
Abstract
Objective
To determine the prevalence and predictors of injury and illness among long-distance hikers.
Methods
This was a cross-sectional study of long-distance hikers (>500 miles [805 km]) along the Appalachian Trail and Pacific Crest Trails between August and October of 2006. An 8-page survey instrument was made available to hikers at a designated station near the northern terminus of the respective trails. The survey questions were yes/no or multiple choice. Independent variables included packweight, footwear, and type and frequency of water purification. χ2 tests to compare categorical data and the Cochran-Armitage test for trend were used (P < .05 significant). We used logistic regression to compare the variables concurrently, and significance was determined using likelihood ratio tests. Profile likelihood confidence intervals for the odds ratios are reported.
Results
Of the 128 hikers completing surveys that met inclusion criteria, the mean age was 33 years (range = 18–65 years), 94% walked >1500 miles (2400 km), and 70% were male. Using univariate analysis, trends were noted in the proportion of hikers reporting paresthesias and increasing packweight (35% with 10–20 pound [4.5–9 kg] packs, 50% with 21–30 pound [9.5–13.5 kg] packs, and 69% with >31 pound [14 kg] packs [P < .002]), as well as in the proportion of hikers reporting paresthesias and increasing footwear rigidity (29% sandals, 36% running shoes, 42% hiking shoes, and 68% hiking boots [P < .001]). In multivariate analysis compared to sandals, the odds ratio of suffering from paresthesias with running shoes was 1.57 (95% CI 0.3, 12.2), hiking shoes 1.73 (95% CI 0.3, 13.9), and hiking boots 3.9 (95% CI 0.7, 32.1) (P = .16). Compared to 10 to 20 pound (4.5–9 kg) packs, the odds ratios of suffering from paresthesias with 21 to 30 pound (9.5–13.5 kg) packs was 1.5 (95% CI 0.6, 3.9), and for >31 pounds (14 kg) was 2.2 (CI 0.7, 7.1) (P = .03). Adjusting for footwear and pack weight, only pack weight was significantly associated with paresthesias. Packweight and footwear were not significantly associated with other musculoskeletal injuries, such as joint sprains or chronic pain, and muscle injuries.
Conclusions
There is an association between packweight and the prevalence of paresthesias among long-distance hikers. The association between type of footwear and the prevalence of paresthesias is significant when analyzed independently, but loses its significance when the variables are examined together. This suggests that there is confounding between footwear and packweight.
Keywords
Introduction
Hikers along the major long distance trails, particularly the Appalachian Trail (AT) and Pacific Crest Trail (PCT), represent a growing population of wilderness travelers. Statistics from the governing body of the AT show a dramatic increase in the number of hikers on the AT during the last few decades, with 37 in the 1960s, 745 in the 1970s, 1407 in the 1980s, 3272 in the 1990s, and 3997 since 2000. Approximately 1375 hikers started the AT in 2006 with 488 completing the entire trail. 1 Formal data are not available for the PCT; however, approximately 400 hikers started the PCT in 2006 with approximately 90 hikers completing the entire trail (E. Faubert, Pacific Crest Trail Association, oral communication, 2006). With the AT covering more than 2000 miles (3220 km) and the PCT covering more than 2600 miles (4200 km), completing the trails in one season (known as a thru-hike) is a physically and emotionally challenging experience, which is compounded by the lack of access to prompt medical care. Also, because of the distances involved and the necessity to complete the hike during particular seasons (generally April to October), there is little time to recover from injury and/or illness incurred during the hike.
During the last decade there has been a trend toward the use of lighter packs and less rigid footwear, known as ultralight backpacking, as a way of increasing mileage and decreasing injury. Previous studies of long-distance hikers have described types of injuries and illnesses, but have not evaluated the impact of pack weight and footwear on patterns of injuries since this ultralight backpacking trend began. 2 –6 The objective of this pilot study was to examine the prevalence of injury and illness among long-distance hikers and relate that to ultralight backpacking techniques, in particular packweight and type of footwear. Data were also collected on the type and frequency of water purification to see how they relate to wilderness-associated diarrhea (WAD); however, due to study limitations, no meaningful conclusions could be drawn. The data and a brief discussion on WAD are included to assist future investigators.
