
Abstract
Objective
There exist no prospectively generated analyses of the type and frequency of medical incidents in desert settings. We created a database of every illness and injury during 6 field seasons in the Gobi Desert in order to optimize expedition medical and safety planning.
Methods
Every incident presenting to the expeditions’ physicians, regardless of type, magnitude, treatment, or outcome, was recorded. Incidents ranged from headache, insomnia, and diarrhea to lacerations, infection, fights, psychosis, and foreign body extraction and were thus categorized, segregating urban travel-related complaints from illness and injury occurring in the desert setting. The chronology of incidents and illnesses was observed. The incidence of categorized illness and injury was analyzed using descriptive statistics and was presented in terms of person-days in the field.
Results
There were 412 incidents recorded during 2689 person-days from 6 field seasons in the Gobi Desert from 2003 through 2007. The expeditions’ physicians saw an average of 2.2 incidents·d−1 in the urban setting compared to 3.6 incidents·d−1 in the desert. Circadian rhythm disturbances, gastrointestinal illnesses, and musculoskeletal complaints predominated in the urban setting, while minor trauma, heat-related exposures, and gastrointestinal and orthopedic problems predominated in the desert setting. Our data show an absolute risk of illness or injury of 153.2 incidents per 1000 person-days and a risk of “gastrointestinal” and “trauma” complaints of 21.2 and 23.1 per 1000 person-days, respectively.
Conclusions
Herein we describe results from the first ever prospective study of the hazards of travel in an arid environment. We observed that there are patterns of injury and illness that are consistent across expeditions to the Gobi Desert. For example, while heat- and wind-exposure–related illness and injury in the desert are quite common, other aspects of the desert environment are very forgiving. Perhaps the most interesting finding in our cohort was the degree to which different problems occurred at different stages of the expeditions. Our data sets suggest several future studies to evaluate patterns of illness and injury and could be an asset to recreational travelers and religious pilgrims, as well as to those sending employees to extreme environments.
Keywords
Introduction
While much has been written about the hazards of high-altitude environments, exhaustive searches of PubMed (National Library of Medicine) revealed few existing papers on the hazards of desert travel. 1 –3 The specific application of medical research in wilderness settings is relatively new. Research exists for the fields of diving medicine 4 –10 and high altitude, 11 –19 and some excellent textbook references exist, 20 –23 although no one has analyzed the time course during which different types of problems occur during an expedition.
The need for risk assessment and medical planning for these environments is well illustrated by the millions of Muslim pilgrims who each year spend days on foot in the desert 24 while making the Hajj—or pilgrimage to Mecca. In recent years, medical illnesses have included communicable diseases, 24 heart problems, and trauma. 25 Other events warranting consideration include desert expeditions, safari travel, and sporting events such as the Dakar Rally and even the Burning Man in Nevada's Black Rock Desert.
Beginning in 2003 and ending in 2007—as part of our data collection for ongoing studies on the risk of acquiring Rickettsia sibirica during 6 scientific expeditions to Central Asia 26 —we prospectively created a database of complaints brought to the attention of 2 physicians staffing expeditions to the Gobi Desert regions of the Republic of Mongolia and China (Inner Mongolia). The Gobi Desert is located on the border of northern China and southern Mongolia and is a geographically diverse high-altitude desert that encompasses sandy dunes, steppes, and mountains, with temperatures between mid-July to mid-August that historically average 16°C ± 24°C. 27 As such, the weather in the Gobi Desert is highly volatile, and one can experience flash floods, tornados, sandstorms, and thunderstorms.
