
Abstract
Introduction
French Guiana is a French territory in South America covered by 90% of tropical forest. Despite regular first aid standards training, some of the workers in isolated areas remain untrained in common problems they may encounter. We present here the knowledge assessment of these workers concerning first aid and a new training program.
Methods
Thirty-two workers operating in remote areas attended a 1-d training course. The program covered infectious diseases, wildlife envenomation, and first aid and basic life support with a wilderness medicine focus. Questionnaires were issued to assess their knowledge and satisfaction with the course.
Results
The learners were 78% male and of intermediate age (26–55 y). The most common profession was forester (53%). Professionals had been working in remote areas for 12 (4–19) y, and 91% had already received first aid training. The common life-threatening emergencies were not well known; only 6 learners (19%) knew how to recognize a cardiac arrest, 7 (22%) recognized symptoms of severe anaphylaxis, and 23 (72%) performed maneuvers not recommended in cases of upper airway partial obstruction. A total of 26 learners (81%) completed the satisfaction questionnaire. The training met the learners’ expectations. However, 92% would like further training, and 96% requested regular renewal.
Conclusions
This training was the first step toward the creation of a specialized wilderness first aid course. This work supports the need to reinforce training for nonmedical personnel by integrating regionally specific topics. This experience permitted the rise of a working group that proposed a medical kit as well as first aid protocols for workers in isolated areas.
Introduction
French Guiana is an overseas French territory located on the northeast coast of South America. Ninety percent of its surface is covered by tropical forest, difficult to traverse, with a poorly developed road network. Its forests account for 40 to 80% of France's total biodiversity, making them exceptionally rich in flora and fauna. 1 Forests cover almost 80,000 km2 in French Guiana, where more than 1500 species of trees thrive, some of which have only been observed in this territory. The objectives of governmental organizations such as the National Forests Office (ONF), the Biodiversity French Office, and the Guianese Amazonian Park are to conserve, protect, and develop this heritage economically and sustainably 2 (Figure 1).
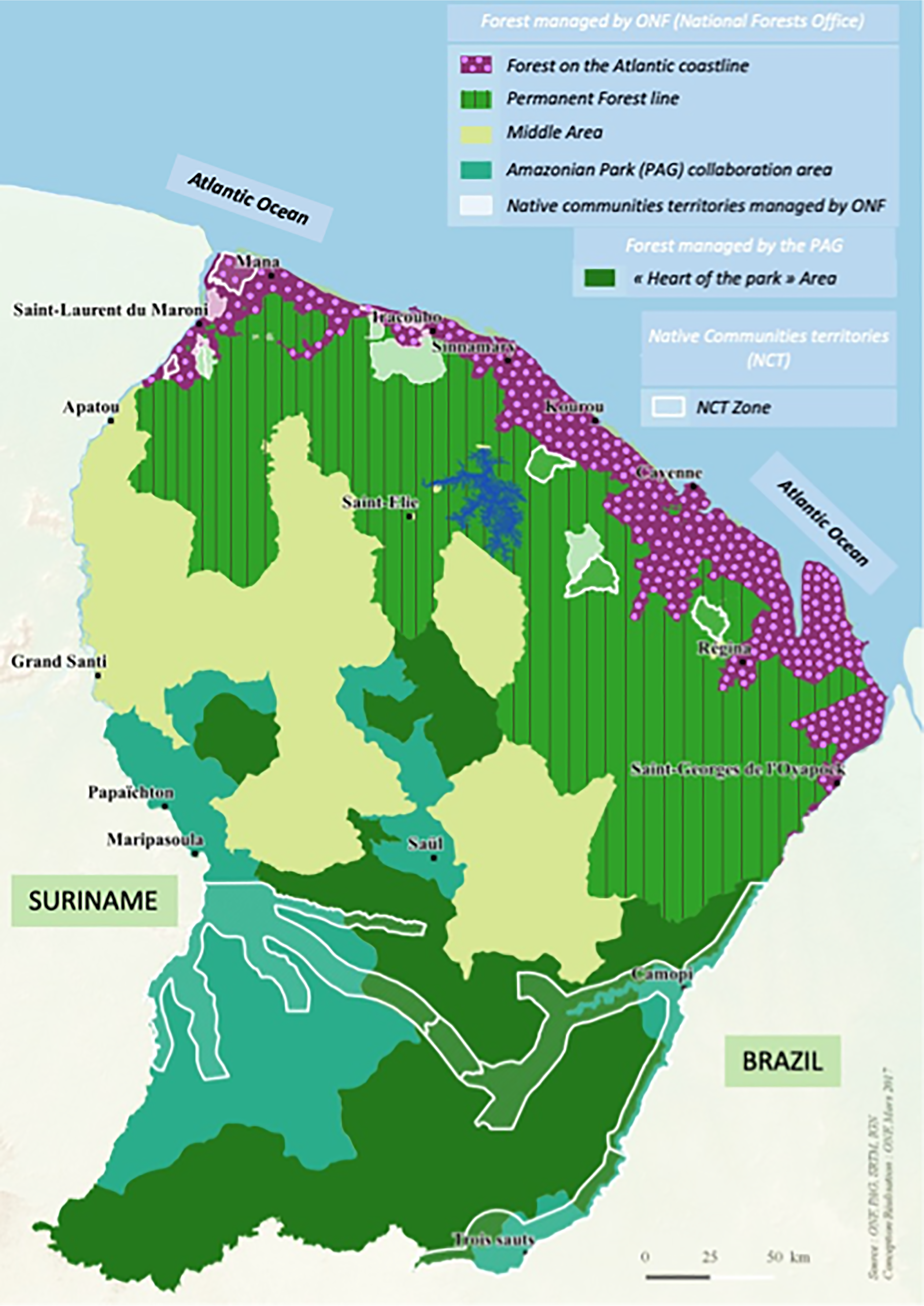
National parks and forests in French Guiana. Source : ONF, PAG, SRTM, IGN, 2017 March.