Methods
This cross-sectional pilot study was performed between August and October 2006 on the AT and PCT. An 8-page survey was compiled and sent to study stations in Glencliff, NH, and Stehekin, WA, which are common resupply points on the respective trails. The survey consisted of multiple choice and yes/no questions with space made available for comments. Distances and packweights were self-reported and presented as multiple-choice questions with ranges, such as <10 pounds, 11 to 20 pounds, etc. These ranges were established based on the first author's (L.S.A.) experience as a thru-hiker on the PCT. Pack weight was surveyed as “base pack weight,” meaning not including food and water. This was done because distances between resupplies and water sources are highly variable and can affect the packweight by as much as 30 pounds (13.5 kg) during the course of a few days. Paresthesias were described as “burning, tingling or numbness in the arms, legs or feet.” A section was made available for hikers to write where on their body they experienced these paresthesias. The survey tool is presented in the Appendix (available at
A volunteer from each community who had regular direct contact with long-distance hikers was recruited to help educate hikers about the purpose and availability of the surveys. Surveys were left in designated places where they could be completed anonymously and voluntarily. Hikers were included if they were at least 18 years old and had walked at least 500 miles (800 km) in the current season, which is the minimum number of miles necessary to apply for a thru-hiker permit on the PCT. The surveys were then sent to Boston Medical Center at the end of the study period, where the data were analyzed. Information regarding the prevalence of a variety of injuries and illnesses suffered during the hike as well as demographics, distance walked, and gear used was collected. Independent variables included pack weight, footwear, and type and frequency of water purification. The χ2 test was used to compare categorical data, and the Cochran-Armitage test was used to evaluate linear trend, using an α level of .05 to determine statistical significance. Logistic regression was used to examine the association between variables significantly associated with paresthesias (P < .05). Significance was determined using likelihood ratio tests, and profile likelihood confidence intervals for the odds ratios are reported. In order to preserve the anonymity of the study respondents, no contact information was obtained, and follow-up was not attempted. This study was given exempt status from the Boston University Institutional Review Board. Data were analyzed using SAS version 9.1 (SAS Institute, Cary, NC).
Results
A total of 143 surveys were completed. Of the completed surveys, 15 were excluded for either hikers being less than 18 years old (n = 2) or having walked fewer than 500 miles (800 km) (n = 13). Of the 128 hikers included, 65 hiked the AT, and 63 hiked the PCT. The mean age was 33 years, with a range of 18 to 65 years. Ninety-four percent of hikers walked more than 1500 miles (2400 km) and 70% were male (see Table 1). The overall prevalence of particular injuries and illnesses is shown in Table 2.
Demographic characteristics (No. = 128)
Prevalence of injury and illness among hikers
The overall prevalence of paresthesias in our study was 48% (60/124). Few participants further delineated where on their body they experienced the paresthesias in the free text section, so localization of paresthesias was not possible. Increasing packweight was associated with increasing prevalence of paresthesias. Among those with “light” packs weighing 10 to 20 pounds (4.5–9 kg), 35% reported paresthesias (95% CI = 22%–50%); among those with “midweight” packs of 21 to 30 pounds (9.5–13.5 kg), 50% reported paresthesias (95% CI = 33%–67%), and among those with “heavy” packs weighing 31 pounds (14 kg) or more, 68% reported paresthesias (95% CI = 50%–87%) (P <.002) (Figure 1). Pack weight was not associated with the prevalence of muscle or tendon injuries, fractures, or acute or chronic joint injuries (Figure 1).
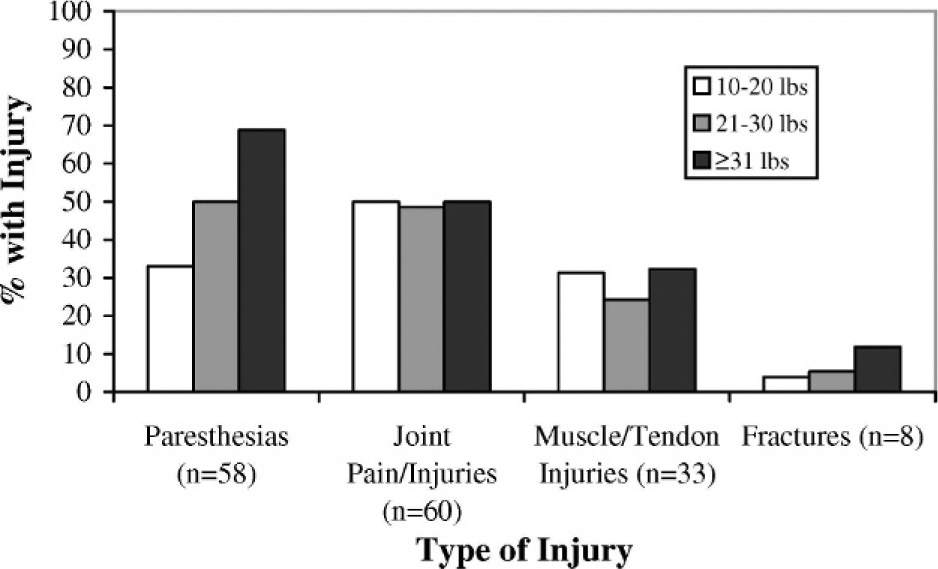
Type of injury by packweight.