Data were collected with the intent of optimizing expedition medical and safety planning by noting patterns of injury and illness consistent across expeditions to this arid environment. Preliminary findings were published as suggestions for a medical kit in 2003. 28
Methods
Between 2003 and 2007, every complaint, illness, or injury occurring during 6 expeditions to the Gobi Desert was recorded by the physicians for these expeditions (M.R.L. and I.H.H.). Expeditions were (variously) jointly sponsored by the American Museum of Natural History, the Smithsonian Institution, and the Chinese and Mongolian Academies of Sciences. Expedition members were primarily natives of North America, Latin America, Mongolia, and China. Teams consisted of scientists, students, cooks, drivers, and other support staff, including the expeditions’ physicians. Each expedition lasted between 3 and 6 weeks, with time in transit, and included urban locales such as Beijing and Ulaan Bataar, with the remainder of time spent in the Gobi Desert. There were no medical exclusion criteria. In order to protect patient confidentiality, complaints and the expedition during which the incidents occurred were anonymized.
We elected to count each presentation of a medical issue to the attention of the physician as a separate medical incident (ie, expeditioners with medical problems were logged in each time they came to see the physician, even if they had previously seen the physician for the same problem). We found that conditions for the most part did not require follow up, and we felt that counting each presentation (initial and follow-up) would better demonstrate the impact of conditions on the medical staff and supplies.
We designed a categorical system separating data into organ-system categories that are commonly reflected in the organization of a typical medical kit. Categories and examples are listed in the Table. The value of this system is threefold: 1) it is universally familiar and rapidly accessible to the average medical provider; 2) it is being increasingly incorporated by medical schools for curricular organization 29 –31 ; and 3) it facilitates the process of diagnosis and treatment because it is a framework within which a differential diagnosis and treatment plan are generally conceptualized. Incidents were recorded with date, location, and the number of persons present on the expedition to assess chronology, location significance, and risk, respectively. Institutional review board approval was obtained and maintained throughout the study. 26
Organ-system categorization*†
Results
A total of 412 incidents were recorded during 2689 person-days from 6 expeditions to different parts of the Gobi Desert between 2003 and 2007. There was an increased frequency of medical incidents in the desert setting of 3.6 incidents per day, compared to 2.2 incidents per day in the urban setting.
Differences in incident type and frequency between urban and desert settings were observed (Figure 1). Circadian rhythm disturbances, gastrointestinal illnesses, and orthopedic/musculoskeletal incidents predominated in the urban setting, while minor trauma, exposure, and gastrointestinal and orthopedic/musculoskeletal problems predominated in the desert setting (Figure 2). In the urban setting, circadian rhythm disturbances composed 36% of all medical complaints and decreased to 5% in the desert setting. Trauma and dermatological and psychological complaints all more than doubled from the urban to the desert setting, composing 16.8%, 3.5%, and 3.5% of all complaints, respectively.
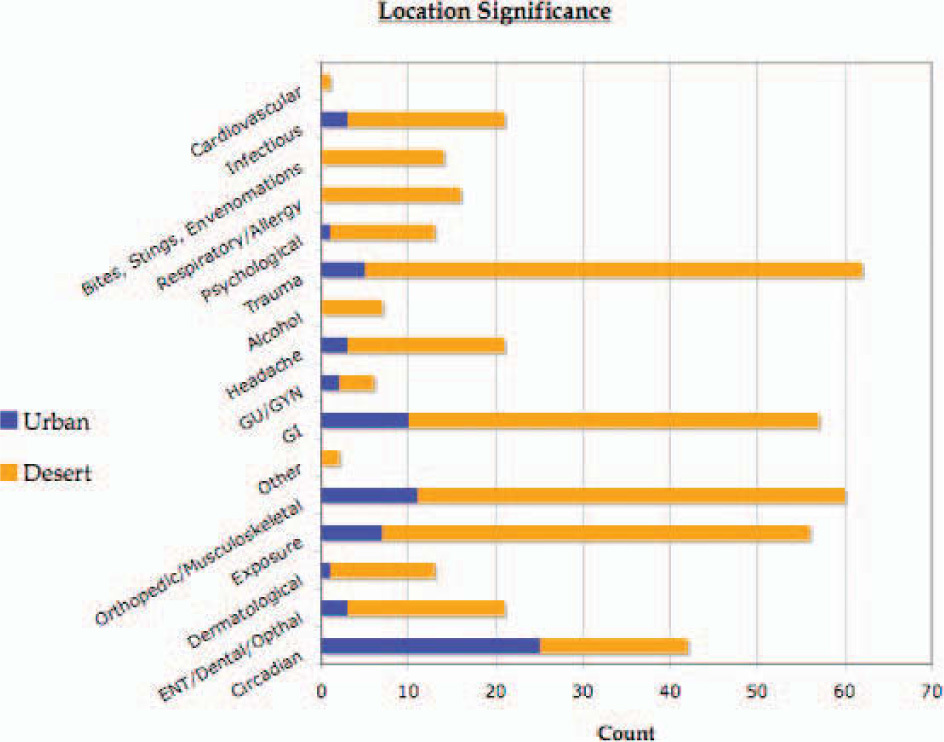
Nature of illness and injury by setting. Blue denotes urban setting, while burnt umber denotes the arid, wilderness setting.