In this context, many professionals explore remote and isolated areas by walking or riding on quads or in pirogues. Missions and explorations are carried out every day by military personnel, scientists, naturalists, and forestry workers from these various institutions. They work several hours from the nearest hospitals and rescue centers, and their only means of evacuation are by Emergency Medical Services (EMS) or civil protection helicopters based in Cayenne. To comply with the requirements of the French penal, labor, and public health codes, professionals working in these environments are trained in first aid and work-related risks.3–5 Despite regular renewal of this national standards training, some of the emergency situations encountered by French Guianese workers in hostile environments are not covered in this training. 6 Thus, a 1-d training course was organized in collaboration with ONF direction and French Guiana's main hospital, the Centre Hospitalier de Cayenne. The aim of this work was to assess the wilderness first aid knowledge of remote workers and to develop a training course that addresses their specific needs.
Methods
The training, organized by ONF direction at the request of employees, took place over 1 d and was taught by hospital physicians. Thirty-two of the 36 ONF workers in remote areas attended. The morning's program (Table 1) was given by a professor of infectious diseases with experience of numerous scientific missions. It covered the various infections (ie, bacterial, viral, and parasitic) that can be contracted, particularly during extended stays in the forest. This program was adapted from a teaching program that had already been running for several years for young doctors coming to work in the area. In the form of lectures, discussions, and feedback, the 2-h session covered epidemiologic data, preventive and curative measures, and the risks inherent in the many pathogens present in the region. The following 2 h were devoted to wildlife envenomation. A specialized emergency physician presented the different envenomation situations that care providers in French Guiana may encounter, from epidemiology to management and complications. Finally, the third part of the day (3 h) was dedicated to first aid and Basic Life Support. Two doctors from French Guiana Emergency Medical Services and a doctor from the French Military Medical Service, both experienced in missions and forest rescue, explained the emergency procedures that workers in isolated environments may encounter. The real-life experiences of the trainers and trainees covered the various emergency situations: cardiac arrest, respiratory distress, hemorrhage, unconsciousness, wounds, and fractures.
Training program.
