
Abstract
Objective
This study assessed a potential relationship between elevated carboxyhemoglobin (COHb) levels and the presence of acute mountain sickness (AMS) at 4300 m on Denali and evaluated the relationship between COHb levels, AMS, and climber characteristics and behaviors. Building on our research done in 2004, in this article we report further data gathered during the 2005 climbing season and evaluate the combined results.
Methods
Participants were screened for AMS using the Lake Louise Self-Report Questionnaire and answered questions focusing on AMS symptoms, AMS prevention, and previous history of altitude illness. Carboxyhemoglobin levels were measured by serum co-oximetry. Additional questions assessed stove practices, climbing practices, and climber behaviors. Nonparametric statistical analyses were performed to examine potential relationships between COHb levels, AMS symptoms, and climber behaviors across the 2 years and with years combined.
Results
Overall, 317 climbers participated in the 2-year study. As in 2004, the combined data demonstrated no relationship between positive carbon monoxide (CO) exposure and positive criteria for AMS (P = .276). Climbers in 2005 were 1.92 times more likely to meet positive criteria for AMS, compared to climbers in 2004 (P = .028). On the contrary, climbers in 2004 were 3.93 times more likely to be CO exposed than climbers in 2005 (P = .003). Overall, climbers descending the mountain were more likely to be positive for CO exposure (5.56 times more likely than ascending climbers, P = .002) and to have higher overall mean COHb levels (2.26% descending vs 0.93% ascending, P = .006). The previous association between increased stove use and climbers who met positive criteria for AMS was not observed in the 2005 or in the combined data (P = .715). A relationship was observed between increased hours of operating stoves and increased COHb levels (P = .002). Female climbers were 2.041 times more likely to meet criteria for AMS (P = .043).
Conclusions
No relationship between AMS symptoms and CO exposure was observed. As found in our initial study, descending climbers had higher overall COHb levels and an increased risk of CO exposure (COHb of >3% in nonsmokers and >10% in smokers). Also, increased hours of stove operation was linked to climbers who had elevated COHb levels.
Introduction
Anecdotal reports of carbon monoxide (CO) poisoning in mountaineers have been documented by the National Park Service (NPS) on Denali (Mt McKinley) for at least 20 years. 1 And from 1985 to present, up to 32% of all climbers on Denali have been treated annually for symptoms of acute mountain sickness (AMS). 2 Our research team investigated CO exposure and the potential relationship between CO toxicity and AMS in 146 climbers during the 2004 Denali climbing season and found no clear correlation between CO exposure and AMS. 3 However, 4 findings related to CO exposure were described by the 2004 research: 1) increased overall carboxyhemoglobin (COHb) levels were observed in descending climbers; 2) there was increased risk of CO exposure (COHb levels of >3% in nonsmokers or of >10% in smokers) while descending; 3) there was a relationship between positive criteria for AMS and increased stove use; and 4) there was a relationship between medication use and elevated COHb levels. 3 Additional data were gathered the following season in 2005, with an additional 171 climbers participating in the same study protocol.
We again hypothesized that elevated COHb is an identifiable risk factor for AMS. With a larger sample size and increased statistical power, we assessed 4 of the 5 significant findings described by the original research and examined the data for variables related to CO exposure and AMS, between years and with the 2 years combined.
Methods
This research project was reviewed and approved by the Human Subjects Review Committee of the Human Subjects Division of the University of Washington. Recruitment, consenting, and testing of climbers occurred per our 2004 research methods.
3
Participation was anonymous and voluntary. As in 2004, individuals were asked to participate in the study when they presented to the first-aid tent complaining of symptoms of AMS, or they were recruited into the study by researchers and were screened for AMS. The Lake Louise Acute Self-Report (LLSR) Questionnaire was used to evaluate participants for AMS (Appendix 1—available at
Participants were also asked 11 questions focusing on basic demographic data and climber behaviors that focused on potential CO exposure risk and individual risk for developing AMS (Appendix 2—available at
Participant COHb levels were again measured using the GEM OPL Oxygenation Portable Laboratory co-oximeter (Instrumentation Laboratory, Lexington, MA), analyzing approximately 0.3 mL of blood collected by venipuncture. Carboxyhemoglobin levels were recorded as a percent range of 0.1% to 75.0%. The operation of the co-oximeter took place inside the relatively stable environment of the NPS first-aid shelter at the 4300-m– high base camp. Optical quality control cuvettes were utilized before analysis of every blood sample to calibrate the instrument, maintaining a constant result reliability for samples analyzed.