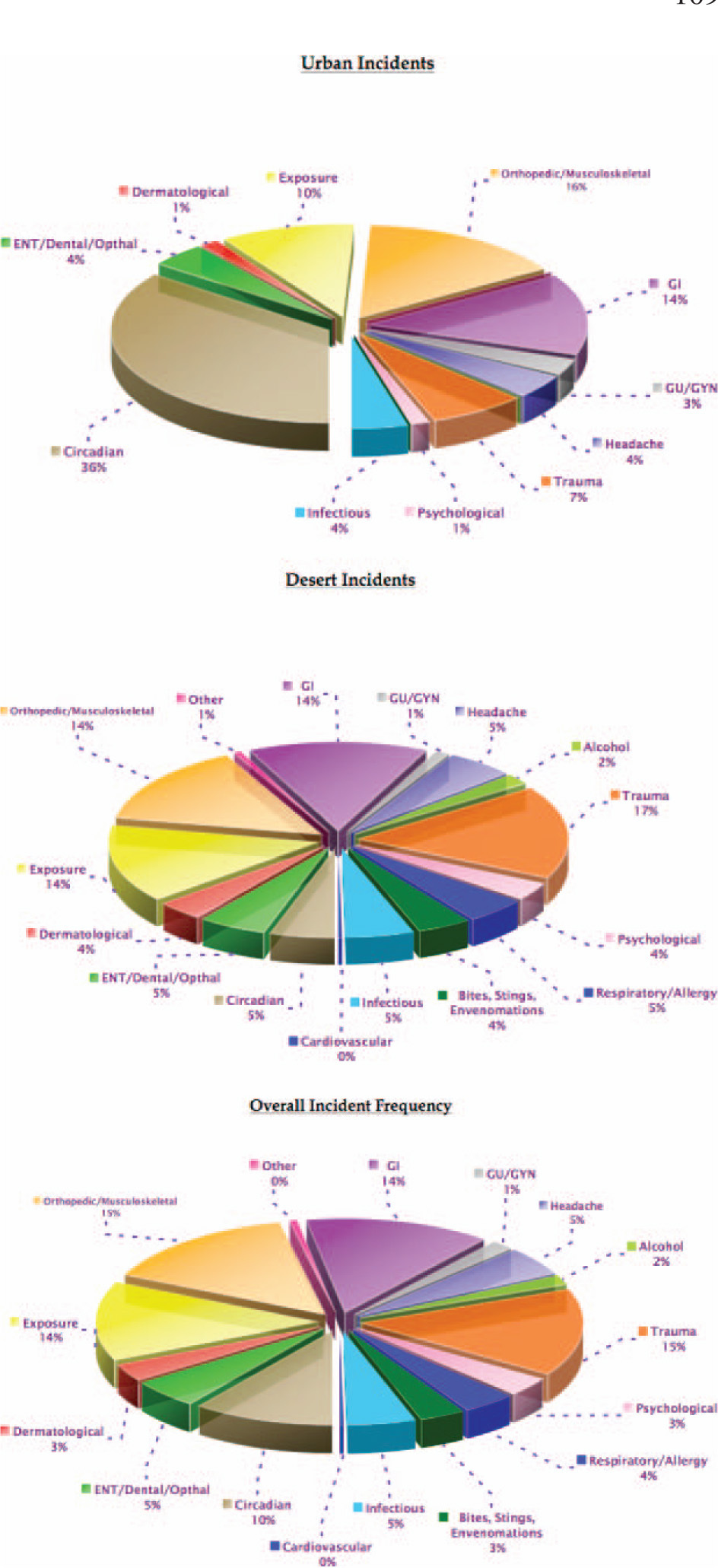
Pie graph describing each diagnosis by percent of total illness and injury in the urban and wilderness settings.