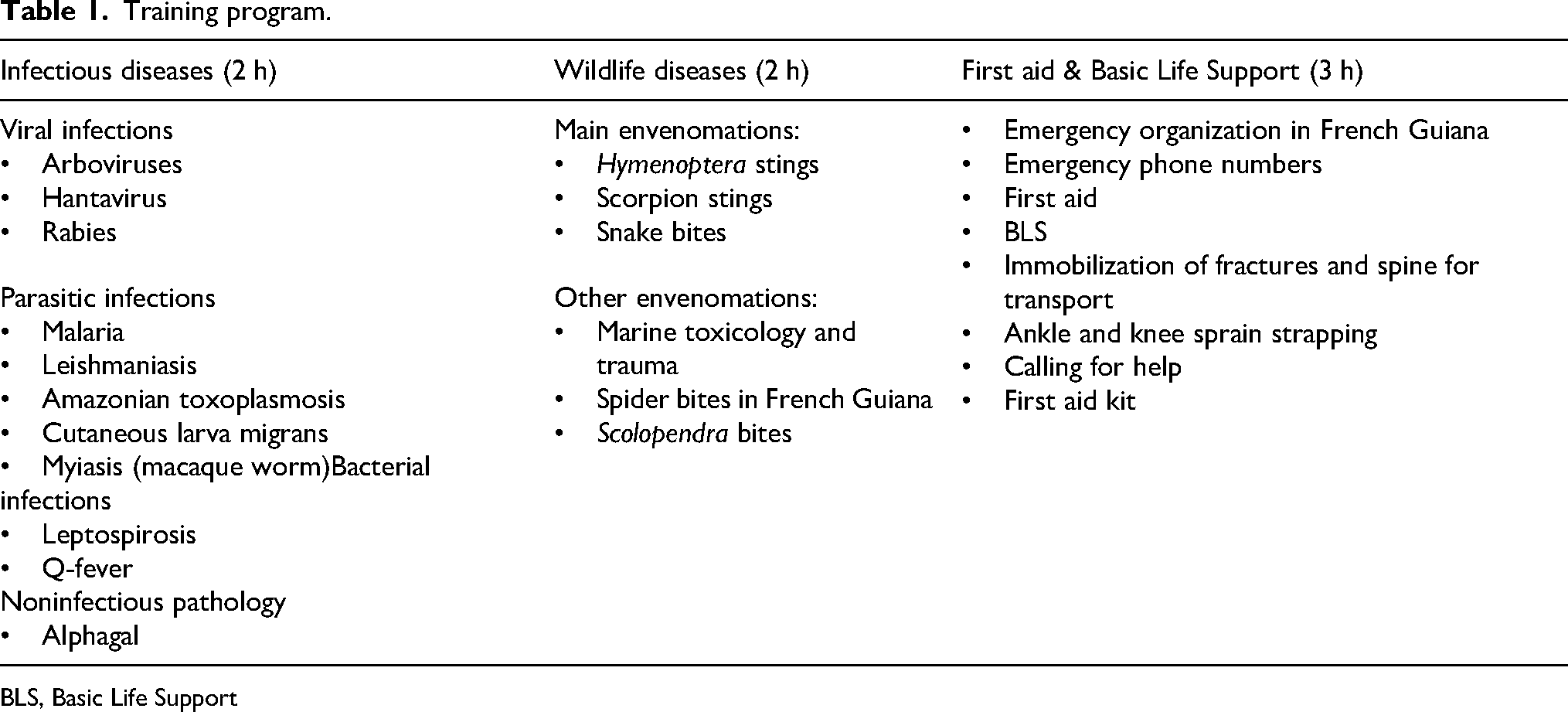
BLS, Basic Life Support
Before the training course, a questionnaire assessing knowledge of professional equipment and first aid was completed by participants (Tables 2 and 3). Trainers used a Google Forms (Google Inc, Mountain View, CA), which allowed live observation of the results and learning adjustments. Indeed, the learning program was prepared but adjusted live to focus on points not well known by the trainees. Subjects mastered were not addressed, whereas others subjects that were less well known or raised questions required more in-depth discussions. At the end of the course, a second questionnaire to evaluate learner satisfaction with the training also was employed (Figure 2). Results of the questionnaire are expressed as headcounts (percentages) for qualitative data and as medians (IQ1–IQ3) for quantitative data. Professionals were questioned anonymously and asked to declare their opposition to the use of their answers. No one objected to the use of their data. Because no personal data were collected, an institutional review board did not have to review the study in accordance with the laws in force in France.