Carboxyhemoglobin levels of >3% (nonsmoker) or >10% (smoker) were considered positive for CO exposure (values below these cutoffs were considered negative). Carboxyhemoglobin levels of >10% for nonsmokers and >20% for smokers were considered positive for CO intoxication. 6 –11
Data analysis
Using SPSS (Version 14, SPSS Inc, Chicago, IL), the same analytic strategy was employed as was detailed in our previous study. 3 With the exception of medication use, the same variables were used in both studies. The data from 2004 and 2005 were combined in order to test the study hypotheses and to increase the power of the statistical tests. Crosstabs, tests of differences between means, Spearman correlation analyses, and logistic regression models were performed for the AMS and CO exposure classification variables with all other study variables that could potentially contribute to positive CO exposure and/or AMS (climbing year, age, days ascending, hours operating stove, gender, smoking status, use of a heater, and ascending/descending status).
Results
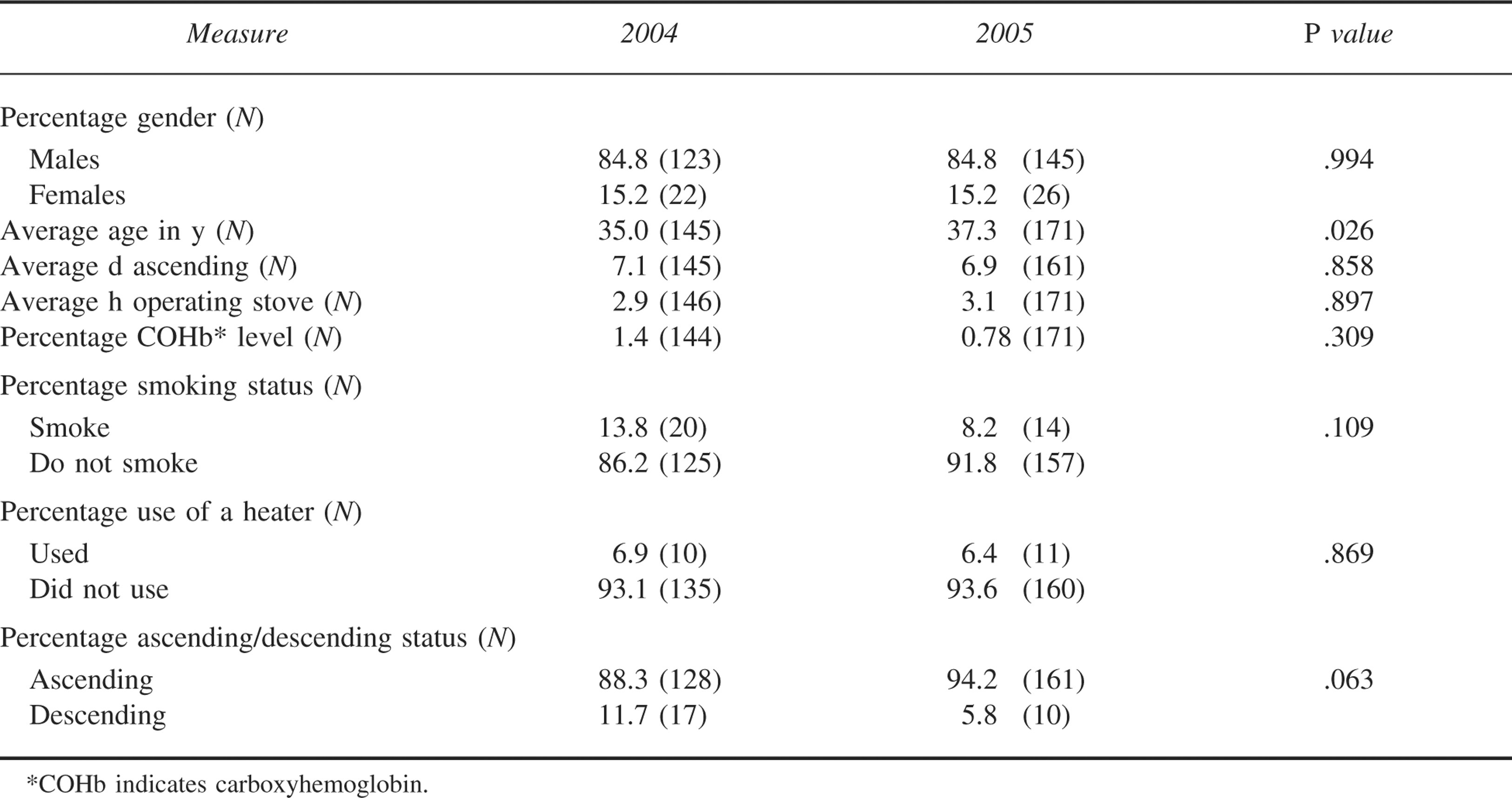