The chronology of medical illnesses was noteworthy for a rapid decline in circadian problems from the beginning onward, with a slight rise toward the end of the expeditions. Exposure-related illnesses were frequent at the outset of the expeditions, became more prominent toward the middle of the expeditions, and rapidly fell off toward the end of expeditions. Orthopedic and musculoskeletal complaints steadily rose throughout, while nonorthopedic traumatic injuries had their peak in the middle of the expeditions (Figure 3).
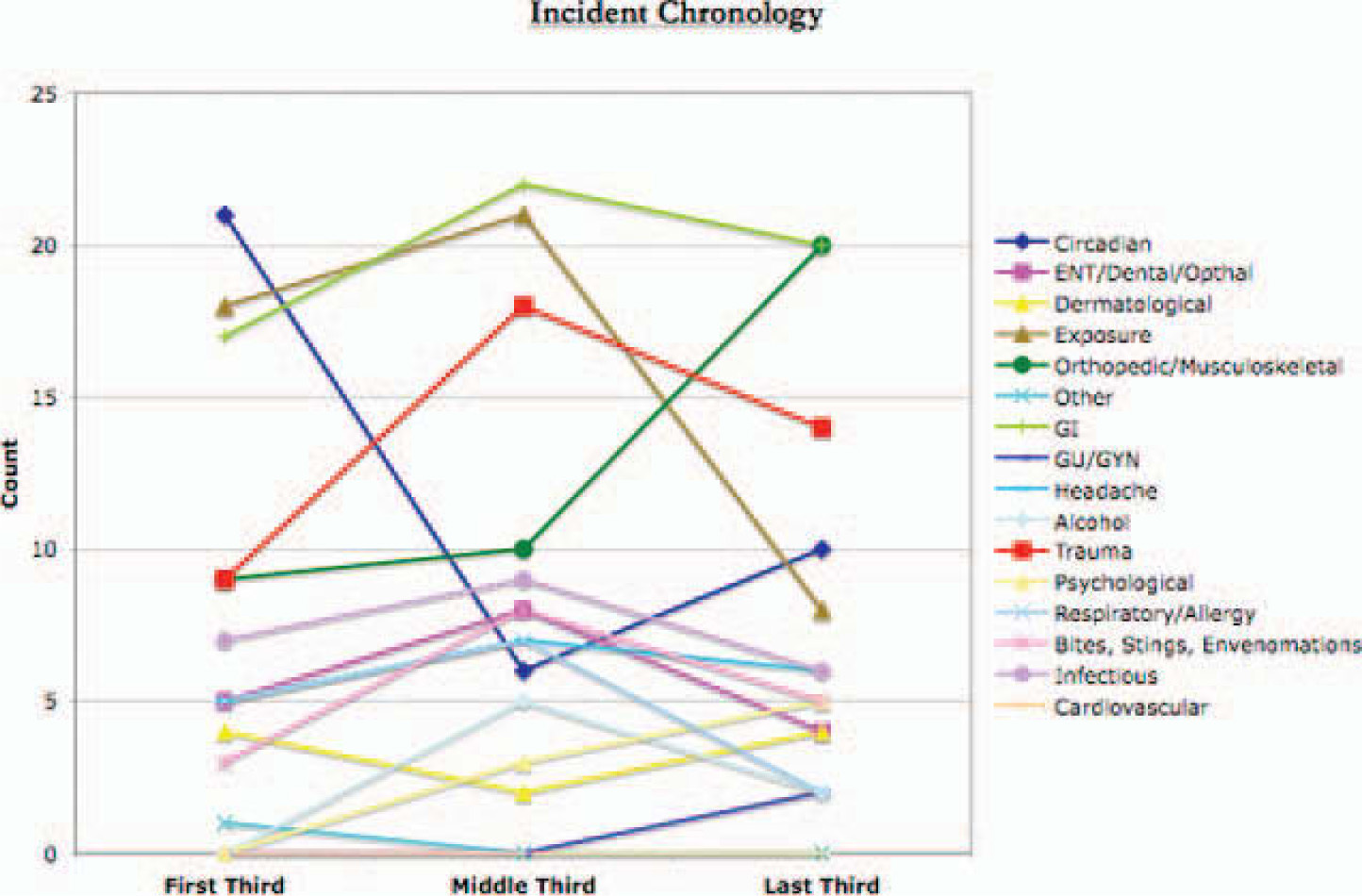
Incidences of various illnesses and injuries as a function of time during each expedition season. Expeditions varied in duration from 3 to 6 weeks.
The median age of the expeditioners was 36 years, ranging from 22 to 74 years. The average age was 39 years, and the standard deviation was 14 years. During the 6 seasons during which the study took place, 3 complaints brought to the attention of expedition physicians were not properly recorded and are not included in the study results. Additionally, events involving alcohol intoxication with or without fighting and with or without concomitant injuries were recorded as single encounters but separate injuries (eg, intoxicated and tripped over tent wire resulting in an abrasion was counted as 2 illnesses). These overlapping injuries accounted for less than 1.5% of the total number of encounters.
Discussion
During our analysis, we found 2 studies that should be compared to our results. One study looked at 7 years of data collected from an ongoing expedition to the Artic, but it differed strongly from our study in that it excluded events not requiring an MD level of care. 32 It did not give a frequency analysis of illness and injury. The other study, by Anderson and Johnson, 33 retrospectively analyzed medical incident data collected on a wide variety of expeditions over a period of years using a classification system resembling ours. This study was not specific to any one geographic setting.
