that did not result in the filing of a case incident report were missed by this study. Second, several reports could not be included in the study because of unclear documentation. Third, the initial categorization of the injuries into types was performed by EMS personnel or rangers at the time of the incident and does not reflect the final clinical diagnosis. However, this method is consistent with that used in similar previous studies. 9 –11 Because this was a retrospective study, no attempt was made to validate the diagnosis presented on the case incident report sheet. Differentiation between soft tissue injury, fracture, and a sprain can be difficult on preliminary examination in the field, so there is likely some overlap in diagnosis between these criteria. Fourth, during the 5-year review period, there were minimal case incident reports regarding pediatric medical illness. If the reviewed time period could have been extended, potentially more information regarding pediatric medical illness in Shenandoah National Park could have been obtained. Finally, Shenandoah National Park does not contain any large areas of water or areas with an altitude over 4051 feet (1235 m), and there is minimal winter sport activity, such as skiing, which might affect the nature of the injuries and illnesses with which patients present.
Conclusions
The most common traumatic injuries necessitating a case incident report occurring in visitors to Shenandoah National Park are lower extremity soft tissue injuries and lacerations incurred while hiking. This pattern of adult trauma has now been found to be consistent among several geographically different National Parks in the United States and represents an injury pattern that all wilderness/outdoor care providers need to be competent to treat. The percentage of trauma victims under the age of 18 years as well as the patterns of traumatic injury that they experienced are similar among geographically distinct parks. In addition, the medical illnesses persons under the age of 18 years experience are similar. However, among adult visitors, the most common medical issue with which participants in outdoor recreation presented in Shenandoah National Park was chest pain. This trend is not consistent among National Parks across the United States and illustrates the importance of recognizing local patterns of illness. In Shenandoah National Park, tailoring care provider training toward acute cardiac events and providing visitors with information about signs of acute cardiac illness could help improve care in an area shown to have a high prevalence of cardiac disease. Knowing that trauma injury patterns are relatively similar but that medical illness is more locale specific can help health care providers tailor their resource allotment and health management protocols to their particular areas of care.
Footnotes
*
No version of this manuscript has been previously published, presented, or submitted for publication in any form.
**
There are no financial interests, direct or indirect, that might have affected this work.