A total of 171 climbers were consented and enrolled and tested during May 2005. The total number of climbers participating over the 2 years was 317. Again in 2005, most participants were ascending the mountain. The median time to reach the 4300-m–high base camp was 6.9 days (compared to 7.1 days in 2004). All categorical and quantitative climber characteristics were similar between years, except for age (Table 1).
Climber characteristics across study years
Using the combined data, with their increased statistical power, 4 of the 5 associations observed in 2004 were again tested (medication use was not tested because it was not recorded in 2005). For the combined data, the findings are as follows.
No Relationship Between Co Exposure and Positive Criteria for AMS
Combined data upheld the null hypothesis, and no relationship was observed between positive CO exposure and positive criteria for AMS (Fisher exact test, P = .276). In addition, no relationship was observed between CO exposure and age, days ascending, gender, smoking status, or use of a heater. Also, no relationship was found between AMS and age, days ascending, hours operating a stove, smoking status, use of a heater, or ascending/descending status.
Increased COHb Levels and Increased CO exposure Risk in Descending Climbers
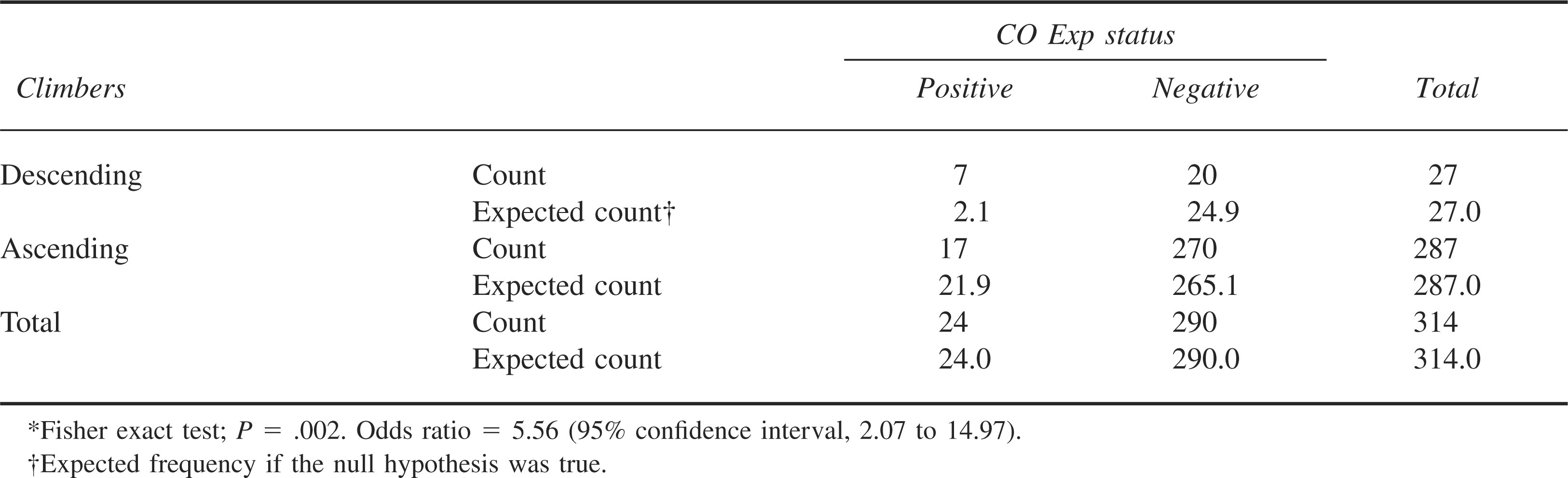
Mean overall COHb levels were higher in descending climbers (2.26% descending vs 0.93% ascending) (Mann-Whitney U test, P = .006). Climbers descending the mountain were again more likely to be positive for CO exposure (COHb levels of >3% in nonsmokers or of >10% in smokers) (Fisher exact test, P = .002). The combined data demonstrated that descending climbers were 5.56 times more likely to meet criteria for CO exposure than were ascending climbers (the 2004 data showed a similar risk, but at 3.6 times more likely than ascending climbers) (Table 2).
Descending/ascending climbers by carbon monoxide exposure (CO Exp) status*
No Relationship Between Increased Stove use and Positive Criteria for AMS
Our previous finding that increased stove use was noted for climbers who also met positive criteria for AMS was not upheld (t = −0.365, P = .715).
Other Notable Findings
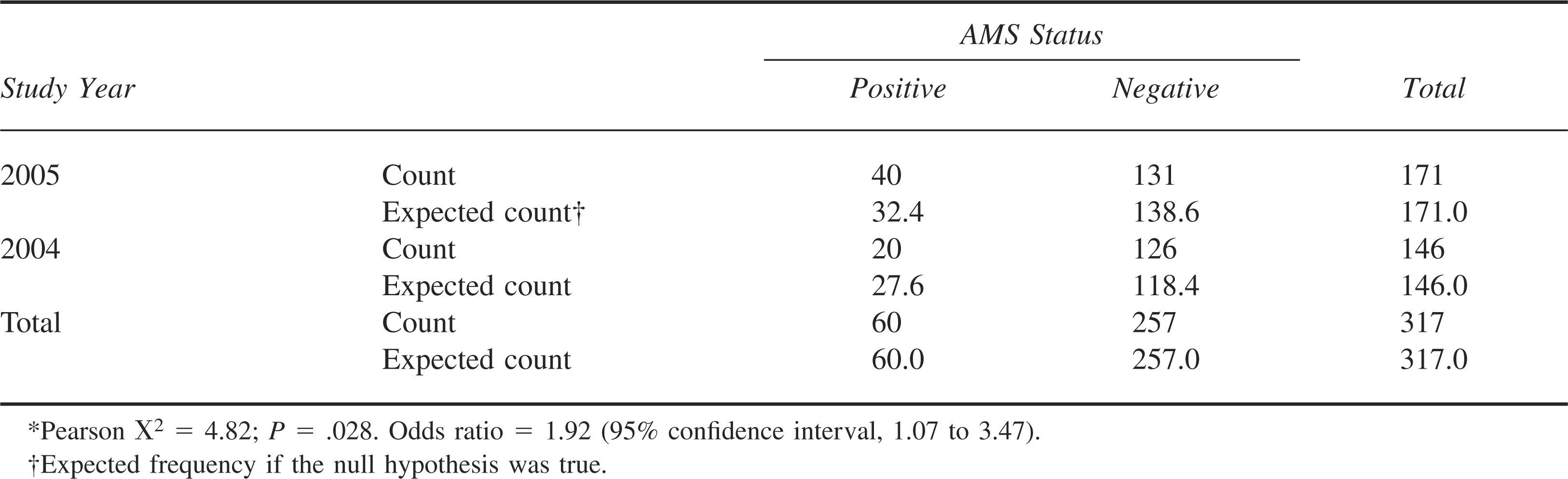
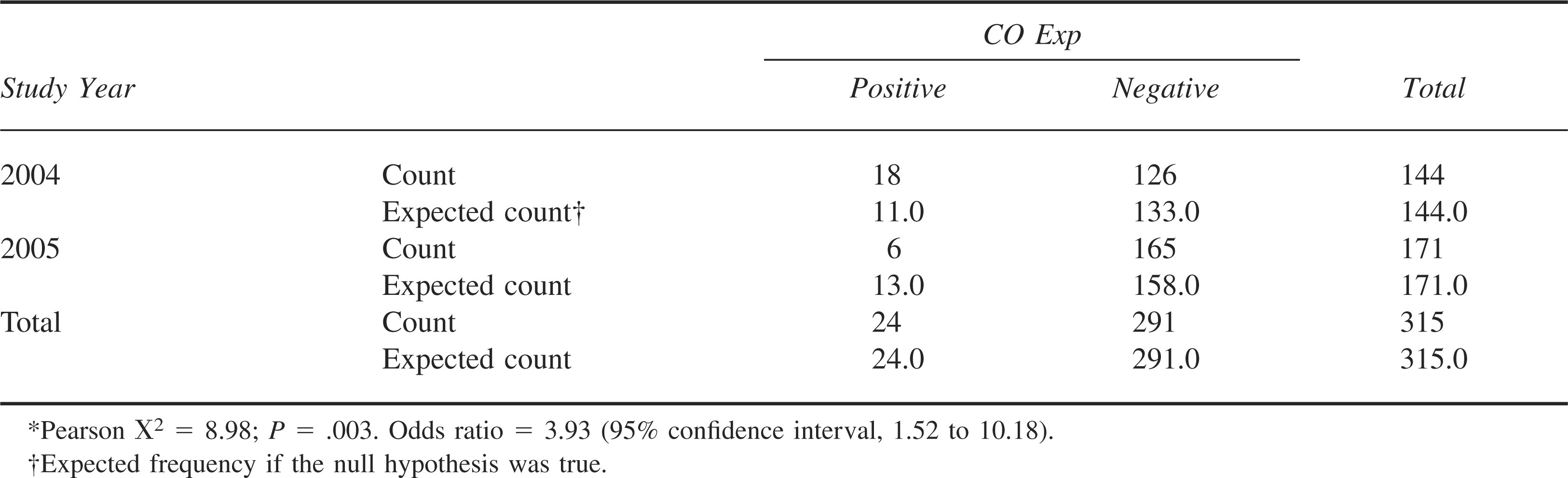
Climbers in 2005 were 1.92 times more likely to meet positive criteria for AMS, compared to climbers in 2004 (Pearson χ2 = 4.82, P = .028) (Table 3). On the contrary, climbers in 2004 were 3.93 times more likely to be CO exposed than climbers in 2005 (Pearson χ2 = 8.98, P = .003) (Table 4).
Study year by acute mountain sickness (AMS) status*
Study year by carbon monoxide exposure (CO Exp) status*
Analysis also demonstrated a relatively weak correlation (Spearman correlation) between the number of hours operating stoves and COHb levels during the 2005 season. Specifically, higher hours of stove use was associated with higher COHb levels (r = −177, P = .002). No climbers from either season met criteria for CO intoxication.
Also, in 2005, female climbers were observed to be 2.041 times more likely to meet criteria for AMS, as compared to men (Pearson χ2 = 4.103, P = .043). No additional relationships were found to be predictors of positive criteria for AMS or CO exposure. In addition, logistic regression models did not demonstrate any combination of variables that was a predictor of CO exposure or AMS besides the individual predictors identified (descending for CO exposure and gender for AMS status).