Comparing results, Anderson and Johnson found an overall risk of 6.44 incidents per 1000 person-days, while we found a 20-fold greater risk at 153.2 incidents per 1000 person-days. To try and separate minor from major illnesses, their categories of “gastrointestinal” and “trauma” showed an absolute risk of 2.12 and less than 1.10 incidents per 1000 person-days, respectively, compared to our results of 21.2 and 23.1 incidents per 1000 person-days, respectively. A likely explanation for this discrepancy, which Anderson and Johnson provide, is the potential underreporting of less severe incidents in their study as a result of their use of retrospective self-reporting 6 months after the trip. Our study, in contrast, encouraged a low reporting threshold. A comparison of the percent frequency of illness and incidents shows “GI,” “orthopedic” (including “trauma”), and “environmental” categories composing 33%, 17%, and 14% of the total, respectively; our data showed that “GI,” “orthopedic,” “trauma,” and “exposure” composed 13.8%, 14.6%, 15.1%, and 13.6% of the total, respectively. Differences may result from the same reporting issues.
In our study, it should be noted that the majority of the complaints in the category “orthopedic/musculoskeletal” were back pain, and, moreover, these complaints were reported in patients with a prior history of back pain. Furthermore, the expedition members had access to alcohol during the expedition, which contributed to certain incidents in addition to those listed under the category “alcohol.”