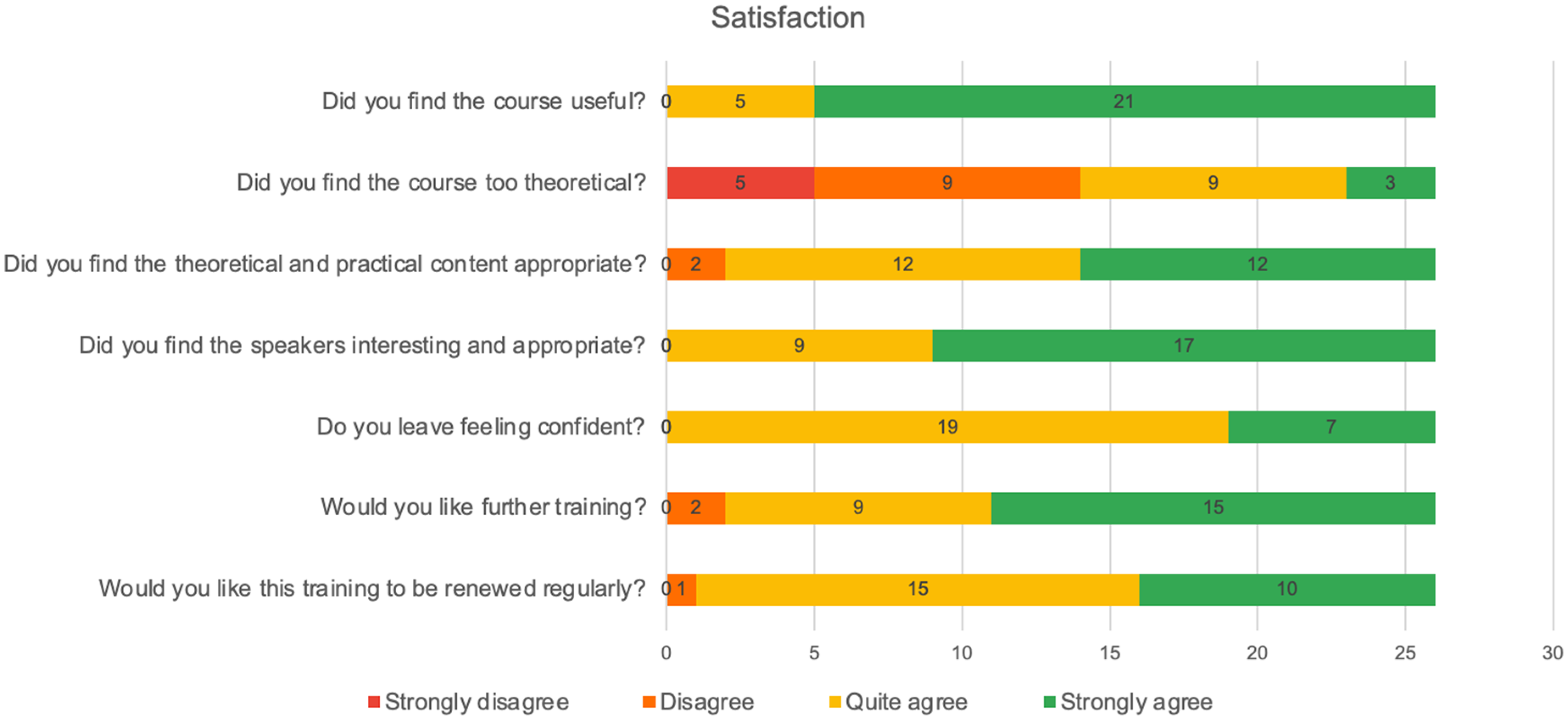
Learners’ training satisfaction (n=26).
