
Abstract
Objective
To determine if an “industry standard” exists for wilderness first aid training and certification of outdoor adventure/education leaders.
Methods
Regulatory authorities, national organizations, and school/college groups were queried with regard to their requirements for first aid training of their wilderness trek leaders.
Results
Only 10 of the 22 states with guide licensure programs required any first aid training as a condition of licensure, and none specified a specific course. Of those programs requiring such training, the requirements ranged from a 6-hour standard first aid course to more structured “wilderness first responder” certification.
Conclusions
There exists no uniform industry standard for first aid training and certification of wilderness leaders. The epidemiology of backcountry injuries as well as what is currently known about clinical skills retention indicate that there may be little evidence basis for much of current practice.
Introduction
With the obvious exception of some “extreme” activities, outdoor adventure travel is one of the safest forms of recreation. Very few peer-reviewed studies have examined the types and frequencies of illnesses and injuries encountered in wilderness travel. The ones that have, however, have stressed the infrequency and minor nature of most events. 1 –4 The bulk of reported injuries consist of minor musculoskeletal trauma and lacerations, the basic management of which is addressed in most first aid courses available to the public. Larger databases of sports-related major injuries and deaths consistently show that wilderness activities such as backpacking are extraordinarily safe in comparison to other athletic activities. 5 –7
In light of this, it is somewhat surprising that there has been a growing interest in the first aid background, qualification, and certification for leaders of such activities. This interest has been marked by a proliferation of courses and certifications directed toward leaders in the outdoor recreation/education industry. This has occurred despite the absence of any evidence basis in the peer-reviewed medical literature with regard to the types of medical competencies required for such activity, or, indeed, with regard to the ability of laypersons to retain such competencies in any meaningful way. Thus, managers of such programs may have difficulty establishing the appropriate training requirements for their personnel.
For ethical, risk management, and liability prevention reasons it would be useful for wilderness programs to understand the current standard of first aid certification for the industry. Since there is no recognized regulatory body with oversight over this activity in the United States, there is no recognized standard. In this setting, an alternative approach is to examine systematically current practice in the industry. The goal of this study, therefore, was to establish what constitutes the contemporary practice for first aid certification of wilderness leaders in organized programs in the United States.
Methods
We identified several segments of the outdoor adventure industry and developed a strategy for approaching each in order to establish their standards.
Regulatory Authorities
In some states, individuals taking clients into the wilderness for compensation are required to hold licensure. We used a strategy that included Internet searches, letters, and personal phone calls to ascertain which of the 50 states had such licensure programs and, for the ones that did, what if any requirements for first aid qualification they mandated.
National Organizations
We identified 4 national organizations that provide oversight to semi-autonomous programs providing outdoor adventure activities: the Boy Scouts of America (BSA), the American Camp Association, the Sierra Club, and the American Canoe Association. Through personal contacts with administration and review of their published standards, we determined the first aid qualifications these bodies require of their participating programs.
School and College Programs
We identified colleges that operate wilderness programs for their own students through the Association for Experiential Education Professional Group. Direct mail or e-mail contacts were made with these programs; we asked these representatives to complete a brief survey instrument addressing their first aid training requirements for out trip leaders. We also queried them as to the way in which costs for this training were handled. The survey instrument is available in the Appendix (available at
Others
Finally, we made direct contact with managers at 3 national providers of outdoor adventure/education: the National Outdoor Leadership School, Outward Bound, and the Wilderness Education Association. For each group, we inquired as to the organization's requirement for first aid training of their leaders.