In univariate analysis, increasing rigidity of footwear was also associated with increasing prevalence of paresthesias. Among those wearing sandals, 29% reported paresthesias (95% CI = 4%–71%), compared to 36% among those wearing running shoes (95% CI = 22%–51%), 42% among those wearing hiking shoes (95% CI = 23%–63%), and 68% among those wearing hiking boots (95% CI = 50%–87%) (P < .001) (Figure 2). Footwear was not associated with the prevalence of muscle or tendon injuries, fractures, or acute or chronic joint injuries (Figure 2).
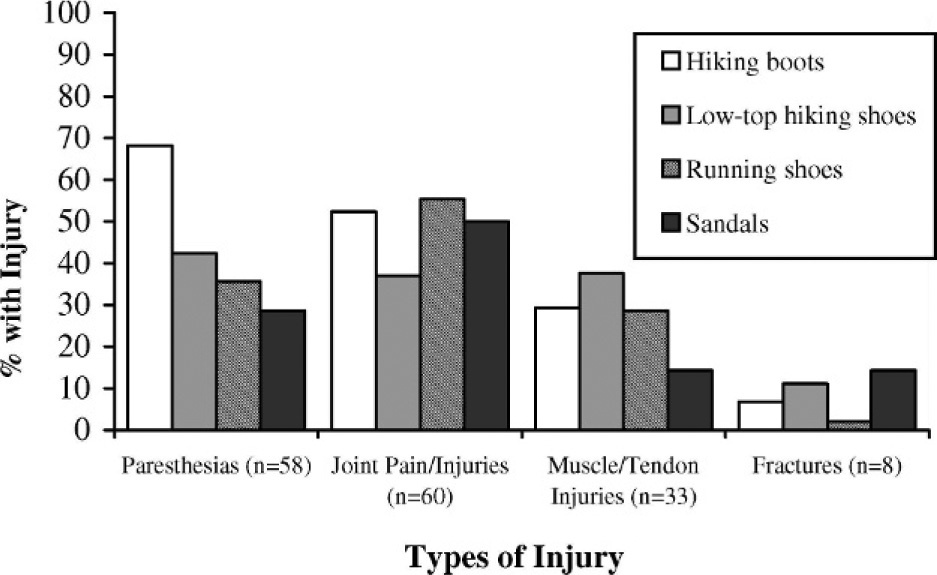
Frequency of injury by type of footwear.
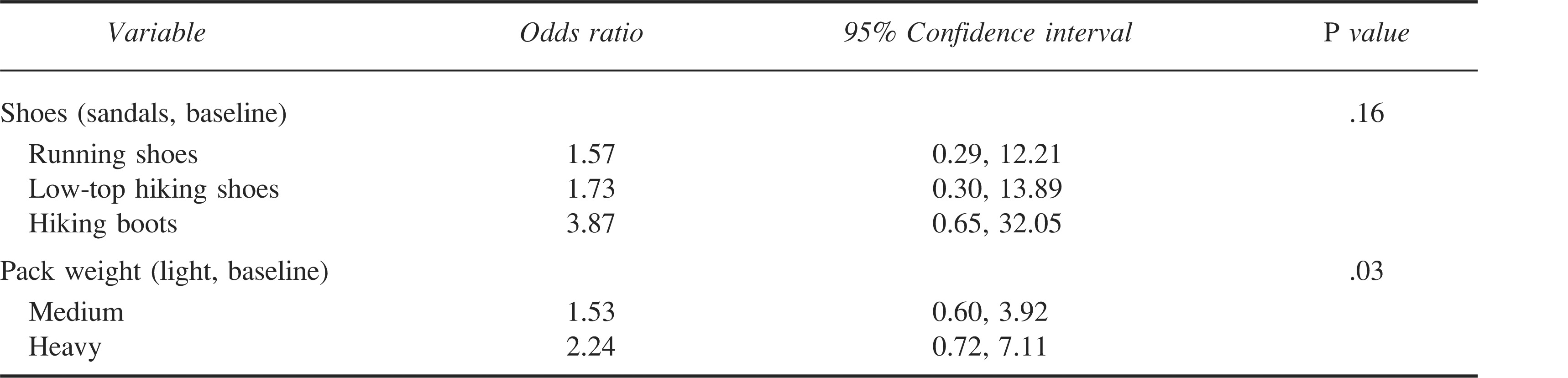
Logistic regression was used to determine the relationship between packweight, type of footwear, and the incidence of paresthesias. Using this model, odds ratios were calculated. Compared to sandals, the odds ratio of suffering from paresthesias with running shoes was 1.57 (CI 0.3, 12.2), hiking shoes 1.73 (CI 0.3, 13.9), and hiking boots 3.9 (CI 0.7, 32.1) (P = .16). Compared to 10 to 20 pound (4.5–9 kg) packs, the odds ratio of suffering from paresthesias with 21 to 30 pounds (9.5–13.5 kg) packs was 1.5 (CI 0.6, 3.9), and for ≥31 pounds (14 kg) was 2.2 (CI 0.7, 7.1) (P = .03). No statistically significant interactions were found between the variables. Table 3 shows the results of the model without an interaction. It is interesting to note that none of the profile likelihood confidence intervals appears to reveal an odds ratio that is significantly different from 1, even though the P value for the variable pack weight was significant. When the model is run with just pack weight the odds ratio between heavy and light packs is significant (odds ratio = 4.03, 95% CI = 1.61, 10.71). It would appear that the study is underpowered to detect these subtle differences between the packweights when adjusting for type of footwear, although it is evident that overall there is a significant relationship between pack weight and paresthesias, with heavier packs being correlated with a greater chance of paresthesias.