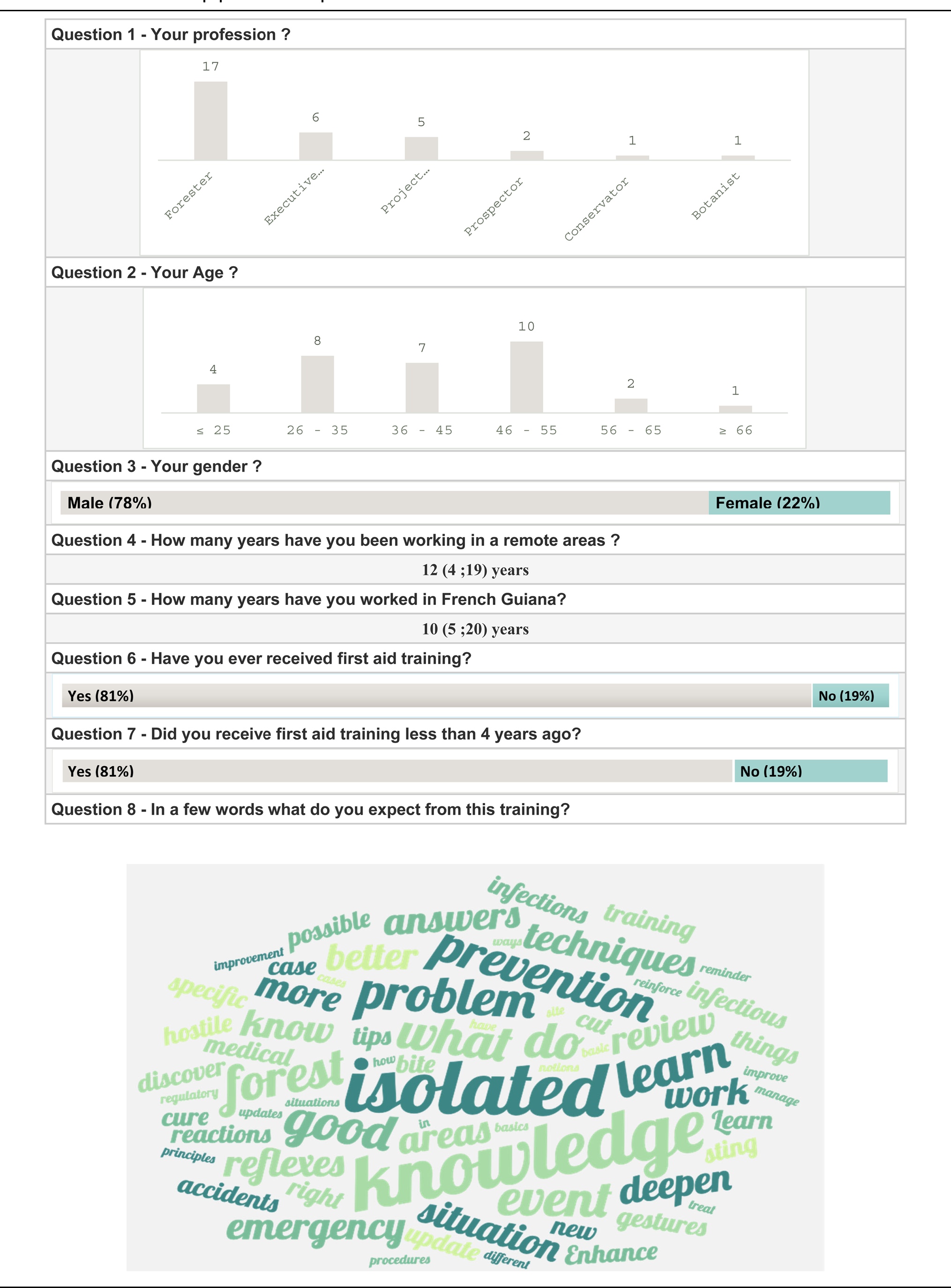
Characteristics, equipment, and expectations of workers.