Results
Regulatory Authorities
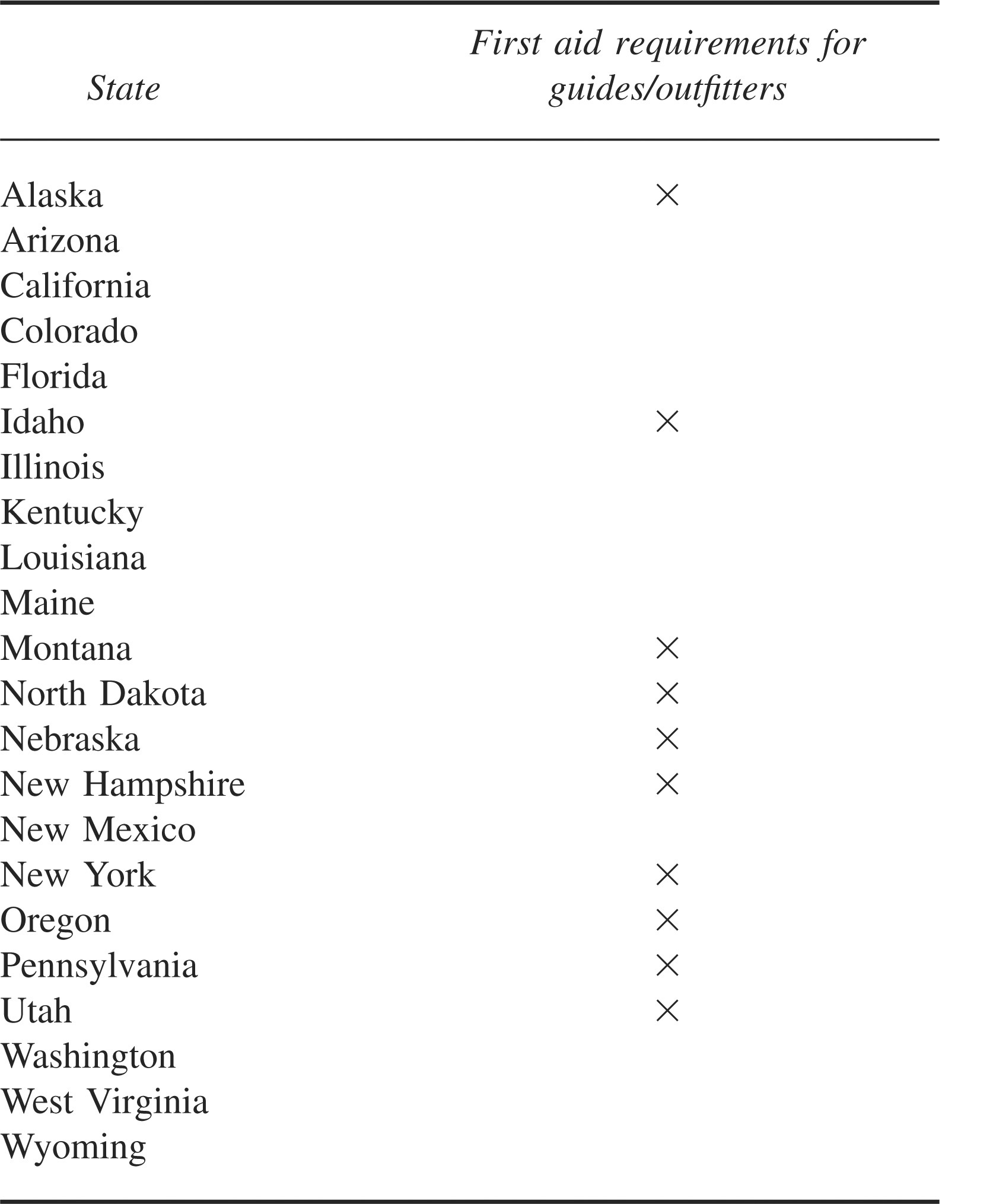
Twenty-two states have programs for licensure of guides or outfitters. Of these, 10 states (45%) require some sort of first aid training as a condition of receiving and maintaining such licensure. None of these 10 states required any specific course (the Table).
States that license guides/outfitters
National Organizations
The national standards for high adventure programs of the BSA require that its trek leaders have first aid and cardiopulmonary resuscitation (CPR) training. At a minimum, an 8-hour course by a “community agency” is required (standard No. 20-120). The BSA further “recommends,” but does not yet require, the American Red Cross's (ARC) Wilderness First Aid Basic course. In 2007, 70 656 youth participated in BSA high adventure treks (F. Reigelman, written communication, 2008).
The American Camp Association's accreditation standard calls for a 16-hour first aid course and CPR certification for leaders of overnight wilderness trips from its camps (standard No. HW-1-C). The Sierra Club's requirements for leaders of outings include completion of the organization's Outings Leader Training as well as first aid certification equivalent to or higher than ARC Basic First Aid. 8 The American Canoe Association, which teaches paddling skills to over 150 000 people annually, recommends “basic first aid and CPR” training for its instructors, but has no formal requirement. 9
School and College Programs
Twenty college programs that offer wilderness experiences for their students responded to the survey. Of these, 19 programs (95%) required some form of first aid training for their trek leaders. Three of the 19 considered the ARC standard first aid course to meet this requirement, while another 8 required a wilderness first aid course—either a local program or the ARC course. Eight of the programs (40% of the total) required wilderness first responder (WFR) certification for their trek leaders.
The survey also addressed costs of such training, which averaged $219 per course for the programs that required it. As a related question, we queried these programs in regard to the driver training they provided trek leaders who transported participants. Only 10 programs required formal training for this activity; training programs ranged from 1 to 6 hours in length.
Others
The National Outdoor Leadership School and Outward Bound require WFR or wilderness emergency medical technician certification for their trek leaders. The Wilderness Education Association also requires WFR certification or its “equivalent” but has not defined precisely what constitutes an “equivalent” certification. None of these programs require that their trip leaders complete any specific WFR course.
Discussion
The simple answer to the question posed in the title of this paper is “No.” Although most of the groups and organizations queried required some type of first aid training for their outdoor leaders, the requirement was clearly not uniform.
It might be argued that the data from state regulatory authorities were most pertinent to the question. Indeed, the existence of a law or regulation mandating a certain type of training would establish the de facto “standard,” at least in the jurisdiction involved. States are the usual governmental bodies establishing such regulations in the United States. Many states do provide oversight and licensure for individuals (guides or outfitters) taking clients into backcountry settings for a fee. Although the 22 states that have licensure for this activity vary considerably in their overall process, none specify any particular type of first aid training for licensure. Indeed, 12 states require no such training at all.