Logistic regression analysis of packweight and footwear vs paresthesias
Of note, WAD was a problem for many hikers (overall prevalence of 50%). However, because of the variety of water sources and water purification habits, to name just a few variables, no meaningful conclusions could be made from the data.
Discussion
Musculoskeletal Injuries
During the last 10 years there has been a significant shift in philosophy and type of gear used among long-distance hikers toward lighter pack weights and less substantial footwear as ways of decreasing the work of hiking, enabling longer distances to be covered and fewer injuries suffered. The purpose of our study was to analyze how this ultralight technique affected the prevalence of injury and illness among long-distance hikers. Musculoskeletal injuries represent a significant source of morbidity among long-distance hikers. Paresthesias, which are characterized as a painful burning, tingling, or numb sensation caused by compression and/or repetitive trauma of a peripheral nerve, were the most common musculoskeletal injury suffered by hikers in our study (48%). Various types of paresthesias have been previously described among long-distance hikers: ulnar paresthesias, meralgia paresthetica, tarsal tunnel syndrome, and digitalgia paresthetica. 7
Our study demonstrated a significant decrease in the prevalence of paresthesias associated with lighter pack weights and suggests that less rigid footwear may have an effect as well. In the univariate analysis less rigid footwear was associated with a statistically significant decrease in the prevalence of paresthesias. However, when the effect of packweight was adjusted for logistic regression, footwear type did not have a statistically significant effect on the prevalence of paresthesias. The difference in the findings is due to confounding, because hikers that carry light packs tend to wear less rigid footwear. Our interpretation of these data is that footwear may have an effect on the prevalence of paresthesias, but the results are inconclusive. It is likely that a larger sample size would help to clarify the subtle relationship between type of footwear and paresthesias.
The results regarding the association between packweight and the prevalence of paresthesias, however, are clear. This is in contrast to a study by Boulware in which data were collected in 1997, before ultralight hiking became more commonly accepted. 7 In that study, the overall incidence of paresthesias or numbness was 34% (n = 96) and was significantly higher in younger subjects, those walking >2000 miles (relative risk = 1.3; 95% CI, 1.1–1.6; P = .01) and in women (relative risk = 1.43; 95% CI, 1.05–1.97; P = .03), but no significant associations between the prevalence of paresthesias and pack weight, or paresthesias and the use of running shoes were found. However, the range of pack weights in that study for both controls and those experiencing paresthesias was 16.6 kg (36.5 pounds) to 20.6 kg (45.3 pounds), which is well over our delineation for a “heavy” pack (greater than 14 kg [31 pounds]). Of note, it is not clear whether food and water were included in the estimation of pack weight in that study. Also, there were fewer hikers wearing running shoes in Boulware's study (n = 19 or 6%) compared to our study in which 48 hikers (38%) wore running shoes. The fairly even distribution of hikers between the different pack weight categories and types of footwear in our study supports our hypothesis that hikers are moving toward lighter pack weights and less rigid footwear and gave us an advantage in comparing the prevalence of paresthesias between the groups. An interesting question is that, given that our subjects are overall using lighter packs, why is the prevalence of paresthesias or numbness higher in our study than Boulware's (48% vs 34%)? We feel that the difference involves the difference in the distances hiked between the 2 studies. In our study we included the PCT, which is roughly 2600 miles compared to the AT, which is roughly 2000 miles. Sixty-one of our subjects (49%) reported hiking >2000 miles, whereas the Boulware study involved only the AT. This is supported by the finding of the Boulware study that the prevalence of paresthesias increases with distance hiked (overall paresthesias n = 96 with average 1785 miles hiked vs controls n = 176 with average of 1555 miles hiked). 7 Boulware's study was able to identify the type of paresthesias experienced by hikers, which we were unable to do because it was not further delineated on our survey tool. This information would be very helpful in understanding how pack weight and footwear are impacting the prevalence of paresthesias, and we recommend future researchers make this clear.