Discussion
With the increased power from the combined data, this research project found no relationship between symptoms suggestive of AMS and positive CO exposure in climbers on Denali (P = .276). The number of climbers with CO exposure and positive criteria for AMS was markedly different when data from the 2 study years were compared to one another, with CO exposure being more prevalent during the first study season. In contrast, CO exposure was lower in 2005 (3.5% vs 12.5% in 2004), and positive criteria for AMS was higher in 2005 (23.4% vs 13.7% in 2004). The differences in CO exposure across the 2 years indicate a predictable but previously undescribed weather effect that may influence CO exposure and AMS risk for climbers on Denali (ie, an increased risk for CO exposure in relatively poor weather and increased AMS risk in relatively good weather).
The potential weather effect on increased CO exposure risk correlates well to annual weather data collected by the NPS at the 2200-m Kahiltna base camp and at the 4300-m–high base camp. These data indicate increased precipitation, higher maximum wind speeds, and lower average temperatures in 2004 vs 2005, though we were unable to formally analyze these data as a result of inconsistencies in NPS weather data collection procedures over both years (Missy Smothers, Denali National Park and Preserve, Talkeetna Ranger Station, written communication, February 2007).
In theory, more climber time spent in tents waiting out foul weather may have led to improved acclimatization but increased CO exposure. In contrast, fair weather in 2005 may have led to shorter periods spent in shelters, resulting in the lower overall COHb levels observed in all climbers tested and in a lower number of climbers who met criteria for CO exposure. With better weather, one would also assume that climbers engaged in more rapid interval altitude gains, resulting in an increased risk for developing AMS. Although increased numbers of climbers reported symptoms consistent with AMS in 2005, the average time taken to reach the 4300-m base camp was similar to that reported in 2004 (6.9 days in 2005 vs 7.1 days in 2004). Increased rates of AMS in 2005 with similar average ascent times may have been due to climber characteristics not assessed by this study (ie, individual climber experience at altitude, the number of participants who were in guided groups, etc) and/or insufficient power of this study to accurately assess risk factors for AMS alone.
Combined data showed elevated COHb levels in descending climbers compared to ascending climbers and an increased risk of CO exposure while descending, now with an increased odds ratio (5.56 vs 3.6 in 2004). Following a successful ascent, alpine climbers can be motivated to get off a mountain as quickly as possible, possibly resulting in behaviors that may increase one's exposure to CO. Behaviors, including stove operation in unventilated areas (inside tents and vestibules), the use of continuous but poor ventilation rather than intermittent good ventilation, and decreased climber activity when not actually descending, may have contributed to increased CO exposure in descending climbers.6,12,13
The observations that descending climbers had higher overall mean COHb levels and more often met criteria for CO exposure may also support the possibility that high-altitude mountaineers may accumulate CO over time. Multiple factors, including a possible prolonged half-life for COHb at altitude, an additive hypoxic effect of COHb, increased endogenous CO production at altitude, a greater CO sink from altitude-induced polycythemia, and a progressive decrease in daily activity, all may contribute to high-altitude CO accumulation.1,7,14 Further research is needed to help answer questions related to CO exposure and possible chronic CO accumulation at altitude.
In 2004, a relationship between positive criteria for AMS and increased stove use was observed. This finding was of unclear significance, and it was hypothesized that increased stove use and increased CO exposure may be contributing to or mimicking symptoms of AMS.8,15 With the combined data set, this relationship was not upheld (P = .715), indicating that the initial findings were random secondary to small sample size and insufficient statistical power.
The stability of the relationship between medication use and elevated COHb levels observed in 2004, unfortunately, could not be assessed because medication use was not recorded in 2005. Any relationship between elevated COHb and use of medication to assist in acclimatization is likely complex and warrants additional investigation. 7
The predictable relationship between elevated COHb and increased stove use does support the fact that CO exposure remains a potential risk for high-altitude mountaineers. That said, this research team would have expected a more robust relationship between increased stove use and CO exposure considering the occasionally risky stove-use practices employed by climbers (ie, operating a stove inside a ventilated tent, sealed vestibule, or even a sealed tent). The true danger of CO exposure from portable cook stoves, especially when ‘risky stove-use practices’ are employed, remains unclear. One must also consider that the danger of cooking in less-than-adequately ventilated settings may not pose as serious a physiologic risk as is commonly perceived by climbers and wilderness medical providers and as described by controlled research focused on this topic.8,12,13 Human thresholds may be quite high for development of symptoms from CO exposure when at altitude, or elevated COHb levels may be highly transient. Obviously, further investigations, especially in field settings, are needed to better define the CO exposure risk associated with portable cook stove operation.