In expedition planning, an understanding of the relative risks of each environment and consideration of the time spent in each should be considered. Native and foreign participants in expedition travel are at different risk for maladies such as diarrhea, whereas other illnesses and injuries may affect all participants at the same rate (although the threshold for complaining might be significantly different).
In our cohort of expeditioners transitioning between urban and rural environments, any increase in the incidence of illness or injury compared to their resident environment can be thought of as a travel-related risk. The altitude and geography of the Gobi Desert make its temperature fluctuations more extreme than would be encountered in other deserts, such as those at lower elevation. As with any environment, many flora and fauna of the Gobi Desert are unique to this location and are not found elsewhere. Consideration of the prevalence of and treatment for exposure to harmful or toxic flora and fauna, including pathogens and diseases, within a specific region should guide expedition medical supply planning. 20,21,34 –36
Limitations of our study include the fact that potentially significant complaints may have been missed as a result of underreporting. Conversely, having a physician on staff may have decreased the reporting threshold. Thus, there may be some selection biases. All members of the expeditions were briefed about the nature of our study on arrival and again just prior to departure to the desert. No member of any expedition declined to utilize physician services knowing that medical logs were being kept, although expedition members requested that a few select complaints not be recorded. Some expedition members brought medications from another physician to self-medicate. Finally, because our expeditions disbanded within 24 to 36 hours of return from the desert, no logs of postexpedition illnesses and injury exist. Interestingly, though, several illnesses and injuries were diagnosed weeks and even months after return from expeditions. For example, suspicion of tick-borne rickettsiosis after a clinical diagnosis of lymphoma with B-symptoms was the inspiration for our original study of the risk of acquiring R sibirica during scientific expeditions to Central Asia. 26 A persistently painful leg injury was diagnosed (by magnetic resonance imaging) as a deep bone contusion more than 2 months after return. A persistent, dermatophytic toenail infection not responding to fluconazole was confirmed to be Rhodotorula. 37 Thus, an unknown and probably significant number of expedition-related maladies were almost certainly missed. We are aware of one case of antibody-confirmed R sibirica following the 2007 season, but the diagnosis was made after data collection ended. Other incidents that occurred and might have resulted in harm were armed robbery of the expedition (as a group) and 3 separate robberies and attempted robberies in urban marketplaces between 2003 and 2007.
We observed that there are patterns of injury and illness that are consistent across expeditions to the Gobi Desert. For example, while heat- and wind-exposure– related illness and injury in the desert are quite common, other aspects of the desert environment are very forgiving. Our physicians encountered few incidences of Tinea cruris and other causes of itchiness and discomfort in the perineal, foot, and axillary regions that are commonly encountered in humid environments. 38 –40 This is likely a result of the rapid evaporative rates for water in arid, relatively high-altitude environments. Needless to say, every geographic region has unique hazards. Perhaps the most interesting finding in our cohort was the degree to which different problems occurred at different stages of the expeditions. Not surprisingly, sleep-related disturbances predominated during the early stages of travel. Nevertheless, other temporal patterns appear to be worthy of further investigation. Though preliminary, our data indicate several studies that could and should be carried out in order to develop more efficient medical kits and tools for predicting patterns of illness and injury during work and travel in arid environments such as the Gobi, Atacama, and Sahara Deserts. Such studies could analyze whether the risks we observed in the Gobi Desert are consistent across other arid environments. Additionally, studies could compare physician reporting vs self-reporting of incidents and could also compare reporting in physician-staffed expeditions to that in expeditions without a physician. Future findings could be an asset to recreational travelers and religious pilgrims as well as to those sending employees to extreme environments.
Footnotes
Acknowledgments
We wish to thank all members of these expeditions to the Gobi Desert for participating in our study and for their keen interest in advancing knowledge in the natural history of the earth as well as medicine. In addition, we thank the University of California, San Francisco School of Medicine Dean's Summer Research Fund (JET) and the American Museum of Natural History and the Smithsonian Institution Department of Vertebrate Paleontology for coordinating and funding these scientific expeditions and for allowing us to participate.