Another interesting finding in our study was that rigidity of footwear and packweight were not associated with an increase or decrease in the prevalence of other musculoskeletal injuries (fractures, joint pain/stiffness, muscular/tendon injuries). These findings of decreased paresthesias with lighter packs and lack of other injuries associated with packweight or footwear provide support for the ultralight approach to backcountry travel as a healthier alternative to the traditional “heavy boots and heavy packs” approach.
Gastrointestinal Illnesses
A common source of morbidity among long-distance hikers is WAD. Approximately 50% of our study population reported diarrhea at some point during their thru-hike, which corresponds to the prevalence of WAD in previous studies. 2 –4,8 Unfortunately, our study was not adequately powered to draw any meaningful conclusions regarding how variables such as type and frequency of water purification might have affected the prevalence of WAD in our population. In order to detect a 25% difference in the prevalence of diarrhea based upon water treatment practices stratified by water treatment method (always use water treatment compared to not always use water treatment) with 80% power, we would have needed approximately 640 respondents, necessitating a multiyear study. Also, the variety of water sources that long-distance hikers are exposed to in the course of a single day further complicates any conclusions. Future study of WAD among long-distance hikers could try to evaluate the prevalence of WAD over a specific section of a trail where the water sources are well known. It would be helpful to have hikers keep a log indicating frequency and duration of WAD or to install multiple study stations along the route. Other studies 8 –12 have examined this topic more rigorously and would be useful in guiding further research.
Limitations
There were several limitations to our study based on design and setting that affected the number of participants we were able to recruit and the quality of information we retrieved. The trails are in remote wilderness settings and cover >2000 miles, and other than the voluntary registers at resupply points (at which hikers may or may not stop) there are no ways of knowing how many hikers are on the trail and recruiting them into the study unless a researcher is physically stationed on the trail for several weeks, which time and funding prevented. Even then, recruiting at a single study station (at the northern terminus of each trail) imposes a survival bias, as those who did not make it to the study station, possibly due to injury or illness, were not included in the study. Therefore, the survey results are representative of long-distance hikers that may have sustained injuries and illness, but were able to continue their hike. Also, because the hikers were questioned only one time (at the end of the hike, which generally was about 5 months in duration), our results could be complicated by recall bias, which would most likely underestimate the reporting of injuries and illness. However, considering the dedication of long-distance hikers to walking the trail, it would be expected that survey respondents would have a heightened awareness about their physical conditions. Thus, it is not likely that recall bias had a substantial impact on the results.
Conclusions and future directions
Long-distance hikers represent a unique cohort of wilderness travelers because they endure intense physical exertion through remote, highly varied, and, at times, extreme wilderness environments continuously for months. The desire and need to travel efficiently and safely along this journey have fueled much creativity and experimentation in hiking techniques and gear, resulting in a movement known as ultralight hiking. This is the first study to our knowledge to look at how ultralight hiking affects the prevalence of injury and illness among hikers. It demonstrates that reducing pack weight can decrease the prevalence of paresthesias, without significantly affecting the prevalence of joint pain/stiffness or muscle/tendon injuries. The study also suggests that there is an association between the rigidity of footwear and the prevalence of paresthesias, although further study is needed to clarify this relationship.
Long-distance hikers did prove to be a difficult group to study as described above; however, future researchers might consider a few suggestions: 1) a multiyear study would enable enough subjects to draw meaningful conclusions about significant sources of morbidity, such as WAD, and 2) having multiple study stations along the trail could reduce recall bias and help control for variables such as water sources and changing gear based on the type of environment and weather conditions encountered.
Footnotes
Acknowledgments
We would like to thank Dick and Adele Bingham of Stehekin, WA, and Gary Beale of Glencliff, NH, for their invaluable help distributing the surveys and the research staff at Boston Medical Center for help with the study design and data analysis.
Appendix
*
Previously presented as a poster at the Society of Academic Emergency Medicine Annual Meeting, Chicago, IL, May 16–19, 2007.