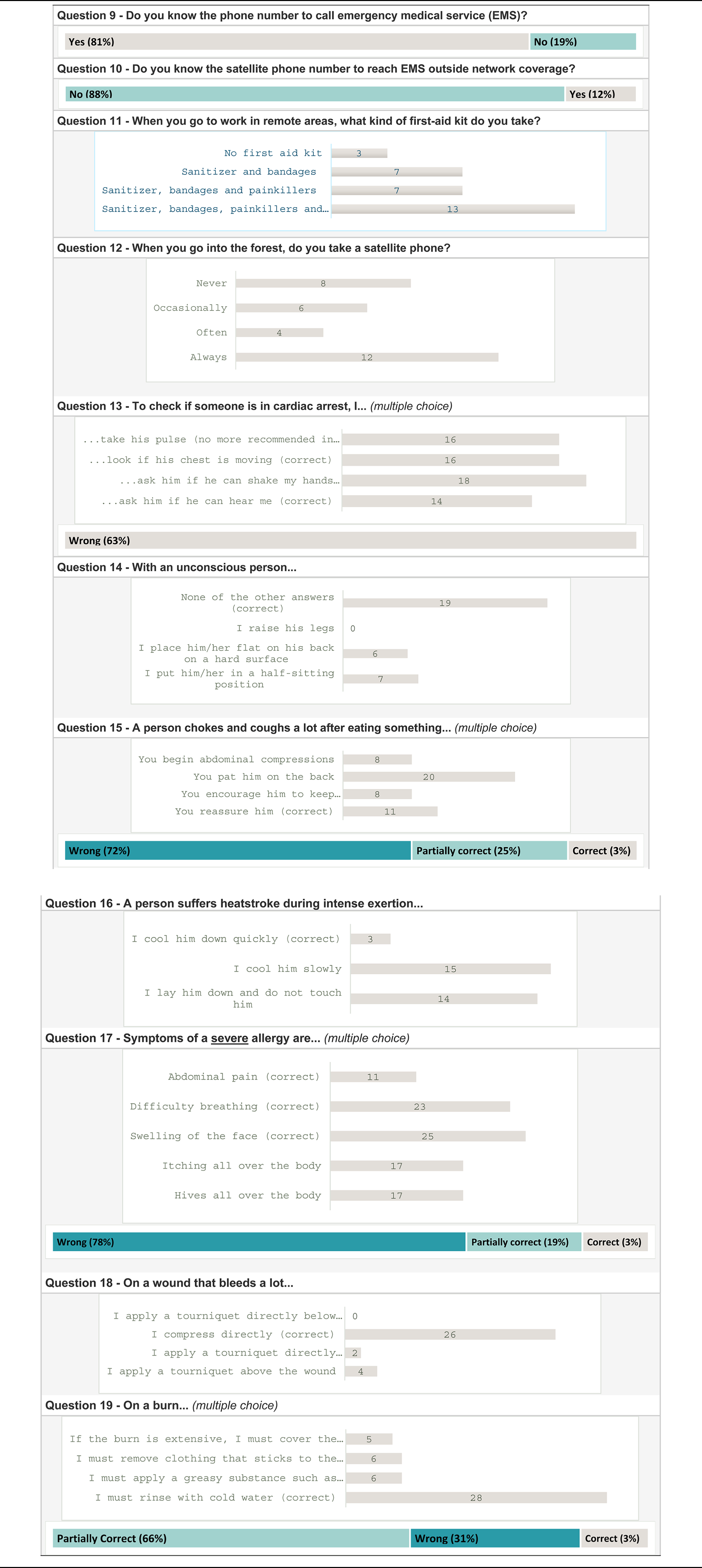
Knowledge assessment deployed before training course.
Results
Thirty-two professionals were present, and 32 questionnaires (100%) were completed at the start of the training. The learners were 78% (n=25) male and mostly of intermediate age (26–55 y of age). The data are presented in Table 2. Socioprofessional categories ranged from those with no secondary education to those with higher education. The most common profession was forester (n=17; 53%). Professionals had been working in French Guiana for 10 (5–20) y and in remote areas for 12 (4–19) y. Twenty-nine of our trainees (91%) had already received first aid training, the majority within the last 4 y (n=26; 81%). Despite regular renewal of this training, we note that knowledge of the common life-threatening emergencies were not mastered: 6 (19%) knew the criteria for recognizing a cardiac arrest, 23 (72%) performed maneuvers not recommended in cases of partial obstruction of the upper airways, 3 (9%) suggested to cool down a heat stroke, and 7 (22%) recognized the symptoms of severe anaphylaxis. Other emergencies seem to be better mastered by the professionals questioned: 19 (59%) knew positions not to use in an unconscious person, 26 (81%) immediately compressed a bleeding wound, and 21 (66%) cooled a burn. Responses to the questionnaire are shown in Table 3. The training provided an opportunity to review the sequences involved in the management of the various life-threatening emergencies: cardiopulmonary arrest, airway obstruction, hemorrhage, burns, heatstroke, and allergy, among others. The Emergency Medical Services hotline was well known (n=26; 81%), but the satellite phone number, mandatory if there is no telephone network, was not known to the learners (n=4; 12%). Given these confusions, the trainers provided information on the organization of care and the resources available. One of the main concerns voiced by the group during the training course was how to prepare an emergency kit. Responses were heterogeneous, but 49% (n=16) regularly or always carried a satellite phone, and 85% (n=27) carried a first aid kit of varying proportions.