In terms of numbers of participants served, 3 of the organizations queried (American Camp Association, BSA, and the Sierra Club) clearly dwarf other programs. The BSA alone provides wilderness experiences for over 70 000 youth annually. Note that these participants are all minor children, for whom the risk of potential liability for inadequate treatment might reasonably be considered higher than that for adults. This organization, with a major risk management bureaucracy, has no current specification of training requirement and is recommending, in a nonbinding fashion, a program with a 16-hour format. This program (ARC's Wilderness First Aid Basics), however, offers the advantage of a nationally standardized curriculum and certification.
Establishing data from college programs proved the most problematic. These programs vary considerably in their organizational structures, and their leadership changes frequently. Furthermore, there is no central registry for all such programs. Thus, it is likely that such programs were underrepresented in the survey. Nonetheless, they exhibited the same degree of variability in standards that we identified in the rest of the industry.
In light of the fact that motor vehicle accidents are the leading cause of death and disability in college-aged youth, it is noteworthy from a risk management perspective that the training and certification requirements for student leaders to drive participants to trailheads are considerably less intense than those required for them to provide first aid on the trail, where the likelihood of serious illness or injury is remote.
The National Outdoor Leadership School, Outward Bound, and Wilderness Education Association were all more prescriptive in their requirements, each requiring a WFR certification or an ill-defined “equivalent” for their trek leaders. Even this, however, is short of a usable “standard,” given the number of organizations in the United States offering this certification and given the fact that there is no uniform national curriculum or examination for this certification.
If there is no uniform “industry standard” for wilderness first aid training, one might logically ask whether there should be and how it should be determined. Given the epidemiologic data available, one could argue that training in the management of soft-tissue musculoskeletal injuries and lacerations should form the core content of any such program. A casual examination of the content of some of the more popular wilderness first responder courses, however, shows a very broad array of content, offered over a period of several days. Although the precise content of these programs is the proprietary property of the companies offering them, there is a published “recommended minimum” topic list for wilderness first responder courses. 10 This content may significantly exceed that required, for example, for youth sports programs, in which the risk of disabling injury is far greater than that in wilderness activity.
The extent of this content presents some concerns in the context of what the medical education community understands about skills acquisition and retention, currently an area of robust scholarly interest. It should be emphasized that the bulk of wilderness leaders taking first aid courses are not coming from a formal medical background, nor are they regularly working in medical fields. On the other hand, skills taught in the more typical first responder or higher level provider (Department of Transportation–certified) courses are generally being provided to individuals who will be engaged in the emergency medical services industry, either in a paid or volunteer capacity. With this engagement comes a process of continuous exposure to and experience with actual clinical problems; ongoing, real-time medical supervision; and structured continuing education.
Studies that have examined the retention of specific skills by full-time medical providers have shown that even with regular supervision and practice there is a marked erosion in capability. Airway management and resuscitation skills, for example, deteriorate even in nurses regularly working in an intensive care unit. 11 Two years of hospital-based training in an internal medicine residency does not insure adequate airway management skills. 12 Variability among providers exists even in the performance of such basic procedures as measuring blood pressure. 13
If individuals constantly working in a medical environment have a difficult time maintaining proficiency in the skills of medicine, one wonders about the capability of laypersons, who have considerably less training and virtually no opportunity to practice these skills in the real world, and who are without direct supervision when the skills are actually practiced. Although this has not been examined in any structured format, the experience of cardiopulmonary resuscitation is instructive. The American Heart Association recently eliminated the “pulse check” as a component of CPR being performed by laypersons. 14 The rationale for this change was the recognition that laypersons were incapable of performing this most basic of assessment skills with competence. If the American Heart Association, with a nationally developed and standardized curriculum and instructional aids, is unable to train laypersons to obtain a pulse with confidence, one must wonder about the ability of less-structured programs to produce individuals competent to “manage chest trauma,” “manage changes in level of consciousness,” “manage the diabetic patient,” and handle similar events as cataloged in the aforementioned published recommended minimum topics for a WFR course. 10
There has developed a proliferation of training programs in first aid for individuals undertaking leadership roles in outdoor adventure activity and education. This has occurred in the absence of any definitive industry standard requirement. Epidemiologic studies and what is known about clinical skills retention would indicate that there may be little evidence basis for the content of wilderness first aid courses. It may be time for the wilderness medical community to examine the basic premises underlying such courses, with a goal of bringing them into congruence with epidemiology, evidence-based practice, and clinical pedagogy.
Footnotes
Acknowledgments
The authors acknowledge the assistance of the college outing program managers who completed the survey. Ms Barbara Delaney provided invaluable assistance in data collection and manuscript preparation.
Appendix
*
A preliminary version of this material was presented at the 2007 meeting of the Wilderness Education Association in Denver, CO.