Female climbers participating in this research project were about 2 times more likely to meet positive criteria for AMS than were men. This finding is relatively unique, and published scientific literature on AMS and gender largely supports the idea that there is no gender difference or that there is a decreased susceptibility to developing AMS in women. 16 –18 The relationship of AMS risk and gender observed in this study may represent a new relationship between susceptibility to AMS and female gender; it also may be due to the inadequate power of this study to assess this relationship. The majority of participants in this study were male (only 15% of participants overall, and year-to-year, were female), and the mountaineering experience of participants, which could play a positive or negative role in a climber developing symptoms of AMS, was not assessed. With very little evidence available in the scientific literature focusing on gender and the risk of developing symptoms of AMS, this area certainly deserves to be studied further.
There are several potential limitations to this study. Inaccurate readings by the portable co-oximeter could have occurred as a result of the variable and extreme natural environment at 4300 m on Denali, leading to inaccurate measurements of COHb levels. Also, per conversations with Instrumentation Laboratory Inc, the GEM OPL co-oximeter had not been evaluated for performance at high altitude. The research project did not determine when participants had last operated a stove, only how many hours they had operated one in the last day. Because of the short half-life of COHb and the random recruiting of participants into the study, individuals may have had higher COHb levels before or after being tested. Because many climbers routinely do not seek care for mild symptoms of AMS, additional symptomatic, CO-exposed subjects may have been missed, resulting in underreporting of elevated COHb levels in the population tested. As well, symptoms for the LLSR and all demographic information were self-reported and subject to recall bias. Finally, the percent values of COHb used in this study to define CO exposure and toxicity were based on several published studies detailing CO exposure; the absolute cutoffs for exposure and toxicity in these studies were variable, and all studies reviewed were conducted at elevations far lower than 4300 m. Taking into account the high-altitude setting of this research (and the lower atmospheric pressures encountered), levels for CO exposure may in fact be lower than the values used by this study, leading to an underdiagnosis of CO exposure in the population studied.
The findings of these 2 projects, the first of their kind to assess COHb in climbers at altitude, clearly demonstrate that CO exposure does occur in the high-altitude wilderness setting and is greatest while climbers are descending Denali. Weather may also play a role in the risk of developing AMS and CO exposure, with a greater risk for CO exposure occurring when weather conditions are poor and a greater risk for AMS occurring when conditions are fair. The findings of this project have been presented to the Denali NPS, with hopes that it will help mountaineers better understand their risks for CO exposure while climbing, allowing them to more safely accomplish their objectives at high altitude.
Footnotes
Acknowledgments
The authors thank Ted Epperly, MD, and the Family Medicine Residency of Idaho for technical support; Rob Hilvers, MD, and Rocky Mountain Wilderness Medicine for technical support; Kemala Thompson and Instrumentation Laboratory Inc for assisting with the co-oximeter; Lucy Tyrell and the Denali National Park and Preserve for technical support on Denali; and Lyn O’Doran and the Human Subjects Division of the University of Washington for assistance with the institutional review board (IRB) application. For assistance on the mountain and input on the design and implementation of this research project, the authors would also like to acknowledge Tor Anderson; Peter Hackett, MD; Robert Schoene, MD; Meg Purdue; Lance Taysom, RN; Mike Ross, MD; John Evans; the Denali National Park Climbing Rangers and the Park Rangers based at the Talkeetna Ranger Station; Neva Santos and the Idaho Academy of Family Practitioners; Dana Design and K2 Sports Inc; and MSR Inc. The authors acknowledge grants from the following organizations: Equipment grant—Instrumentation Laboratory Incorporated, Lexington, MA; Research grant—Rocky Mountain Wilderness Medicine, Boise, ID; Research grant—Idaho Academy of Family Practitioners, Boise, ID; Equipment grant—K2 Incorporated, Vashon Island, WA.