At the end of the training course, learner satisfaction was assessed: 26 learners (81%) completed the satisfaction questionnaire. The training appeared to have met the expectations of the professionals trained (Figure 2). However, 24 learners (92%) would like further training, and 25 (96%) requested regular renewal of this training.
Discussion
This study examined the needs and concerns regarding first aid of workers in isolated areas. It also reports on the immediate response provided by a team of experienced teaching doctors. The course was carried out in Cayenne, French Guiana, with professionals working in the heart of the Amazon rainforest. 1 This first training session enabled isolated workers to discuss first aid situations with health professionals. For the most part, these 32 people had received standardized, mandatory, and regular training under French law.3–5 The importance of training the general population in first aid techniques is well established.7,8 However, the “First Aid and Safety at Work” training taught to professionals in accordance with national and international recommendations was not sufficient to enable them to deal with the emergencies they may encounter. 9
Indeed, these standardized training courses, which are designed to meet the training needs of as many people as possible, sometimes produce questionable results in terms of assimilated knowledge and skills.10,11 Our results assessing the knowledge of professionals who were up to date with their training (<4 y) support the observation that recognitions of cardiac arrest and severe anaphylaxis are not mastered, nor are the first steps of management of a partial upper airway obstruction or heat illness. These observations raise a number of questions. The first hypothesis is that the workers’ national training is probably not fully adapted and insufficient for isolated workers. 4 Second is that these training courses are perhaps not adapted to enable sufficient first aid knowledge to be maintained. 11 ONF direction, keen to meet the knowledge needs of its employees, organized this training day managed by teaching doctors. The Amazonian territory of French Guiana, described as a “hostile to humans’ zone” or even a “green hell,” presents numerous specific territorial characteristics in terms of pathologies and care networks. 12 From infectious tropical pathologies (eg, arbovirosis, malaria, leishmaniasis, and bacterial zoonoses) 6 to toxinology (eg, snake bites, 13 scorpion stings, 14 envenomation by killer bees, 15 etc) to more traditional pathologies requiring adaptation to the isolated environment, teachers tried to respond to learners’ concerns.
The course was enthusiastically received by learners, and the results of the satisfaction assessment were good (eg, usefulness, 100%; suitability, 92%; and interest, 100%). Although its organization has some limitations from a purely pedagogic point of view, this training was a first step toward specialized training in first aid and Basic Life Support for professionals working in isolated areas.16,17 However, to support trainees’ desire to supplement and renew this training, and with a view toward updating and maintaining skills, we plan to continue this educational work. 18 It's important to note that the answers to the question about the course being too theoretical were mixed. Future courses will consider integrating more practical workshops and fewer lectures.
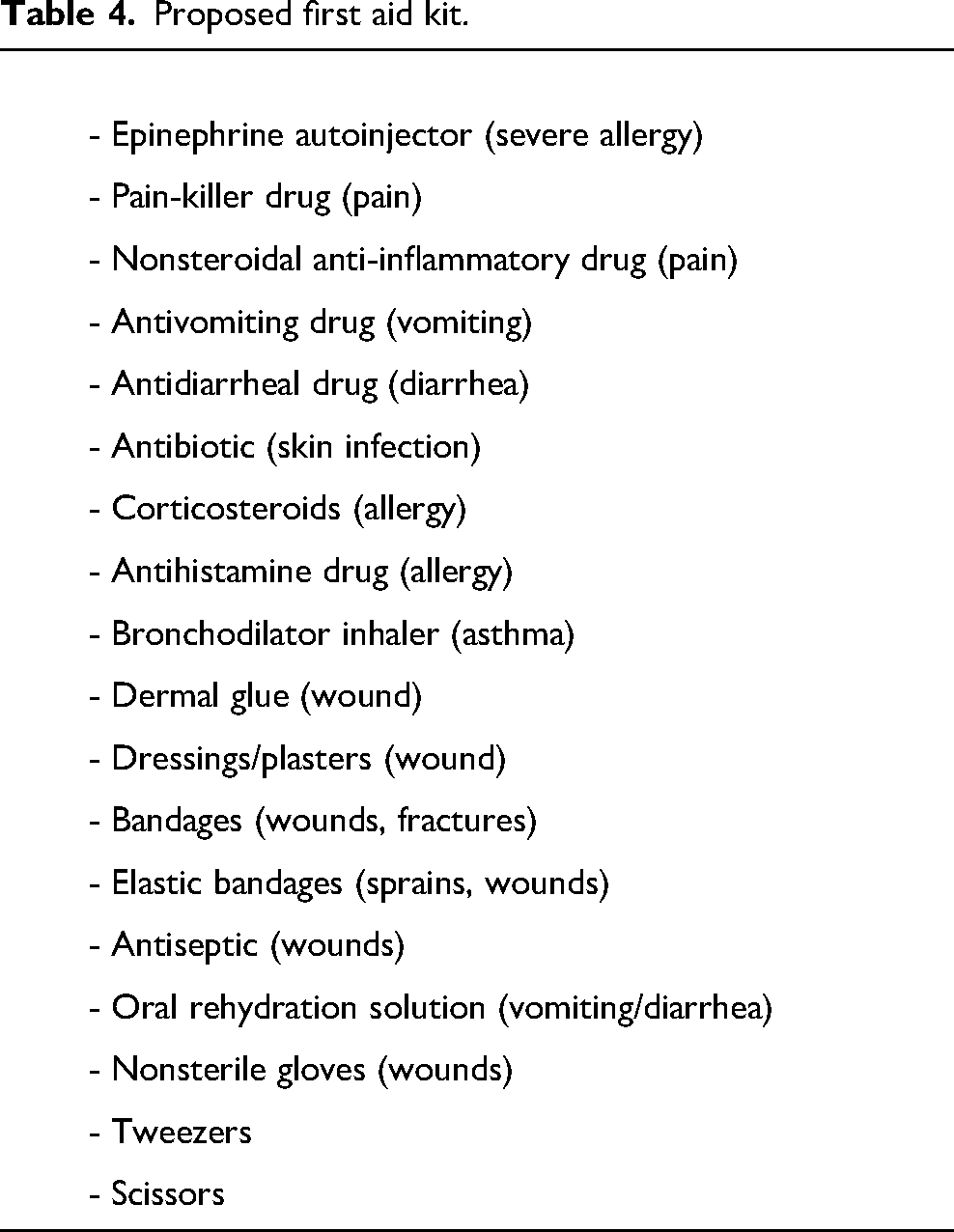
One of the final aspects of this training course was a discussion of the emergency equipment that these professionals can or should use. Legislation varies from country to country, and the mandatory employer's first aid kit in France seems rudimentary for working in isolated Amazonian environments. 4 Most of the professionals surveyed (85%) go on expeditions with a first aid kit, but its composition is highly heterogeneous and completed by each individual regarding their experience in emergency situations, without any control by the employer or consideration by a specialist. With this in mind and following discussions with the professionals, a first aid kit adapted to the needs assessment was proposed (Table 4). Unfortunately, the literature on the subject is sparse; only aeronautical first aid kits have been published extensively, in an environment that differs from the setting of our professionals.19,20 This proposed first aid kit is therefore not supported by any scientific argument but is prepared to respond to the common life-threatening emergencies (eg, cardiac arrest, unconsciousness, airway obstruction, heat illness, etc) that these professionals in isolated environments may encounter. 9 The use and design of this first aid kit will require more assessment. After completion of the course, a working group was organized with the aim of offering this training course to all companies in the region. The objective to prepare an approved first aid kit and a short protocol guide for these professionals will be the fruit of reflection and a literature review.21,22
Proposed first aid kit.
Conclusions
This training was the first step toward the creation of a specialized training of first aid in isolated environments. Other organizations have already approached the team to repeat this type of training. This work supports the need to reinforce training in this field for nonmedical personnel by integrating the specificities of a region that are not covered by international recommendations of training. This experience permitted the rise of a working group that will soon propose a medical kit and first aid protocols for workers in isolated environments as well as for deep-forest scientific stations.
Footnotes
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.